Melanotan I: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Afamelanotide, [Nle4, D-Phe7]-alpha-MSH, NDP-MSH, NDP-alpha-MSH, Scenesse (brand name)
Attribute
Administration
- Detail
- Injectable (subcutaneous), Implant (subcutaneous bioresorbable, physician-administered)
Attribute
Research Status
- Detail
- FDA-approved as Scenesse for erythropoietic protoporphyria (EPP). Phase III trials in vitiligo. EMA-approved for EPP. Research peptide versions are not equivalent to the approved pharmaceutical implant.
Attribute
Typical Dose Range
- Detail
- Implant: 16 mg every 60 days (physician-administered). Injectable (research): 250-1,000 mcg/day subcutaneously.
Attribute
Half-Life
- Detail
- Approximately 30 minutes (free peptide); ~15 hours apparent half-life with implant formulation (flip-flop kinetics)
Attribute
Cycle Length
- Detail
- Implant: up to 6 implants per year (continuous). Injectable: 2-3 month courses, often season-limited
Attribute
Storage
- Detail
- Lyophilized: -20C to 2-8C, protected from light; Reconstituted: 2-8C, use within 30 days
Overview / What Is Melanotan I?
The Basics
Melanotan I is a synthetic version of alpha-MSH (alpha-melanocyte-stimulating hormone), the natural hormone your body produces to trigger tanning when your skin is exposed to sunlight. It was developed in the 1980s at the University of Arizona as a way to produce protective skin darkening without requiring heavy UV exposure.
What makes Melanotan I notable is that it actually became an FDA-approved drug. Under the brand name Scenesse, it is used to treat erythropoietic protoporphyria (EPP), a rare genetic condition where even brief sunlight exposure causes severe, debilitating pain. For these patients, Melanotan I functions like an internal sunscreen, increasing the protective melanin pigment so they can spend more time outdoors without experiencing phototoxic reactions.
Melanotan I is often compared to its cousin, Melanotan II, but the two are quite different. Think of Melanotan I as a single-purpose key that opens one specific lock: the MC1R receptor on your skin cells, which controls pigmentation. Melanotan II is more like a master key that opens multiple locks throughout the body, including receptors in the brain that affect appetite and sexual arousal. This selectivity is why Melanotan I earned regulatory approval while Melanotan II did not. Melanotan I produces tanning with significantly fewer off-target effects.
Beyond tanning, emerging research suggests Melanotan I may have neuroprotective properties, cardiovascular benefits, and anti-inflammatory effects, though these applications remain under investigation.
The Science
Melanotan I (afamelanotide, [Nle4, D-Phe7]-alpha-MSH) is a linear tridecapeptide analog of alpha-melanocyte-stimulating hormone (alpha-MSH) with two amino acid substitutions that dramatically enhance its pharmacological profile [1]. The norleucine substitution at position 4 prevents methionine oxidation, while the D-phenylalanine substitution at position 7 confers resistance to enzymatic degradation and increases receptor binding affinity approximately 1,000-fold relative to native alpha-MSH [2][3].
The peptide was synthesized in 1980 by Sawyer, Hruby, and Hadley at the University of Arizona [1]. Its primary target is the melanocortin-1 receptor (MC1R) on epidermal melanocytes, where it acts as a full agonist with sub-nanomolar binding affinity (~0.1 nM). MT-I retains approximately 10-fold selectivity for MC1R over other melanocortin receptor subtypes (MC3R, MC4R, MC5R), a modest but functionally significant margin that concentrates its activity on cutaneous melanogenesis and photoprotection [2][3].
The linear 13-residue structure (Ac-Ser-Tyr-Ser-Nle-Glu-His-D-Phe-Arg-Trp-Gly-Lys-Pro-Val-NH2) does not meaningfully cross the blood-brain barrier, which accounts for the absence of central nervous system effects (appetite suppression, sexual arousal) observed with the structurally distinct cyclic heptapeptide Melanotan II [4][5]. Neither MT-I nor MT-II activates MC2R, the ACTH-specific adrenal receptor, meaning neither compound triggers cortisol synthesis [3].
Afamelanotide received FDA approval in October 2019 under the brand name Scenesse for increasing pain-free light exposure in adults with erythropoietic protoporphyria [6]. The EMA authorized the drug in 2014 under exceptional circumstances [7].
Molecular Identity
Attribute
Common Names
- Detail
- Melanotan I, MT-I, Afamelanotide, [Nle4, D-Phe7]-alpha-MSH, NDP-MSH, NDP-alpha-MSH
Attribute
Brand Name
- Detail
- Scenesse (CLINUVEL Pharmaceuticals)
Attribute
Amino Acid Sequence
- Detail
- Ac-Ser-Tyr-Ser-Nle-Glu-His-D-Phe-Arg-Trp-Gly-Lys-Pro-Val-NH2
Attribute
Sequence Length
- Detail
- 13 amino acids (tridecapeptide)
Attribute
Molecular Formula
- Detail
- C78H111N21O19
Attribute
Molecular Weight
- Detail
- 1,646.85 Da
Attribute
CAS Number
- Detail
- 75921-69-6
Attribute
PubChem CID
- Detail
- 16133793
Attribute
Target Receptor
- Detail
- MC1R (Melanocortin-1 Receptor), primary; MC3R, MC4R, MC5R secondary at higher concentrations
Attribute
Functional Class
- Detail
- Melanocortin receptor agonist; alpha-MSH analog; photoprotective agent
Attribute
Origin
- Detail
- Synthetic (developed at University of Arizona, 1980)
Attribute
Solubility
- Detail
- Water-soluble
Mechanism of Action
The Basics
When your skin is exposed to UV light, your body naturally produces alpha-MSH, which tells special cells called melanocytes to produce melanin, the pigment that darkens your skin and absorbs harmful UV radiation. Melanotan I mimics this natural hormone, but with two key advantages: it is much more powerful (roughly 1,000 times more potent) and lasts much longer because it resists the enzymes that would normally break it down.
Here is how it works, step by step. Melanotan I attaches to the MC1R receptor on melanocytes (the pigment-producing cells in your skin). This activates an internal signaling cascade that ultimately switches on the genes responsible for producing eumelanin, which is the brown-black form of melanin that provides real UV protection. Unlike pheomelanin (the red-yellow pigment more common in fair-skinned people), eumelanin actually absorbs UV radiation and neutralizes damaging molecules called free radicals.
Melanotan I also appears to enhance your skin's DNA repair machinery, providing a second layer of protection beyond pigment production. This means it does not just make you darker; it helps your cells fix UV damage more efficiently.
