PT-141: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Bremelanotide, Vyleesi (brand name), PT 141, MTPT-141
Attribute
Administration
- Detail
- Injectable (subcutaneous); auto-injector (Vyleesi); nasal spray (unregulated, variable bioavailability)
Attribute
Research Status
- Detail
- FDA-approved as Vyleesi for HSDD in premenopausal women (2019). Off-label use in men is not FDA-approved.
Attribute
Typical Dose Range
- Detail
- 500-1750 mcg per dose (on-demand); 1750 mcg (1.75 mg) is the FDA-approved dose
Attribute
Half-Life
- Detail
- Approximately 2-2.7 hours
Attribute
Cycle Length
- Detail
- On-demand use; no traditional cycling. Max 1 dose per 24 hours, max 8 doses per month.
Attribute
Storage
- Detail
- Lyophilized: -20C or below; Reconstituted: 2-8C, use within 1-4 weeks
Overview / What Is PT-141?
The Basics
PT-141, known by its pharmaceutical name bremelanotide and sold under the brand Vyleesi, is a synthetic peptide that enhances sexual desire by acting directly on the brain. Unlike medications such as sildenafil (Viagra) or tadalafil (Cialis) that work by increasing blood flow to the genitals, PT-141 targets melanocortin receptors in the hypothalamus, the region of the brain that governs arousal and sexual motivation. The result is an increase in genuine desire rather than simply an improved physical response.
The compound was discovered by accident. In the 1990s, researchers at the University of Arizona were studying Melanotan II, a tanning peptide, when they observed unexpected and pronounced sexual arousal in study participants. That finding launched a separate line of research that eventually produced PT-141, a modified version of Melanotan II engineered to retain the sexual desire effects while minimizing the tanning activity [1].
In 2019, the FDA approved bremelanotide (as Vyleesi) for the treatment of hypoactive sexual desire disorder (HSDD) in premenopausal women, making it the first centrally-acting medication approved specifically for sexual desire [2]. It is administered as a subcutaneous injection approximately 45 minutes before anticipated sexual activity. While not approved for men, clinical studies have shown efficacy for male erectile dysfunction, particularly in cases where PDE5 inhibitors have failed [3].
The most commonly reported side effect is nausea, occurring in approximately 40% of users. This is dose-dependent and tends to diminish with repeated use [2].
The Science
PT-141 (bremelanotide; Ac-Nle-c[Asp-His-D-Phe-Arg-Trp-Lys]-OH) is a synthetic cyclic heptapeptide melanocortin receptor agonist with preferential activity at MC3R and MC4R [1][3]. It is structurally derived from Melanotan II through deamination of the C-terminal, resulting in reduced MC1R binding (and therefore reduced melanogenic activity) while preserving central nervous system effects on sexual arousal pathways [4].
The compound was developed following observations by Wessells and colleagues during MT-II tanning studies, where male subjects exhibited spontaneous erectile responses and increased sexual desire [5]. Subsequent pharmacological optimization produced bremelanotide, which received FDA approval in June 2019 based on the RECONNECT Phase 3 trials (n=1,267 premenopausal women with HSDD) [2].
The central mechanism of action distinguishes PT-141 from all other approved sexual dysfunction therapies. PDE5 inhibitors (sildenafil, tadalafil, vardenafil) act peripherally on the nitric oxide/cGMP pathway in penile corpus cavernosum smooth muscle. PT-141 acts centrally on MC4R in the medial preoptic area (mPOA) and paraventricular nucleus (PVN) of the hypothalamus, brain regions that regulate sexual behavior across both sexes [6]. This mechanistic distinction explains PT-141's efficacy in PDE5 inhibitor non-responders with psychogenic erectile dysfunction [3][5].
Molecular Identity
Attribute
Amino Acid Sequence
- Detail
- Ac-Nle-c[Asp-His-D-Phe-Arg-Trp-Lys]-OH
Attribute
Molecular Formula
- Detail
- C50H68N14O10
Attribute
Molecular Weight
- Detail
- 1025.18 g/mol
Attribute
CAS Number
- Detail
- 189691-06-3
Attribute
PubChem CID
- Detail
- 9941379
Attribute
Structure Type
- Detail
- Cyclic heptapeptide with 2-7 lactam bridge, N-terminal acetylation
Attribute
Key Modification
- Detail
- D-Phe at position 4 of cyclic core; C-terminal free acid (vs. amide in MT-II)
Attribute
Origin
- Detail
- Synthetic; deaminated metabolite-derivative of Melanotan II
Attribute
Receptor Selectivity
- Detail
- MC4R >> MC3R > MC1R (reduced MC1R vs. MT-II)
Mechanism of Action
The Basics
Most medications for sexual dysfunction work by improving the physical mechanics of arousal, essentially increasing blood flow to the genitals. PT-141 takes a fundamentally different approach. It works in the brain, targeting the neural pathways that generate the feeling of wanting sex in the first place.
Think of it like this: if PDE5 inhibitors (Viagra, Cialis) are turning up the volume on a speaker, PT-141 is turning on the radio station. The speaker can be as loud as it wants, but if nothing is playing, there is no music. PT-141 activates the signal itself, the desire that drives arousal, rather than amplifying the downstream physical response.
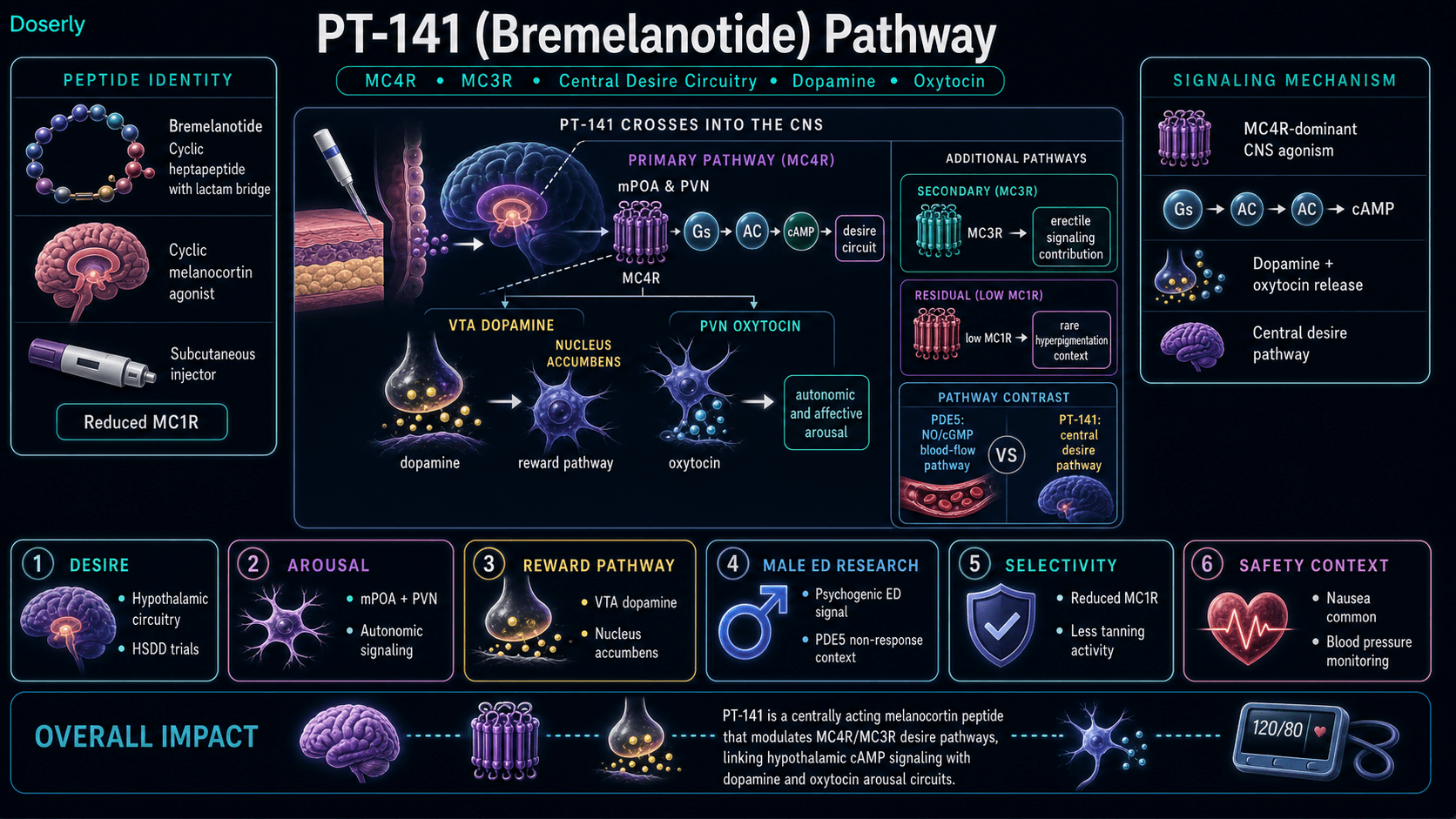
It does this by binding to melanocortin receptors (specifically MC4R) in the hypothalamus, a brain region that acts as a control center for sexual behavior. When PT-141 activates these receptors, it triggers a cascade that increases dopamine and oxytocin release, both of which are intimately involved in desire, arousal, and the experience of sexual pleasure [6].
This central mechanism is why PT-141 can work for people whose sexual difficulties are rooted in low desire, stress, hormonal changes, or psychological factors, even when medications that target blood flow alone have not helped.
The Science
Bremelanotide exerts its effects through agonism at melanocortin-3 and melanocortin-4 receptors (MC3R/MC4R) in the central nervous system [1][3].
MC4R activation (primary mechanism): MC4R is densely expressed in the medial preoptic area (mPOA) and paraventricular nucleus (PVN) of the hypothalamus, brain regions established as key regulators of sexual behavior in both sexes. MC4R activation triggers Gs-coupled adenylyl cyclase signaling, increasing intracellular cAMP, which drives dopamine release in the nucleus accumbens and mesolimbic reward circuits [6]. Concurrent oxytocin release from the PVN modulates the autonomic and affective components of sexual arousal [4].
MC3R modulation (secondary): MC3R contributes to energy homeostasis and may play a modulatory role in erectile signaling, though its contribution to PT-141's sexual effects is less characterized than MC4R [4].
MC1R interaction (reduced): Unlike Melanotan II, PT-141 has reduced affinity at MC1R (the melanocyte-stimulating receptor), minimizing melanogenic side effects. Some residual MC1R activity explains the occasional skin hyperpigmentation reported with repeated use [4].
Gender-independent mechanism: The hypothalamic circuitry targeted by PT-141 is functionally conserved between sexes, which explains the compound's demonstrated efficacy in both women (RECONNECT trials, FDA-approved) [2] and men (Phase II erectile dysfunction studies) [3][5]. This central mechanism operates independently of peripheral vascular status, distinguishing PT-141 from PDE5 inhibitors that require intact vascular nitric oxide signaling.
No tachyphylaxis: Clinical trial data from the 52-week open-label extension showed sustained or increasing efficacy with repeated use, with no evidence of tolerance development [7].
Pathway Visualization
Pharmacokinetics
The Basics
PT-141 has a relatively short active window in the body. After a subcutaneous injection, it reaches its peak concentration in about one hour and is largely cleared within a few hours. The recommended timing of 45 minutes before anticipated activity is based on this absorption profile [2].