The critical difference from Melanotan II is selectivity. Melanotan I focuses its action on that one receptor on your skin cells. It does not significantly activate the brain receptors (MC3R, MC4R) that cause the appetite suppression and sexual arousal effects associated with Melanotan II.
The Science
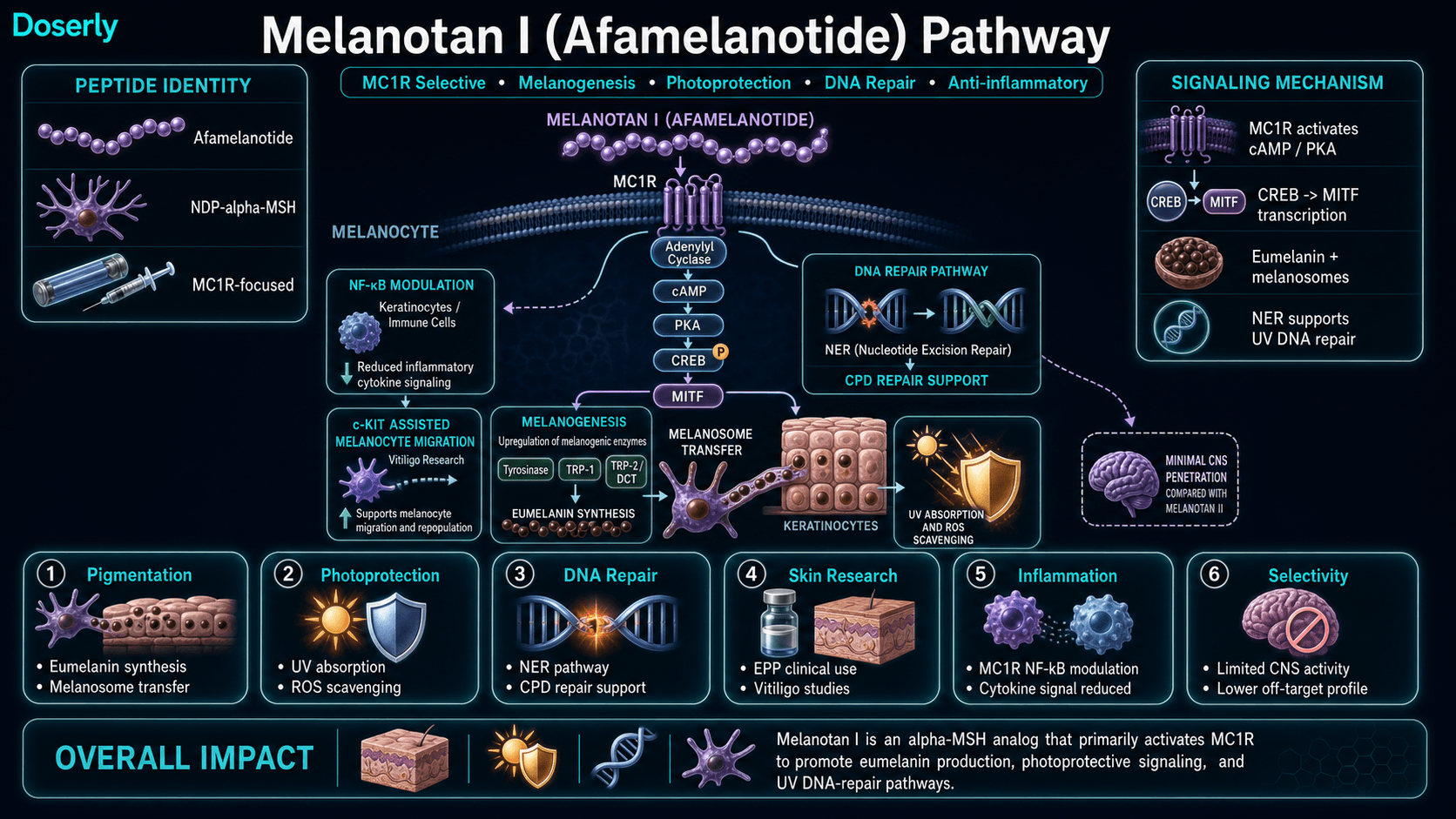
MC1R activation by afamelanotide stimulates adenylyl cyclase, elevating intracellular cyclic AMP (cAMP), which activates protein kinase A (PKA). PKA phosphorylates CREB (cAMP response element-binding protein), which upregulates MITF (microphthalmia-associated transcription factor), the master regulator of melanocyte differentiation and melanogenesis [2][8].
MITF induces expression of three key enzymes in the eumelanin biosynthetic pathway: tyrosinase, tyrosinase-related protein 1 (TRP-1), and tyrosinase-related protein 2 (TRP-2/DCT). These enzymes catalyze the sequential conversion of tyrosine to DOPA, dopaquinone, and ultimately eumelanin [8]. The resulting eumelanin provides photoprotection through two mechanisms: direct absorption of UV radiation and scavenging of reactive oxygen species (ROS) [2][3].
Beyond melanogenesis, MC1R activation enhances nucleotide excision repair (NER) of UV-induced cyclobutane pyrimidine dimers (CPDs), providing DNA repair capacity independent of pigment production [3][9]. This dual mechanism (pigmentation plus DNA repair) explains why MC1R loss-of-function variants (R151C, R160W, D294H), which are prevalent in fair-skinned populations, are established melanoma risk factors [9].
Additional demonstrated pathways include:
- Melanocyte proliferation and dendritic extension via c-Kit receptor pathway potentiation, promoting melanocyte migration into depigmented areas relevant to vitiligo therapy [8]
- Anti-inflammatory activity through MC1R-mediated suppression of NF-kB signaling in keratinocytes and immune cells, reducing pro-inflammatory cytokines (TNF-alpha, IL-1beta, IL-6) [8][10]
- At higher concentrations, cross-reactivity at MC3R, MC4R, and MC5R contributes to modest peripheral effects including potential blood pressure modulation (MC4R) and fatty acid oxidation (MC5R) [8][11]
Pathway Visualization
Pharmacokinetics
The Basics
Melanotan I has a short life in the bloodstream. As a free peptide, it is broken down within about 30 minutes. This rapid clearance is why the approved pharmaceutical version (Scenesse) uses a slow-release implant that delivers the peptide gradually over 60 days, creating an apparent half-life of around 15 hours.