However, many users report that the effects last considerably longer than the peptide's presence in the bloodstream would suggest. The pharmacological effects on desire and arousal can persist for 6 to 24 hours or even longer in some individuals. This disconnect between how quickly the peptide clears the blood and how long the effects last is because PT-141 triggers downstream signaling cascades (dopamine and oxytocin release) that continue even after the peptide itself has been metabolized.
The subcutaneous route provides essentially complete absorption and is better tolerated than intranasal delivery, which was explored in earlier development but abandoned due to inconsistent absorption and blood pressure concerns [3].
The Science
Following subcutaneous administration of 1.75 mg, bremelanotide reaches peak plasma concentration (Tmax) within approximately 1 hour [2]. The elimination half-life is approximately 2.7 hours, with hepatic metabolism and renal excretion as the primary clearance pathways [4].
Parameter
Route
- Value
- Subcutaneous injection
Parameter
Tmax
- Value
- ~1 hour
Parameter
Elimination half-life
- Value
- ~2.7 hours
Parameter
BBB penetration
- Value
- Yes (cyclic structure and lipophilic features confer CNS penetration)
Parameter
SC bioavailability
- Value
- Approximately 100%
Parameter
Intranasal bioavailability
- Value
- Variable, unquantified (formulation abandoned)
Parameter
Oral bioavailability
- Value
- Negligible
Parameter
Duration of pharmacodynamic effect
- Value
- 2-6 hours (clinical); up to 24-48 hours (community reports)
The pharmacodynamic effect duration significantly exceeds the pharmacokinetic half-life because MC4R activation triggers sustained downstream neuromodulatory cascades, including prolonged dopamine tone in the mesolimbic pathway and oxytocin release from the PVN, both of which have independent temporal dynamics from the parent peptide's clearance [6].
The half-life and clearance data above tells you how long the compound stays active, but what does that mean for your daily schedule? Doserly's pharmacokinetic tools let you plug in your dose and frequency to see a projected concentration timeline, helping you understand when you're at peak levels and when the compound has largely cleared.
This becomes especially useful when titrating. If you're increasing your dose gradually, the estimator shows how each step changes your projected peak and trough levels, giving you and your healthcare provider concrete data to discuss at check-ins rather than relying on subjective feel alone.
See where a dose, cycle, or change fits in time.
Doserly gives each protocol a timeline so dose changes, pauses, restarts, and observations are easier to compare later.
Timeline
Cycle history
Timeline tracking helps with recall; it is not a treatment recommendation.
Research & Clinical Evidence
Female Hypoactive Sexual Desire Disorder (FDA-Approved Indication)
The Basics
The strongest clinical evidence for PT-141 comes from the RECONNECT trials, two large Phase 3 studies that led to FDA approval. These studies enrolled 1,267 premenopausal women diagnosed with hypoactive sexual desire disorder (HSDD), a condition characterized by persistently low sexual desire that causes significant personal distress [2].
Over 24 weeks, women who received PT-141 (1.75 mg subcutaneously, as needed before sexual activity) showed statistically significant improvements in both sexual desire and reduction in distress related to low desire, compared to the placebo group. About 25% of treated women achieved what researchers defined as a clinically meaningful improvement [2].
A 52-week extension study showed that benefits were sustained or even increased with continued use. Desire scores climbed higher than in the initial 24-week trial, and distress continued to decrease, with no new safety concerns emerging over the full year [7].
The Science
The RECONNECT program comprised two randomized, double-blind, placebo-controlled Phase 3 trials enrolling 1,267 premenopausal women with generalized acquired HSDD. Participants self-administered bremelanotide 1.75 mg subcutaneously on an as-needed basis, at least 45 minutes before anticipated sexual activity [2].
Primary endpoints at 24 weeks showed statistically significant improvement versus placebo: Female Sexual Function Index-Desire (FSFI-D) domain score increased by +0.35 (P<0.001), and Female Sexual Distress Scale-Desire/Arousal/Orgasm (FSDS-DAO) Item 13 decreased by -0.33 (P<0.001) [2]. The responder rate (clinically meaningful improvement) was approximately 25% versus placebo [2].
The 52-week open-label extension (n=272) demonstrated sustained or increasing efficacy: FSFI-D improvements of +1.25 to +1.30 from baseline and FSDS-DAO reductions of -1.4 to -1.7, with no new safety signals [7]. These improvements exceeded the core trial's placebo-controlled effects, though the open-label design precludes attribution to pharmacology alone.
The most common adverse event was nausea (40.0% vs. 1.3% placebo), leading to discontinuation in approximately 9.1% of treated patients [2].
Male Erectile Dysfunction
The Basics
PT-141 has been studied in men with erectile dysfunction, though it is not FDA-approved for this use. The most compelling finding is that it appears to work through a different pathway than standard ED medications, making it potentially useful for men who have not responded to Viagra or Cialis [3][5].
In small but well-designed crossover studies, 8 out of 10 men with psychogenic (stress or anxiety-related) erectile dysfunction developed clinically apparent erections after PT-141 administration. The effects were significantly different from placebo, and increased sexual desire was reported after 68% of PT-141 doses compared to only 19% of placebo doses [5].
However, a subsequent study in men with organic (vascular) erectile dysfunction showed reduced efficacy, suggesting that PT-141's brain-based mechanism is most effective when the underlying issue is psychological rather than vascular in nature [3].
The early intranasal formulation used in male studies was eventually abandoned due to concerns about blood pressure increases. The subcutaneous formulation has a more favorable safety profile regarding blood pressure [3].