For injectable research peptide versions, the short half-life means the peptide clears the body quickly after each dose. However, the tanning effect it triggers persists much longer than the peptide itself, because melanin, once produced, remains in the skin for weeks as part of the normal skin cell turnover cycle. Volunteers who received Melanotan I in early clinical studies retained their tan for weeks after the drug became undetectable in their blood. Some researchers followed up with subjects 25 years after their first exposure and found no late-onset effects [4].
The key pharmacokinetic parameters for the implant formulation include: peak plasma concentration at approximately 36 hours after implant insertion, with over 90% of the drug released by day 5 and plasma levels undetectable by day 10. Subcutaneous bioavailability is 100% for the implant formulation [4].
Melanotan I has no oral bioavailability (it would be destroyed by digestive enzymes) and does not meaningfully cross the blood-brain barrier, which is why it lacks the central nervous system effects of Melanotan II [4][5].
The Science
Afamelanotide pharmacokinetics have been characterized primarily in the context of the 16 mg bioresorbable subcutaneous implant formulation [4].
Parameter
Tmax
- MT-I (16 mg implant)
- ~36 hours
Parameter
Intrinsic t1/2
- MT-I (16 mg implant)
- ~30 minutes
Parameter
Apparent t1/2
- MT-I (16 mg implant)
- ~15 hours (implant-driven, flip-flop kinetics)
Parameter
Cmax
- MT-I (16 mg implant)
- 3.7 ng/mL
Parameter
BBB penetration
- MT-I (16 mg implant)
- Minimal
Parameter
SC bioavailability
- MT-I (16 mg implant)
- 100% (implant formulation)
Parameter
Oral bioavailability
- MT-I (16 mg implant)
- 0%
Parameter
Duration of melanogenic effect
- MT-I (16 mg implant)
- Weeks beyond drug clearance
The implant provides controlled release: median Tmax at approximately 36 hours post-insertion, with greater than 90% of drug liberated by day 5 and plasma concentrations falling below the limit of quantitation by day 10 [4][7]. The intrinsic elimination half-life of the free peptide is approximately 30 minutes, but the absorption rate-limited release from the implant creates flip-flop kinetics with an apparent half-life of roughly 15 hours [4].
For subcutaneous injection of research peptide formulations, absorption is expected to be rapid (analogous to Melanotan II data showing absorption half-life of 0.07-0.79 hours), with similarly brief elimination kinetics [5]. The persistent melanogenic effect despite rapid drug clearance reflects the time course of melanin turnover in the epidermis rather than ongoing receptor stimulation [4].
Research & Clinical Evidence
Erythropoietic Protoporphyria (EPP)
The Basics
Erythropoietic protoporphyria is a rare genetic condition where even brief sunlight exposure causes intense, burning pain in the skin. People with EPP often have to avoid sunlight almost entirely, which dramatically limits their quality of life. Melanotan I (as Scenesse) was specifically developed and approved for these patients.
The results in clinical trials were meaningful. Patients who received the implant could spend significantly more time in direct sunlight without pain. In one European trial, treated patients averaged 6 hours of pain-free sun exposure over the study period compared to just 45 minutes for those receiving placebo. Phototoxic reactions were roughly cut in half. Long-term follow-up of 115 patients over up to 8 years showed that quality-of-life scores nearly doubled and remained elevated throughout the entire observation period.
The Science
Afamelanotide's EPP clinical programme comprises three Phase III randomised controlled trials enrolling 244 patients across US and European sites [6].
The pivotal US trial (CUV039, n=93) demonstrated that patients receiving three afamelanotide implants every 60 days spent a median of 64.1 hours in pain-free direct sunlight over 180 days, compared to 40.5 hours for placebo (P=0.04) [6]. The European trial (CUV029, n=74) showed median pain-free sunlight of 6.0 hours versus 0.75 hours for placebo over 270 days (P<0.05), with phototoxic reactions reduced from 146 to 77 events (P=0.04) [6]. A third trial (CUV017, n=91) demonstrated significant reductions in pain frequency (P=0.0023) and average pain severity (P=0.0017) over 12 months [6][12].
Biolcati et al. followed 115 EPP patients for up to 8 years on afamelanotide, documenting quality-of-life scores rising from 31% to 74% of maximum, a gain sustained throughout the entire observation period [7]. Adverse events were predominantly mild: nausea, headache, and localised hyperpigmentation at the implant site.
Photoprotection and Tanning
The Basics
Melanotan I was originally developed as a sunless tanning agent, and clinical trials confirm it works remarkably well for this purpose. Subjects who received the peptide were 75% more likely to develop a tan and 47% less likely to experience sunburn. They needed roughly 50% less UV exposure to achieve equivalent tanning compared to controls, and their tan lasted about three weeks longer.
What is particularly noteworthy is that Melanotan I works even in people who normally cannot tan at all. Individuals with variant MC1R genes (common in redheads and very fair-skinned people, Fitzpatrick skin types I and II) showed significant increases in melanin density and visible tanning. One study demonstrated approximately 50% fewer sunburn cells and 60% less DNA damage compared to placebo.
The Science
Phase I trials of subcutaneous afamelanotide in healthy volunteers demonstrated dose-dependent increases in skin melanin density, with measurable tanning occurring even in individuals carrying MC1R loss-of-function variants (the R151C and R160W alleles associated with red hair and poor tanning capacity) [13][14].
Barnetson et al. (2006) showed that MT-I increased melanin density without UV exposure, enhanced photoprotection, reduced sunburn cell formation, and produced no serious adverse events in a controlled study [15]. The combination of pharmacological melanogenesis with UV exposure produced synergistic photoprotection superior to either intervention alone.
Vitiligo
The Basics
Vitiligo causes patches of skin to lose their pigment, creating visible white areas. Researchers have studied whether Melanotan I could help repigment these areas, particularly when combined with narrowband UVB light therapy (a standard vitiligo treatment). In a Phase II trial, the combination achieved about 49% repigmentation compared to 33% with light therapy alone, with significantly faster results on the face and upper extremities. A large Phase III trial (CUV105) enrolling over 200 patients was underway as of 2025.
The Science
A Phase II randomised controlled trial (n=55, Fitzpatrick skin types III-VI) demonstrated that afamelanotide combined with narrowband UV-B (NB-UVB) phototherapy achieved 48.6% repigmentation at day 168 versus 33.3% with NB-UVB alone, with significantly faster onset on the face and upper extremities [16]. The repigmentation mechanism involves MC1R-mediated melanocyte proliferation and migration into depigmented epidermis, augmenting the phototherapy-induced melanocyte activation [8].