The Science
Wessells and colleagues conducted small crossover studies (n=10-20) in men with psychogenic erectile dysfunction demonstrating that 8 of 10 subjects developed clinically apparent erections after subcutaneous PT-141 administration, with mean penile tip rigidity exceeding 80% for 38 minutes versus 3 minutes on placebo (P=0.0045) [5]. Increased sexual desire was reported after 68% of PT-141 doses versus 19% of placebo doses [5].
A subsequent study in men with organic (vascular) erectile dysfunction demonstrated reduced efficacy, consistent with PT-141's central mechanism of action being most effective in the absence of peripheral vascular pathology [3].
Diamond and colleagues (2004) established dose-dependent efficacy across 0.3-10 mg subcutaneous and intranasal administration routes in an IJ-IMPOTENCE study [3]. The intranasal formulation was abandoned following safety concerns regarding transient blood pressure elevations observed with the nasal delivery route.
Phase II trials in men for erectile dysfunction were initially discontinued due to blood pressure concerns with intranasal dosing, though subcutaneous administration has since resumed clinical investigation with an improved safety profile [3].
Neurobiology of Sexual Desire
The Basics
Research into how PT-141 works at the brain level has revealed that it directly stimulates dopamine release in brain regions associated with pleasure and motivation. This is fundamentally different from how SSRIs (antidepressant medications) work, which can actually suppress sexual desire as a side effect. PT-141 operates on the excitatory side of the equation, amplifying the brain's natural wanting signals rather than manipulating serotonin pathways [6].
Importantly, studies have not shown evidence of addiction or tolerance development. The brain does not appear to become dependent on PT-141 to maintain normal sexual function, and stopping use does not produce withdrawal effects [6][7].
The Science
Neurobiological characterization of bremelanotide has established that MC4R activation in the mPOA drives dopamine release through mesolimbic circuitry, specifically in the nucleus accumbens, a key node in the brain's reward and motivation network [6]. This dopaminergic mechanism is independent of and complementary to the serotonergic pathways targeted by flibanserin (Addyi), the other FDA-approved HSDD treatment.
Preclinical c-Fos mapping studies in rats and primates confirmed hypothalamic activation following PT-141 administration, with activation patterns consistent with sexual arousal circuitry [3]. The 52-week extension data showing no tolerance development [7] is consistent with the intermittent, on-demand dosing paradigm, which avoids the receptor desensitization that might occur with chronic daily agonist exposure.
Biomarker Evidence Matrix
Category
Libido
- Evidence Strength
- 9/10
- Reported Effectiveness
- 8/10
- Summary
- Phase 3 RCTs (n=1,267) with FDA approval for HSDD. 66% positive on Drugs.com (41 reviews, avg 7.2/10). Strong, consistent community signal across multiple platforms.
Category
Sexual Function
- Evidence Strength
- 7/10
- Reported Effectiveness
- 7/10
- Summary
- Phase II crossover studies in men (n=10-20, P=0.0045). Enhanced physical arousal in both sexes. Community reports of superior erectile response vs. PDE5 inhibitors. Anhedonia risk (~30% of male users) limits score.
Category
Nausea & GI Tolerance
- Evidence Strength
- 8/10
- Reported Effectiveness
- 3/10
- Summary
- Phase 3 data: 40% nausea, 9.1% discontinuation. 51.2% Drugs.com nausea mentions. Universally discussed as dominant side effect in community.
Category
Side Effect Burden
- Evidence Strength
- 7/10
- Reported Effectiveness
- 4/10
- Summary
- Well-characterized from Phase 3 trials: nausea, flushing (7.3%), headache (9.8%), transient BP increase. Anhedonia reported in community.
Category
Mood & Wellbeing
- Evidence Strength
- 2/10
- Reported Effectiveness
- 6/10
- Summary
- No direct evidence for mood effects. Community positivity likely driven by improved sexual satisfaction (psychosocial, not pharmacological).
Category
Blood Pressure
- Evidence Strength
- 6/10
- Reported Effectiveness
- 4/10
- Summary
- Transient systolic rise of 10-15 mmHg documented in clinical studies. Intranasal formulation abandoned due to BP concerns. SC route safer but still monitored.
Category
Temperature Regulation
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Flushing documented in clinical trials and community (7.3% on Drugs.com). Transient, diminishes with use.
Category
Skin Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- Residual MC1R activity from MT-II derivation. Rare, mild hyperpigmentation with repeated use. Less than parent compound.
Category
Treatment Adherence
- Evidence Strength
- 3/10
- Reported Effectiveness
- 6/10
- Summary
- On-demand model well-received. Injection ease noted. Onset variability (2-8 hours) creates scheduling challenges.
Category
Emotional Aliveness
- Evidence Strength
- 2/10
- Reported Effectiveness
- 5/10
- Summary
- Split signal: some report feeling "alive," others report anhedonia. Insufficient data for directional conclusion.
Benefits & Potential Effects
The Basics
The primary benefit that brings people to PT-141 is enhanced sexual desire. For individuals experiencing low libido, whether due to hormonal changes, stress, medication side effects, aging, or diagnosed HSDD, PT-141 offers a fundamentally different approach from the blood-flow-focused medications that dominate the sexual health landscape.
Users commonly describe the experience as a return to a more natural, spontaneous sense of desire rather than a forced physical response. Reports of "feeling like a teenager again" are common in community discussions, reflecting the peptide's action on the brain's desire circuitry rather than peripheral blood vessels.
Beyond desire itself, improved physical arousal, enhanced sensitivity, stronger orgasms, and increased sexual confidence are frequently reported effects. These benefits appear to be sex-independent, with both women and men reporting improvements across multiple dimensions of sexual function.
For some users, there are secondary benefits in relationship quality and emotional wellbeing that stem from restored sexual connection with partners. Several community reports describe PT-141 as transformative for relationships that had been strained by mismatched desire levels.