Phase III trial CUV105, enrolling over 200 patients as of May 2025, evaluates afamelanotide for vitiligo as both monotherapy and adjunctive therapy [17].
Neuroprotection and Cognitive Function
The Basics
Preclinical research in mouse models suggests that Melanotan I may protect the brain against the type of damage that leads to cognitive decline and Alzheimer's disease. Even very small doses appeared to reduce amyloid beta plaques (the protein clumps associated with Alzheimer's), protect neurons from death, and improve measures of cognitive function. These effects appear to be mediated through the MC4 receptor and involve increasing brain-derived neurotrophic factor (BDNF), a protein critical for maintaining healthy brain connections.
Separate studies in stroke models showed that treatment with Melanotan I could reduce brain damage and improve recovery of learning and memory, even when administered up to 9 hours after the stroke event. A small feasibility study (n=6) in human stroke patients showed early improvement in neurological scores.
These findings are promising but remain in early stages. No large-scale human trials for neurological applications have been completed.
The Science
In triple-transgenic mouse models of Alzheimer's disease, daily administration of NDP-alpha-MSH reduced levels of amyloid beta plaques, protected neurons from apoptosis, and improved clinical measures of cognitive function and synaptic transmission. These effects were abolished by MC4R antagonism, confirming the receptor dependence of the neuroprotective mechanism [18][19].
MC4R stimulation boosted neurogenesis and cognitive recovery in AD models, with once-daily MT-I administration reducing levels of all AD-related biomarkers across multiple pathophysiological pathways [19][20]. MC4R activation on astrocytes increased BDNF expression via the ERK-cFos pathway, enhancing synaptic stability and neurogenesis [21].
In gerbil models of ischemic stroke, nanomolar doses of NDP-alpha-MSH reduced neuronal death, improved recovery of learning and memory, and promoted synaptic plasticity even when administered 9 hours post-event. The mechanism involves overexpression of the Zif268 gene [22]. A Phase IIa feasibility study (n=6) in acute human stroke patients showed median NIHSS improvement from 6 to 2 by day 7 [23].
Cardiovascular Effects
The Basics
Animal studies have found that Melanotan I can reduce high blood pressure without affecting normal blood pressure, a potentially valuable property since many current blood pressure medications can cause dangerously low readings. In heart attack models, administration of melanocortins including Melanotan I during cardiac arrest improved survival rates by 81%, restored blood pressure and heart rate, and reduced inflammatory markers.
The Science
Research in DOCA-salt hypertensive mice demonstrated that alpha-MSH analogs attenuate blood pressure elevation without affecting normotensive animals, suggesting selective antihypertensive activity [24]. In rat cardiac arrest models, NDP-alpha-MSH administration during CPR in conjunction with epinephrine restored baseline arterial pressure and heart rate, reversed metabolic acidosis, reduced inflammatory markers, and improved survival rate by 81% [25].
Neuroinflammatory Disease
The Basics
In mouse models of multiple sclerosis, Melanotan I interfered with the immune process that destroys the protective coating (myelin) on nerve cells. It prevented myelin loss and even helped restore nerve signaling. Similar protective effects were observed in models of uveitis, a painful inflammatory eye condition.
The Science
MC1R activation by NDP-alpha-MSH demonstrated neuroprotective properties in experimental autoimmune encephalomyelitis (EAE), the standard mouse model of multiple sclerosis. Administration prevented demyelination and improved myelin recovery [10]. In experimental autoimmune uveitis, alpha-MSH suppressed T-cell function through MC4R-mediated pathways; local ocular administration was as effective as systemic delivery, offering potential for reduced systemic side effects [26].
Fat Metabolism
The Basics
Research in mice suggests that Melanotan I can influence fat metabolism through the MC5 receptor, promoting the oxidation (burning) of fatty acids in muscle tissue and shifting fat cells from storage mode to burning mode. This remains an early-stage research observation.
The Science
Stimulation of MC5R by melanocortin agonists promotes oxidation of fatty acids by skeletal muscle and shifts adipocyte metabolism from lipogenesis to lipolysis [11][27]. The metabolic effects involve multiple receptor subtypes and physiological pathways, and have been characterized only in murine models.
Biomarker Evidence Matrix
Category
Skin Health
- Evidence Strength
- 9/10
- Reported Effectiveness
- 8/10
- Summary
- Three Phase III RCTs in EPP (n=244) demonstrate significant photoprotection and melanogenesis. Phase I tanning trials confirm melanin density increases even in MC1R-variant individuals. Community reports strongly positive for natural-looking tans.
Category
Inflammation
- Evidence Strength
- 6/10
- Reported Effectiveness
- 4/10
- Summary
- MC1R-mediated NF-kB suppression demonstrated in preclinical models across multiple tissue types. No human inflammation-specific trials. Community discussion minimal.
Category
Blood Pressure
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- Animal studies show selective antihypertensive effects. No human cardiovascular trials. Limited community reporting.
Category
Longevity & Neuroprotection
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- Preclinical AD models show amyloid reduction, neurogenesis, and cognitive recovery via MC4R. Small human stroke feasibility study (n=6). No completed human neurological trials. Community discussion academic only.
Category
Immune Function
- Evidence Strength
- 5/10
- Reported Effectiveness
- 4/10
- Summary
- MC1R-mediated anti-inflammatory and immunomodulatory effects in preclinical EAE and uveitis models. No human immune-specific trials.
Category
Side Effect Burden
- Evidence Strength
- 8/10
- Reported Effectiveness
- 7/10
- Summary
- Over 1,000 patients across 10+ years of clinical use with no serious adverse events reported. Community consistently reports mild, transient side effects.
Category
Nausea & GI Tolerance
- Evidence Strength
- 7/10
- Reported Effectiveness
- 6/10
- Summary
- Nausea is the most commonly reported side effect in clinical trials and community. Consistently described as mild and transient, especially relative to MT-II.
Category
Appetite & Satiety
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Minimal appetite effects expected due to MC1R selectivity and limited BBB penetration. Community reports negligible appetite changes.
Category
Libido
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- MT-I does not significantly activate MC4R in the brain. Community consistently reports absence of sexual effects, framed as an advantage over MT-II.
Category
Energy Levels
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Mild, transient fatigue occasionally reported during loading phase in clinical trials and community. Not a significant concern.
Category
Temperature Regulation
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Flushing (facial warmth/redness) is a known transient effect. Dose-dependent and self-limiting.
Category
Treatment Adherence
- Evidence Strength
- 4/10
- Reported Effectiveness
- 6/10
- Summary
- Short half-life (~30 min) necessitates daily injections for research formulations. Implant formulation (Scenesse) eliminates adherence concerns with 60-day dosing. Community reports manageable protocol.
Categories with insufficient data: Fat Loss, Muscle Growth, Weight Management, Food Noise, Sleep Quality, Focus & Mental Clarity, Memory & Cognition, Mood & Wellbeing, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Sexual Function, Joint Health, Pain Management, Recovery & Healing, Physical Performance, Gut Health, Digestive Comfort, Hair Health, Heart Health, Heart Rate & Palpitations, Hormonal Symptoms, Fluid Retention, Body Image, Bone Health, Cravings & Impulse Control, Social Connection, Withdrawal Symptoms, Daily Functioning
Benefits & Potential Effects
The Basics
The primary benefit of Melanotan I is skin darkening and UV protection. It increases production of eumelanin (the protective brown-black pigment) rather than pheomelanin (the less protective red-yellow pigment), creating a tan that genuinely shields against UV damage. This works even in people with very fair skin who normally burn rather than tan.
Beyond photoprotection, the potential benefits being explored in research include:
- Skin disorder treatment. Vitiligo repigmentation (Phase III trials ongoing), management of photosensitive conditions like polymorphous light eruption, and potential treatment of actinic keratosis (precancerous UV lesions)
- Neuroprotection. Preclinical evidence for protection against Alzheimer's disease, stroke recovery, and neuroinflammatory conditions like multiple sclerosis
- Cardiovascular support. Selective blood pressure reduction in hypertensive models without affecting normal blood pressure
- Anti-inflammatory effects. Broad anti-inflammatory activity through NF-kB suppression
- DNA repair enhancement. MC1R activation independently enhances the skin's ability to repair UV-induced DNA damage
The Science
The clinical evidence base for afamelanotide's benefits is tiered by strength:
Human RCT data (strongest): Photoprotection in EPP (three Phase III RCTs, n=244) [6][7][12]; vitiligo repigmentation adjunctive to NB-UVB (Phase II RCT, n=55) [16]; enhanced tanning and reduced UV damage in healthy volunteers (Phase I) [14][15].
Human preliminary data: Acute stroke neuroprotection (Phase IIa feasibility, n=6) [23]; actinic keratosis and squamous cell carcinoma prevention (Phase II).
Preclinical data (animal models): Neuroprotection in Alzheimer's and stroke models [18][19][20][22]; selective antihypertensive activity [24]; cardioprotection during cardiac arrest [25]; neuroinflammatory disease (EAE, uveitis) [10][26]; fatty acid oxidation and metabolic effects [11][27].
Side Effects & Safety Considerations
The Basics
Melanotan I has one of the strongest clinical safety records of any peptide in community use. Over 1,000 patients have been treated across more than 10 years of clinical observation, and no serious adverse events have been reported in the clinical programme.
The most common side effects are:
- Nausea (mild, transient, typically resolves within days)
- Headache (mild)
- Facial flushing (brief warmth and redness, dose-dependent)
- Fatigue (mild, transient during initial dosing)
- Injection site reactions (if using injectable formulation)
- Darkening of existing moles and freckles (requires monitoring)
The mole and freckle darkening warrants specific attention. While this is expected and generally manageable, any changes in the ABCDE criteria (asymmetry, border irregularity, color variation, diameter, evolution) should prompt immediate dermatologic evaluation. Regular full-body skin exams with a dermatologist are strongly recommended during and after use.
The melanoma question has been extensively investigated. The weight of evidence indicates that MC1R activation is photoprotective rather than cancer-promoting. A 40-year follow-up of 3,299 Addison's disease patients (who experience chronic MC1R activation through elevated ACTH) showed a melanoma incidence ratio numerically below expected rates. Zero melanoma events have been reported across the entire afamelanotide clinical programme [9].
Contraindications include: history of melanoma or atypical mole syndrome, current skin malignancy, pregnancy and breastfeeding, severe hepatic impairment, and hypersensitivity to alpha-MSH analogs.
The Science
The afamelanotide safety database encompasses over 1,000 patient-exposures across clinical trials and long-term follow-up studies, with over 12,000 doses administered. Treatment-emergent adverse events were predominantly mild and self-limiting: nausea, headache, nasopharyngitis, and localised hyperpigmentation at the implant insertion site [6][7].
The melanoma safety profile is supported by multiple lines of evidence. Epidemiologically, the Addison's disease cohort (3,299 patients, 40-year follow-up) showed a standardised incidence ratio for melanoma of 0.7 (95% CI: 0.2-1.6), numerically below expected rates [9]. Mechanistically, MC1R activation drives both eumelanin synthesis and enhanced nucleotide excision repair of UV-induced DNA damage, both of which are protective pathways [2][3][9]. No formal animal carcinogenicity studies have been conducted for afamelanotide, a gap acknowledged in the Scenesse FDA label [6].
The dermatologic monitoring requirement reflects the peptide's effect on melanocytic nevi rather than an established oncogenic risk. Photographic documentation pre- and post-therapy is recommended for pigment monitoring [8].
The side effects and contraindications above give you a map of what to watch for. Doserly turns that map into a daily practice. Log the specific biomarkers and symptoms associated with this compound's known risk profile, and the app builds a timeline of how your body is responding across your cycle.
Trending in the wrong direction on a key marker? Noticing a pattern that started two weeks into your protocol? Doserly connects the dots between your protocol timeline and your logged data, making it easier to spot emerging issues early and have informed, data-backed conversations with your healthcare provider about what's working and what needs attention.
Connect protocol changes to labs and health markers.
Doserly can keep lab results, biomarkers, symptoms, and dose history close together so follow-up conversations have better context.
Insights
Labs and trends

Doserly organizes data; it does not diagnose or interpret labs for you.
Dosing Protocols
The Basics
Dosing for Melanotan I varies significantly depending on the formulation. The approved pharmaceutical version (Scenesse) delivers a 16 mg dose via a subcutaneous implant every 60 days, implanted by a specialist. This releases approximately 250 mcg per day over the implant's lifespan.
For research peptide formulations (subcutaneous injection), the community and available data suggest a phased approach:
Loading phase: 250-500 mcg daily for 7-14 days to establish a base level of melanin production. Some sources suggest starting at 250 mcg for 7-10 days.
Ramp phase: 500-1,000 mcg daily until desired skin tone is achieved.
Maintenance phase: 250-1,000 mcg administered 1-3 times per week to maintain results.