The Science
The documented and reported effects of PT-141 can be categorized by their mechanistic basis and evidence quality:
MC4R-mediated effects (central, well-evidenced):
- Enhanced sexual desire: Demonstrated in Phase 3 RCTs (RECONNECT, n=1,267) with statistically significant FSFI-D improvements (P<0.001) [2]. Sustained at 52 weeks [7].
- Improved erectile function: Phase II data showing 80% of psychogenic ED patients achieving functional erections (P=0.0045) [5].
- Increased arousal and sensitivity: Reported across both sexes in clinical trials and community [2][3].
- Enhanced dopamine-mediated motivation: Neurobiological studies confirm mesolimbic dopamine release through MC4R-mPOA pathway [6].
MC3R-mediated effects (central, modest evidence):
- Contribution to erectile signaling (less characterized than MC4R pathway) [4].
MC1R-mediated effects (peripheral, residual):
- Mild hyperpigmentation with repeated use (reduced relative to Melanotan II) [4].
Side Effects & Safety Considerations
The Basics
PT-141 has a well-characterized side effect profile, with nausea being the standout concern. Approximately 40% of users in clinical trials experienced nausea, making it the most commonly reported adverse effect [2]. The nausea is dose-dependent, tends to diminish with repeated use, and can often be managed with anti-nausea medication (many community members recommend ondansetron/Zofran taken about an hour before PT-141).
Flushing (facial warmth, redness, a "wave" of heat) occurs in the first 30-90 minutes after injection and is typically mild and transient. Headache is reported by roughly 10% of users. Both effects tend to diminish over time.
Blood pressure increases are a known concern. Clinical data shows transient systolic rises of 10-15 mmHg that can last up to 12 hours. The earlier intranasal formulation was abandoned specifically because of more pronounced blood pressure effects. The subcutaneous route has a more favorable profile, but individuals with uncontrolled hypertension should not use PT-141 [4].
Sexual anhedonia, the inability to experience sexual pleasure despite physical arousal, is a concerning adverse effect reported by community users, particularly men at higher doses. This effect is not prominently featured in clinical trial data but appears in multiple independent community reports. Some users describe it as lasting weeks to months after discontinuation.
Contraindications include uncontrolled hypertension, cardiovascular disease, concurrent use of naltrexone, pregnancy (abortifacient potential), and history of hypersensitivity to bremelanotide [4].
The FDA label limits use to no more than one dose per 24 hours and no more than 8 doses per month [2].
The Science
Common adverse effects from Phase 3 data (RECONNECT trials) [2]:
- Nausea: 40.0% vs. 1.3% placebo (dose-dependent; leading cause of discontinuation at 9.1%)
- Flushing: 20.3% vs. 1.3% placebo
- Headache: 11.3% vs. 1.9% placebo
- Injection site reactions: 5.4% vs. 3.3% placebo
Cardiovascular effects [4]:
- Transient blood pressure elevation: systolic rise up to 10-15 mmHg, diastolic rise up to 5-8 mmHg, lasting up to 12 hours post-dose
- Transient decrease in heart rate
- The intranasal formulation produced more pronounced cardiovascular effects and was abandoned during development [3]
Dermatologic effects [4]:
- Focal hyperpigmentation with repeated use (residual MC1R activity)
- Less pronounced than parent compound Melanotan II due to reduced MC1R binding
Contraindications (FDA label) [2]:
- Uncontrolled hypertension or cardiovascular disease
- Concurrent naltrexone use (pharmacodynamic interaction)
- Pregnancy (Category X; abortifacient potential demonstrated preclinically)
- Known hypersensitivity to bremelanotide
Monitoring parameters [4]:
- Blood pressure and heart rate before and 1-2 hours after first administration
- Monitor for severe or prolonged nausea
- Monitor for priapism (erection lasting >4 hours), particularly in male off-label users
- Assess sexual function outcomes via validated questionnaires if used therapeutically
Side effect profiles are most useful when you can compare them against your own experience in real time. Doserly lets you log symptoms, severity, and timing alongside your dosing data, creating a side-by-side view of your protocol and your body's response.
This kind of systematic tracking catches things that memory alone misses. A subtle mood shift that began three days after a dose increase. Sleep disruption that correlates with evening administration. These patterns become visible when the data is laid out on a timeline, and they give your healthcare provider actionable information rather than vague concerns. Early detection of emerging side effects means earlier intervention.
Keep side effects, flags, and follow-up notes visible.
Doserly helps you document safety observations, side effects, medication changes, and follow-up questions so important context is not scattered.
Safety log
Flags and notes

Safety notes are not emergency guidance; seek medical help when appropriate.
Dosing Protocols
The Basics
PT-141 dosing is different from most peptides because it uses an on-demand model rather than daily dosing. You take it when you anticipate needing it, not on a regular schedule. The FDA-approved dose for women with HSDD is 1.75 mg (1750 mcg) administered subcutaneously at least 45 minutes before anticipated sexual activity [2].
However, community experience suggests that many individuals, particularly those new to the compound, benefit from starting at a lower dose and working up. Starting at 500 mcg allows you to assess your individual tolerance, particularly for nausea, before committing to a full dose. Some users find that 500-1000 mcg is sufficient for their needs, while others require the full 1.75 mg [2].
For men using PT-141 off-label, dosing is less standardized. Community reports and early clinical data suggest a range of 0.3-2.5 mg, with most discussion centering on 1-2 mg per dose. Men appear to experience more dose-dependent side effects, and several sources recommend starting at 0.5 mg or lower to assess tolerance [4].
There are firm limits: no more than one dose in any 24-hour period, and no more than 8 doses per month. These limits are based on safety data from the clinical trials [2].