UV exposure is typically paired with the protocol. Most sources recommend starting with low UV exposure (3-5 minutes), increasing gradually by 30 seconds to 1 minute per session, with maximum sessions of 20-30 minutes. Sunscreen remains mandatory; Melanotan I enhances tanning but does not replace sun protection.
Cycle duration varies. There are no validated guidelines for optimal treatment length. Season-limited courses of 2-3 months during periods of increased sun exposure (summer months) are commonly discussed as a practical approach.
The Science
The only rigorously characterized dosing regimen is the Scenesse 16 mg subcutaneous implant administered every 60 days, with up to 6 implants per year for continuous photoprotection [6][7]. The cumulative daily release from the implant approximates 250 mcg/day based on pharmacokinetic modeling [4][8].
Human equivalent dose (HED) translation from murine photoprotective studies (effective dose ~0.1 mg/kg SC daily) yields approximately 0.5 mg/day for a 60 kg adult using the standard 12.3 conversion factor, which aligns with the implant's release profile [8].
Phase I human tanning studies used subcutaneous doses at 0.16 mg/kg three times weekly for 10 days [14][15]. In the Dorr et al. Phase I study of Melanotan II (the more potent cyclic analog), effective tanning doses were 0.01-0.025 mg/kg/day [5].
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Track injection timing, draw notes, and site rotation.
Doserly helps keep syringe-related notes, injection site history, reminders, and reconstitution context together for easier review.
Injection log
Site rotation
Injection logs support record-keeping; follow clinician instructions for administration.
What to Expect
Week 1-2 (Loading Phase):
Most users report minimal visible change during the first week. Some experience mild nausea and facial flushing, particularly with early doses. These side effects typically diminish within a few days as tolerance develops. A subtle warmth or slight skin tone shift may begin to appear toward the end of the second week, especially with paired UV exposure. Evening dosing and slow titration can help manage initial nausea.
Week 2-4 (Ramp Phase):
Visible tanning becomes apparent. Fair-skinned individuals (Fitzpatrick I/II) typically notice the most dramatic change during this period, as the base pigmentation shifts from absent to present. The tan tends to develop evenly across the body, though areas with more sun exposure may darken faster. Moles and freckles may begin to darken. Nausea should have resolved by this point for most users.
Week 4-8 (Established Phase):
The tan reaches its plateau at the current dose. Users report a stable, natural-looking skin tone. One ginger-haired user who had never tanned in 31 years reported being "gobsmacked" by the color change after approximately 8 weeks of combined MT-I use and moderate UV exposure. Community consensus is that the MT-I tan looks more natural and even compared to MT-II.
Week 8+ (Maintenance):
Once the desired skin tone is achieved, frequency can be reduced to maintenance dosing (commonly 1-3 times weekly). The tan persists for several weeks after discontinuation due to melanin's natural turnover cycle in the epidermis. Pigmentation fades gradually rather than abruptly.
Important notes: Results are highly individual and depend on skin type, dose, and UV exposure. Very fair-skinned individuals may require longer loading phases. Dermatologic monitoring should continue throughout use and after discontinuation.
The week-by-week expectations above are drawn from research and community reports, but your experience will be uniquely yours. Doserly's biomarker tracking transforms those general timelines into personal data points you can actually see and measure.
Log the specific markers relevant to this compound, whether that's pain levels, energy, sleep quality, body composition, recovery time, or mood, and watch your own trend lines emerge over weeks and months. Did your key markers start shifting in week three, like the research suggests? Is your experience tracking with what the community reports, or diverging? Over time, this creates something more valuable than any guide: an evidence-based picture of how your body responds to this specific compound, at your specific dose, within your specific health context.
See where a dose, cycle, or change fits in time.
Doserly gives each protocol a timeline so dose changes, pauses, restarts, and observations are easier to compare later.
Timeline
Cycle history
Timeline tracking helps with recall; it is not a treatment recommendation.
Interaction Compatibility
Good With (Potentially Synergistic)
- Glutathione — Antioxidant support for skin health; commonly paired in skin-focused protocols
- KPV — Anti-inflammatory tripeptide; may complement MC1R-mediated anti-inflammatory effects
- BPC-157 — Tissue repair peptide; general skin and tissue health support
- GHK-Cu — Copper peptide with skin remodeling and collagen-support properties; commonly combined in skin-focused stacks
- Narrowband UVB phototherapy — Clinically demonstrated synergy for vitiligo repigmentation [16]
Caution / Monitor
- Melanotan II — Same receptor family; concurrent use is redundant and may increase melanocortin receptor activation beyond intended levels
- PT-141 — Derived from MT-II; acts on MC4R. Concurrent use could increase melanocortin receptor stimulation
Not Good With (Contraindicated or Caution)
- Immunosuppressive medications — MT-I has immunomodulatory effects via MC1R; potential for unpredictable interaction
- Photosensitizing drugs — May alter the photoprotection equation in unexpected ways
- Active melanoma treatment — Contraindicated due to effects on melanocyte proliferation
Administration Guide
Materials required:
- Sterile insulin syringes (U-100, 0.5 mL or 1 mL)
- Alcohol swabs
- Bacteriostatic water for reconstitution
- Sharps disposal container
Recommended reconstitution solution: Bacteriostatic water (BAC water). The peptide is water-soluble and reconstitutes readily.
Timing considerations: There is no strong evidence for a specific optimal time of day. Some community members prefer evening dosing to minimize awareness of any transient nausea or flushing during sleep. The Scenesse implant is typically administered in the morning based on the rationale of ensuring eumelanin levels are established prior to peak daytime UV exposure. If pairing with UV exposure, administration at least 1-2 hours before sun or light therapy allows for initial receptor engagement.
Post-administration care:
- Monitor for nausea and flushing in the first 30-90 minutes post-dose, particularly during loading phase
- Light snack and ginger tea can help manage nausea
- Do not exceed recommended UV exposure durations
- Monitor existing moles and freckles using the ABCDE criteria
- Maintain regular dermatologic appointments for full-body skin exams
- Keep a log of doses, timing, and any symptoms
Supplies & Planning
Peptide vials: Melanotan I is typically available in 10 mg lyophilized vials from research peptide suppliers. Note that research peptide formulations are not equivalent to the FDA-approved Scenesse implant.
Reconstitution supplies:
- Bacteriostatic water (30 mL vial)
- Sterile insulin syringes (U-100) for reconstitution and injection
- Alcohol swabs for vial stoppers and injection sites
Storage containers: Keep vials refrigerated at 2-8C (35.6-46.4F) after reconstitution, protected from light. Lyophilized (unreconstituted) vials can be stored at -20C for extended periods or at 2-8C for shorter storage.