The Science
FDA-approved regimen (women with HSDD) [2]:
Parameter
Dose
- Value
- 1.75 mg (1750 mcg)
Parameter
Route
- Value
- Subcutaneous (abdomen or thigh)
Parameter
Timing
- Value
- At least 45 minutes before anticipated sexual activity
Parameter
Frequency
- Value
- On-demand; max 1 dose per 24 hours
Parameter
Monthly limit
- Value
- Max 8 doses per month
Commonly reported community protocols:
Use Case
Women (HSDD, following FDA label)
- Starting Dose
- 1.75 mg
- Target Dose
- 1.75 mg
- Frequency
- On-demand, max 8/month
Use Case
Women (conservative start)
- Starting Dose
- 500 mcg
- Target Dose
- 1.0-1.75 mg
- Frequency
- On-demand
Use Case
Men (on-demand)
- Starting Dose
- 500 mcg
- Target Dose
- 1.0-2.0 mg
- Frequency
- On-demand, max 8/month
Use Case
Men (conservative start)
- Starting Dose
- 100-300 mcg
- Target Dose
- 0.5-1.25 mg
- Frequency
- On-demand
Reconstitution:
- 10 mg vial + 3.0 mL bacteriostatic water = ~3.33 mg/mL concentration
- At this concentration, 1 unit on a U-100 insulin syringe = approximately 33.3 mcg
- Alternative: 10 mg vial + 2.0 mL bacteriostatic water = 5 mg/mL (each unit = 50 mcg)
Timing considerations: Community reports consistently suggest that dosing well in advance (4-8 hours) or the evening before anticipated activity produces more reliable results and allows initial side effects (nausea, flushing) to resolve before the desired effects peak.
The dosing protocols above involve numbers that matter: specific microgram amounts, reconstitution ratios, and timing windows. Getting any of these wrong compounds across every subsequent dose from that vial.
Doserly's dose and reconstitution calculators eliminate the guesswork. Enter your vial size, peptide amount, and target dose, and get the exact bacteriostatic water volume, units per tick mark, and doses per vial. The injection site tracker maps your administration history as a visual heat map across your body, flagging areas that need rest and suggesting rotation patterns. Combined with dose reminders that include compound name, amount, and route, every aspect of your daily protocol is handled with the precision it requires.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders

Reminder tracking supports consistency; it does not select a protocol for you.
What to Expect
First Use (Day 1): The first experience is the most unpredictable. Most users report nausea and facial flushing within 30-90 minutes of injection. The severity varies widely. Some describe it as mild queasiness, while others compare it to a bad hangover or flu. Pre-medicating with ondansetron (Zofran) is the most commonly recommended mitigation strategy in the community. Sexual effects may emerge anywhere from 1 to 8 hours after injection, with significant individual variability. Many experienced users recommend a trial run at home before using PT-141 for an important occasion.
First Few Uses (Doses 2-4): Nausea typically diminishes with repeated exposure. By the third or fourth dose, many users report that side effects are manageable or absent. This is the dose-finding period where users adjust their dose up or down to find their personal "sweet spot." Onset timing tends to become more predictable as you learn your body's response pattern.
Established Use (Regular On-Demand): Once an effective dose is found, most users describe consistent enhancement of desire and physical arousal lasting 6-24 hours. Some report effects persisting subtly for up to 48 hours. The on-demand model means there is no cumulative build-up or loading phase. Each dose is an independent event.
Long-Term (6+ Months): The 52-week clinical extension study showed sustained or increasing efficacy with no evidence of tolerance [7]. Community users who have used PT-141 regularly for months report continued effectiveness. Some note that with repeated use, the onset becomes faster and more predictable. Occasional mild skin darkening of freckles or moles may become noticeable with long-term repeated use.
Interaction Compatibility
Commonly Combined With
- Melanotan II — Parent compound. Some users combine MT-II (for tanning) with on-demand PT-141 (for sexual function). Both act on melanocortin receptors; concurrent use increases risk of receptor overstimulation, nausea, and cardiovascular effects. Use extreme caution.
- Oxytocin — Community protocols mention combining oxytocin (intranasal) with PT-141 for enhanced emotional bonding and intimacy effects. Both compounds influence oxytocin pathways.
- Kisspeptin — GnRH-stimulating peptide. Some practitioners discuss combining kisspeptin (for hormonal support) with PT-141 (for desire enhancement) in comprehensive sexual health protocols.
Cautions and Contraindications
- Naltrexone — Concurrent use is contraindicated per the FDA label. Naltrexone may block opioid-mediated pathways that interact with melanocortin signaling [2].
- PDE5 inhibitors (sildenafil, tadalafil) — Community reports suggest combining PT-141 with PDE5 inhibitors is generally tolerated and may be synergistic (central desire + peripheral blood flow). However, the combination may increase priapism risk and blood pressure effects. Medical supervision is strongly recommended.
- Antihypertensive medications — PT-141 may transiently increase blood pressure. Individuals on blood pressure medications should exercise caution and monitor closely.
- SSRI/SNRI antidepressants — No formal interaction data. Theoretically, PT-141's pro-dopaminergic mechanism may partially counteract SSRI-induced sexual dysfunction, which is a common clinical context for PT-141 use.
- Other melanocortin agonists — Concurrent use of PT-141 with Melanotan II or other MCR agonists requires careful monitoring due to overlapping receptor targets.
- Alpha-adrenergic blockers — May compound blood pressure effects.
Administration Guide
Materials required:
- PT-141 lyophilized powder (typically 10 mg vial)
- Bacteriostatic water (for reconstitution)
- U-100 insulin syringes (29-31G, 1/2 inch)
- Alcohol swabs
- Sharps disposal container
Recommended reconstitution solution: Bacteriostatic water (0.9% benzyl alcohol) is the standard reconstitution solution for PT-141. Use sterile water if bacteriostatic water is not available, but use the solution within 24 hours if sterile water is used.
Timing considerations: The FDA-approved protocol recommends administration at least 45 minutes before anticipated sexual activity. However, community experience widely reports that the peak effect often occurs 4-8 hours after injection. Many users dose in the morning for evening plans, or the night before, sleeping through the nausea period. Finding personal timing requires experimentation.
Post-administration care:
- Nausea is the most common immediate reaction. Pre-medicating with ondansetron (Zofran) 30-60 minutes before PT-141 is widely recommended in community discussion.
- Facial flushing is common within the first 30-90 minutes and is not cause for concern unless accompanied by severe headache or chest pain.
- Monitor blood pressure, particularly during the first few uses.
- If an erection persists beyond 4 hours (priapism), seek emergency medical attention.
Supplies & Planning
General supplies for PT-141 use:
Supply
PT-141 vials (10 mg)
- Notes
- Number depends on dose and frequency of use. At 1.75 mg/dose, one 10 mg vial provides approximately 5-6 doses.
Supply
Bacteriostatic water (30 mL)
- Notes
- One bottle typically sufficient for multiple vials.
Supply
U-100 insulin syringes
- Notes
- One per injection. 29-31G, 1/2 inch recommended. Consider 30-unit syringes for doses under 15 units for measurement accuracy.
Supply
Alcohol swabs
- Notes
- For cleaning vial stoppers and injection sites.
Supply
Sharps container
- Notes
- Required for safe needle disposal.
Supply
Anti-nausea medication
- Notes
- Ondansetron (Zofran) widely recommended in community. Consult healthcare provider.
Specific quantities depend on individual dosing, frequency of use, and healthcare provider guidance. Use the reconstitution calculator for preparation math specific to your vial size and target dose.
Storage & Handling
Lyophilized (powder) form:
- Optimal: Store at -20C or below. Can remain stable at -80C for long-term storage (2-3 years).
- Acceptable: Refrigerate at 2-8C for weeks to months.
- Room temperature: Stable short-term (days), but not recommended for extended storage.
- Keep in original sealed packaging. Protect from light and moisture.
Reconstituted (liquid) form:
- Refrigerate at 2-8C immediately after reconstitution.
- Use within 1-4 weeks when reconstituted with bacteriostatic water.
- Do not freeze reconstituted solution.
- Inspect for cloudiness, particles, or discoloration before each use. Discard if any abnormalities are observed.
- Special note: PT-141 reconstituted solutions have a shorter recommended refrigeration life (1 week per some sources) compared to many other peptides.
Handling best practices:
- Allow lyophilized vials to reach room temperature (10-30 minutes) before opening to prevent condensation.
- Wrap vials in foil or store in opaque containers to protect from light.
- Swab vial stopper with alcohol before each draw.
- Use sterile needles and syringes for each injection.
- Label vials with reconstitution date.
Lifestyle Factors
Sexual function and desire are influenced by a constellation of lifestyle factors that can significantly affect PT-141's efficacy. Addressing these factors creates a foundation that supports the compound's mechanism of action.
Stress management: Chronic stress suppresses hypothalamic function, the same brain region PT-141 targets. Stress management practices (meditation, therapy, relaxation techniques) may enhance PT-141's effects by reducing baseline suppression of the melanocortin signaling pathway.
Sleep: Adequate sleep (7-9 hours) is critical for hormonal balance, dopamine receptor sensitivity, and neural recovery. Sleep deprivation impairs the neuroendocrine pathways that PT-141 activates.
Exercise: Regular physical activity supports cardiovascular health, blood flow, hormonal balance, and mood, all of which contribute to sexual function. Moderate aerobic exercise has been independently shown to improve sexual function.
Diet and nutrition: A nutrient-dense diet supporting cardiovascular health and systemic blood flow supports PT-141's efficacy. Adequate zinc, vitamin D, and omega-3 fatty acids are associated with healthy sexual function.
Alcohol: Alcohol impairs vascular response, neural signaling, and judgment. Several community reports note reduced PT-141 efficacy with concurrent alcohol use, and some report lower alcohol tolerance while using the peptide.
Relationship factors: PT-141 enhances desire through neurochemical pathways, but it operates within the context of relationship dynamics, emotional state, and psychological readiness. Open communication with partners about expectations and timing can significantly improve the experience.
Regulatory Status & Research Classification
United States (FDA): Bremelanotide is FDA-approved (2019) under the brand name Vyleesi for the treatment of acquired, generalized hypoactive sexual desire disorder (HSDD) in premenopausal women. It is administered via a prefilled auto-injector. Bremelanotide is not approved for male erectile dysfunction or any other indication. Off-label use is not illegal but is not covered by the FDA's safety determination. The approval was based on the RECONNECT Phase 3 trials [2]. Bremelanotide is available as a compounding ingredient under certain conditions.
Canada (Health Canada): Not approved as of the current date.
United Kingdom (MHRA): Not approved as of the current date. Available through private prescribing pathways in some contexts.
Australia (TGA): Not approved as of the current date.
European Union (EMA): Not approved. Palatin Technologies (the developer) has not pursued EMA marketing authorization.
WADA Status: Not currently listed on the WADA Prohibited List.
Active clinical trials: Palatin Technologies has resumed clinical investigation for male erectile dysfunction using the subcutaneous formulation. ClinicalTrials.gov contains registered studies for bremelanotide in sexual dysfunction contexts.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is the difference between PT-141 and Viagra?
Viagra (sildenafil) and similar PDE5 inhibitors work by increasing blood flow to the genitals. PT-141 works in the brain by activating melanocortin receptors that control sexual desire. Viagra addresses the physical ability to achieve an erection; PT-141 addresses the wanting. Based on available research, PT-141 appears to be effective for individuals whose sexual difficulties are rooted in low desire or psychological factors, even when blood-flow medications have not helped [3][5].