General planning notes: The number of vials needed depends on the dose and protocol duration chosen in consultation with a healthcare provider. Use the reconstitution calculator for preparation math at your specific concentration targets.
Storage & Handling
Lyophilized (unreconstituted):
- Long-term: -20C or below
- Short-term: 2-8C (refrigerator)
- Protected from light and moisture
- Stable for 24-36 months when properly stored
Reconstituted:
- Refrigerated at 2-8C (35.6-46.4F)
- Protected from light
- Use within 30 days of reconstitution
- Do not freeze reconstituted solution
- Label vial with reconstitution date
Handling best practices:
- Allow vial to reach room temperature before reconstitution
- Add bacteriostatic water gently along the vial wall; do not shake vigorously
- Swirl gently until fully dissolved (clear solution)
- Clean vial stopper with alcohol swab before each withdrawal
- Use a fresh sterile syringe for each injection
Lifestyle Factors
UV exposure management: Melanotan I enhances tanning but does not replace sun protection. Sunscreen use remains mandatory. Start with minimal UV exposure (3-5 minutes) and increase gradually. Maximum recommended session length is generally 20-30 minutes. Avoid tanning beds if possible; if used, reduce duration significantly compared to normal sessions.
Skin monitoring: Regular full-body skin examinations with a dermatologist are strongly recommended before, during, and after any melanocortin protocol. Photograph existing moles and freckles before starting to create a baseline for comparison. Report any changes in the ABCDE criteria immediately.
Bloodwork recommendations: While Melanotan I does not typically require extensive monitoring, the following are suggested for extended use:
- Comprehensive metabolic panel (CMP) including liver function (ALT, AST, ALP, bilirubin) annually
- Complete blood count (CBC) for general wellness
- Vitamin D (25-OH) if limiting sun exposure while using the peptide
Hydration: Adequate water intake supports overall skin health and may help mitigate nausea during the loading phase.
Sun exposure counseling: Users should be counseled against overexposure due to a potential false sense of protection. Increased melanin provides genuine UV shielding, but it does not make the skin impervious to damage.
Regulatory Status & Research Classification
United States (FDA): Afamelanotide is FDA-approved under the brand name Scenesse for increasing pain-free light exposure in adults with erythropoietic protoporphyria (EPP). Approved October 2019 with priority review and orphan drug designation (NDA 210797) [6]. Research peptide versions of Melanotan I sold by peptide suppliers are not the same as the FDA-approved pharmaceutical product and are not approved for human use.
European Union (EMA): Marketing authorization granted in 2014 under exceptional circumstances for EPP. In September 2025, the EMA removed the 4-implant-per-year cap, harmonizing with US labeling for year-round treatment [7].
United Kingdom (MHRA): Available for EPP treatment. Classification follows EMA guidance.
Australia (TGA): The TGA has issued warnings about melanotan products sold online, noting that unapproved melanotan is illegal to sell in Australia. The pharmaceutical implant for EPP is available through specialist prescribers.
Canada (Health Canada): Not specifically approved. Access may be available through special access programmes for EPP patients.
WADA Status: Melanotan I (afamelanotide) is not currently listed on the WADA Prohibited List, though athletes should verify current status before use.
Active Clinical Trials:
- Phase III vitiligo trial (CUV105): Over 200 patients enrolled as of May 2025, evaluating afamelanotide as monotherapy and adjunctive therapy [17]
- Phase II trials in actinic keratosis and polymorphous light eruption
- Phase IIa stroke feasibility study completed [23]
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is the difference between Melanotan I and Melanotan II?
Melanotan I (afamelanotide) is a linear 13-amino-acid peptide that primarily activates the MC1R receptor on skin cells, producing tanning with minimal off-target effects. Melanotan II is a cyclic 7-amino-acid peptide that non-selectively activates MC1R through MC5R, including brain receptors that cause appetite suppression and sexual arousal. MT-I is FDA-approved (Scenesse); MT-II has never completed clinical development and is not approved in any jurisdiction.
Does Melanotan I cause melanoma?
Based on the available evidence, MC1R activation appears to be photoprotective rather than cancer-promoting. The Addison's disease cohort (3,299 patients with chronic MC1R activation over 40 years) showed melanoma incidence numerically below expected rates. The afamelanotide clinical programme reports zero melanoma events across more than 1,000 patients over periods exceeding 10 years. However, no formal long-term carcinogenicity studies have been conducted, and regular dermatologic monitoring is recommended.
How long does it take to see results?
Based on community reports and clinical data, initial visible tanning typically begins within 1-2 weeks, with more noticeable results at 3-4 weeks. Fair-skinned individuals (Fitzpatrick I/II) may require longer loading phases. The tan persists for several weeks after discontinuation.
What are the most common side effects?
The most commonly reported side effects across clinical trials and community use include mild nausea, facial flushing, headache, and transient fatigue. These typically resolve within the first few days of use. Darkening of existing moles and freckles is expected and requires dermatologic monitoring.
Can I use Melanotan I without UV exposure?
Clinical data indicates that Melanotan I can increase melanin production without UV exposure. However, combining with low-level UV exposure enhances and accelerates the tanning response. This was demonstrated in the vitiligo trials where afamelanotide plus NB-UVB produced superior results to NB-UVB alone.
Is the research peptide the same as Scenesse?
No. Scenesse is a 16 mg bioresorbable subcutaneous implant manufactured by CLINUVEL Pharmaceuticals under pharmaceutical-grade conditions with FDA oversight. Research peptide versions of Melanotan I are not manufactured to the same standards, are not FDA-approved for human use, and are intended for research purposes only.
What bloodwork should I monitor?
Based on available sources, commonly recommended monitoring includes liver function tests (ALT, AST) annually for extended use, complete blood count, and Vitamin D levels if sun exposure is being limited. Regular dermatologic skin exams are considered essential.
Sources & References
[1] Sawyer TK, Sanfilippo PJ, Hruby VJ, et al. [Nle4, D-Phe7]-alpha-MSH: a highly potent alpha-melanotropin with ultralong biological activity. Proc Natl Acad Sci USA. 1980;77(10):5754-5758. PMID: 6777774.
[2] Mun Y, Kim W, Shin D. MC1R: Pharmacological and Therapeutic Aspects. Int J Mol Sci. 2023;24(15):12152. PMID: 37569558.
[3] Hruby VJ, Cai M, Cain J, et al. Approaches to the rational design of selective melanocortin receptor antagonists. Expert Opin Drug Discov. 2015;10(10):1057-1069. PMC4608743.