How long does PT-141 take to work?
The FDA label recommends administration at least 45 minutes before anticipated activity. However, community reports show highly variable onset times, ranging from 1 to 8 hours. Many experienced users report peak effects at 4-8 hours post-injection or even the following day. Finding personal timing typically requires a few trial runs.
How long do the effects last?
Clinical studies report a pharmacodynamic effect window of 2-6 hours. Community reports frequently describe effects lasting 12-24 hours, with some reporting subtler effects persisting for up to 48 hours. The half-life of the peptide itself is approximately 2.7 hours, but the downstream neurochemical effects outlast the peptide's presence in the bloodstream [2][6].
Can PT-141 be used by men?
PT-141 is not FDA-approved for men, but clinical studies have demonstrated efficacy for male erectile dysfunction, particularly in PDE5 inhibitor non-responders with psychogenic ED [3][5]. Male off-label use is widely discussed in community forums. Men may experience more pronounced side effects (especially nausea) than women at comparable doses [4].
How do I manage the nausea?
The most widely recommended approach in the community is pre-medicating with ondansetron (Zofran) 30-60 minutes before PT-141. Other commonly reported strategies include: dosing before sleep to sleep through the nausea, starting at a lower dose and titrating up, having ginger tea or ginger candies on hand, and eating a light snack before dosing. Nausea tends to diminish with repeated use [2].
Can PT-141 cause permanent side effects?
Based on clinical trial data through 52 weeks, no permanent adverse effects have been reported [7]. However, community reports of sexual anhedonia (inability to feel pleasure) in some male users are a concern. While most reports describe this as temporary (resolving within days to weeks after discontinuation), some individuals report effects persisting longer. This adverse effect is not well-characterized in formal clinical data. Individuals who notice any change in their ability to experience pleasure should discontinue use and consult a healthcare provider.
Can I combine PT-141 with other ED medications?
Community reports suggest that PT-141 can be used alongside PDE5 inhibitors (Viagra, Cialis) because they work through different mechanisms. Some users describe this combination as synergistic, with PT-141 providing desire and PDE5 inhibitors providing physical support. However, combining these medications may increase the risk of priapism and blood pressure effects. Always discuss combination use with a healthcare provider.
Is the nasal spray form effective?
The intranasal formulation was explored during clinical development but was abandoned due to inconsistent absorption and more pronounced blood pressure effects compared to subcutaneous injection. Nasal sprays sold through unofficial channels have unquantified bioavailability. The subcutaneous route provides approximately 100% bioavailability and is the only route with clinical validation [3].
Sources & References
Clinical Trials & Human Studies:
[1] Dorr RT, Lines R, Levine N, et al. "Evaluation of melanotan-II, a superpotent cyclic melanotropic peptide in a pilot phase-I clinical study." Life Sciences. 1996;58(20):1777-1784. PMID: 8637402
[2] Kingsberg SA, Clayton AH, Portman D, et al. "Bremelanotide for the treatment of hypoactive sexual desire disorder: Two randomized phase 3 trials." Obstetrics & Gynecology. 2019;134(5):899-908. PMID: 31599840. DOI: 10.1097/AOG.0000000000003500
[3] Diamond LE, Earle DC, Rosen RC, et al. "Double-blind, placebo-controlled evaluation of the safety, pharmacokinetic properties and pharmacodynamic effects of intranasal PT-141, a melanocortin receptor agonist, in healthy males and patients with mild-to-moderate erectile dysfunction." International Journal of Impotence Research. 2004;16(1):51-59. DOI: 10.1038/sj.ijir.3901115
[4] FDA. "Vyleesi (bremelanotide) prescribing information." 2019. Available at: https://accessdata.fda.gov/drugsatfda_docs/label/2019/210557s000lbl.pdf
[5] Wessells H, Fuciarelli K, Hansen J, et al. "Synthetic melanotropic peptide initiates erections in men with psychogenic erectile dysfunction: double-blind, placebo controlled crossover study." Journal of Urology. 1998;160(2):389-393. PMID: 9679880
[6] Pfaus JG, et al. "The neurobiology of bremelanotide for the treatment of female hypoactive sexual desire disorder." CNS Spectrums. 2021;26(2):107-115. PMID: 33455598
[7] Clayton AH, et al. "Long-term safety and efficacy of bremelanotide for hypoactive sexual desire disorder." Obstetrics & Gynecology. 2019;134(5):909-917. PMID: 31599847
Reviews & Meta-Analyses:
[8] Spielmans GI, Ellefson EM. "Small effects, questionable outcomes: Bremelanotide for hypoactive sexual desire disorder." Journal of Sex & Marital Therapy. 2024.
[9] Nappi RE, Tiranini L, Martini E, et al. "Medical treatment of female sexual dysfunction." Nature Reviews Urology. 2022;19:708-721.
[10] Hedlund P. "PT-141 Palatin." Current Opinion in Investigational Drugs. 2004;5(4):414-421.
Related Peptide Guides
- Melanotan II — Parent compound from which PT-141 was derived. Non-selective melanocortin agonist used primarily for tanning.
- Melanotan I — Linear melanocortin analog (afamelanotide). MC1R-selective, FDA/EMA-approved for erythropoietic protoporphyria.
- Oxytocin — "Bonding hormone" with complementary effects on emotional intimacy and social connection.
- Kisspeptin — GnRH-stimulating peptide involved in reproductive hormone regulation.
- Gonadorelin — Synthetic GnRH analog for gonadotropin stimulation.
- HCG — Human chorionic gonadotropin, used in fertility and testosterone maintenance protocols.
Need the reconstitution math for PT-141: Complete Research Guide?
Open the calculator with PT-141: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.