[4] Minder EI, Barman-Aksoezen J, Schneider-Yin X. Pharmacokinetics and Pharmacodynamics of Afamelanotide and its Clinical Use in Treating Dermatologic Disorders. Clin Pharmacokinet. 2017;56(8):815-823.
[5] Dorr RT, Lines R, Levine N, et al. Evaluation of melanotan-II, a superpotent cyclic melanotropic peptide in a pilot phase-I clinical study. Life Sci. 1996;58(20):1777-1784. PMID: 8637402.
[6] Langendonk JG, Balwani M, Anderson KE, et al. Afamelanotide for Erythropoietic Protoporphyria. N Engl J Med. 2015;373(1):48-59. PMID: 26132941. See also: FDA NDA 210797, Scenesse Label (revised August 2024).
[7] Biolcati G, Marchesini E, Sorge F, et al. Long-term observational study of afamelanotide in 115 patients with erythropoietic protoporphyria. Br J Dermatol. 2015;172(6):1601-1612. PMID: 25494545. See also: EMA EPAR: Scenesse.
[8] Clinuvel Pharmaceuticals clinical and research data. Afamelanotide mechanism of action and clinical pharmacology documentation.
[9] Bohm M, Luger TA, Hartmann K, et al. An overview of benefits and risks of chronic MC1R activation. J Eur Acad Dermatol Venereol. 2025;39:39-51. PMID: 39082868.
[10] Mykicki N, Herrmann AM, Schwab N, et al. Melanocortin-1 receptor activation is neuroprotective in mouse models of neuroinflammatory disease. Sci Transl Med. 2016;8(362):362ra146. PMID: 27797962.
[11] An JJ, Rhee Y, Kim SH, et al. Peripheral effect of alpha-melanocyte-stimulating hormone on fatty acid oxidation in skeletal muscle. J Biol Chem. 2007;282(5):2862-2870. PMID: 17127674.
[12] Wensink D, Langendonk JG, Eekhoff EMW, et al. Afamelanotide for prevention of phototoxicity in erythropoietic protoporphyria. Expert Rev Clin Pharmacol. 2021;14(2):151-160.
[13] Barsh GS. What controls variation in human skin color? PLoS Biol. 2003;1(1):e27.
[14] Levine N, Sheftel SN, Eytan T, et al. Effect of MELANOTAN, [Nle4, D-Phe7]-alpha-MSH, on melanin synthesis in humans with MC1R variant alleles. J Invest Dermatol. 2006;126(12):2697. PMID: 16293341.
[15] Barnetson RS, Ooi TK, Zhuang L, et al. [Nle4-D-Phe7]-alpha-melanocyte-stimulating hormone significantly increased pigmentation and decreased UV damage in fair-skinned Caucasian volunteers. J Invest Dermatol. 2006;126(8):1869-1878. PMID: 16763546.
[16] Lim HW, Grimes PE, Agbai O, et al. Afamelanotide and Narrowband Ultraviolet B Phototherapy for the Treatment of Vitiligo: A Randomized Multicenter Trial. JAMA Dermatol. 2015;151(1):42-50. PMID: 25230094.
[17] CLINUVEL Pharmaceuticals. Phase III vitiligo trial CUV105 recruits 200 patients. Press release, May 2025.
[18] Giuliani D, Neri L, Canalini F, et al. Melanocortins protect against progression of Alzheimer's disease in triple-transgenic mice by targeting multiple pathophysiological pathways. Neurobiol Aging. 2014;35(3):537-547. PMID: 24094579.
[19] Giuliani D, Galantucci M, Neri L, et al. Melanocortins protect against brain damage and counteract cognitive decline in a transgenic mouse model of moderate Alzheimer's disease. Eur J Pharmacol. 2014;740:144-150. PMID: 25034807.
[20] Borse SP, Chhipa AS, Sharma V, et al. NDP-alpha-MSH induces intense neurogenesis and cognitive recovery in Alzheimer transgenic mice through activation of melanocortin MC4 receptors. Mol Cell Neurosci. 2015;67:13-21. PMID: 26003413.
[21] Caruso V, Lagerström MC, Olszewski PK, et al. Melanocortin 4 receptor activates ERK-cFos pathway to increase brain-derived neurotrophic factor expression in rat astrocytes and hypothalamus. Mol Cell Endocrinol. 2014;386(1-2):52-62. PMID: 25892444.
[22] Spaccapelo L, Galantucci M, Neri L, et al. Functional recovery after delayed treatment of ischemic stroke with melanocortins is associated with overexpression of the activity-dependent gene Zif268. Brain Behav Immun. 2011;25(1):80-90. PMID: 19345727.
[23] Stanislaus V, Treharne M, Horne C, et al. A feasibility and safety study of afamelanotide in acute stroke patients. BMC Neurol. 2023;23(1):281.
[24] Ni XP, Bhargava A, Bhargava P, et al. alpha-MSH analogue attenuates blood pressure elevation in DOCA-salt hypertensive mice. Kidney Int. 2006;69(11):1857-1858. PMID: 23977363.
[25] Bazzani C, Guarini S, Botticelli AR, et al. Protective effects of the melanocortin analog NDP-alpha-MSH in rats undergoing cardiac arrest. Eur J Pharmacol. 2001;423(1):37-43. PMID: 25446929.
[26] Taylor AW, Yee DG, Nishida T, et al. Immunosuppressive activity of a novel peptide analog of alpha-melanocyte stimulating hormone in experimental autoimmune uveitis. J Neuroimmunol. 2005;161(1-2):185-191. PMID: 21640392.
[27] Hao L, Sheng Z, Potian J, et al. Characterization of murine melanocortin receptors mediating adipocyte lipolysis and examination of signaling pathways involved. Regul Pept. 2011;163(1-3):50-56. PMID: 21616121.
Related Peptide Guides
- Melanotan II — Cyclic melanocortin agonist; non-selective MC1R-MC5R activation; tanning, appetite, and libido effects
- PT-141 (Bremelanotide) — Derived from Melanotan II research; MC4R agonist FDA-approved for hypoactive sexual desire disorder
- KPV — Alpha-MSH C-terminal tripeptide; anti-inflammatory properties via different mechanism
- Glutathione — Antioxidant commonly paired with melanocortin peptides in skin-focused protocols
- GHK-Cu — Copper peptide with skin remodeling properties; complementary in skin health stacks
- BPC-157 — Tissue repair peptide; general recovery and healing support
Need the reconstitution math for Melanotan I: Complete Research Guide?
Open the calculator with Melanotan I: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.