Kisspeptin: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Kisspeptin-10, KP-10, Metastin 45-54, KISS-1 Decapeptide, KiSS-1 (45-54), Metastin (45-54) Amide
Attribute
Administration
- Detail
- Injectable (subcutaneous); intranasal spray (reported in community use)
Attribute
Research Status
- Detail
- Research Compound; active clinical trials for reproductive endocrinology (Imperial College London); not FDA-approved for therapeutic use
Attribute
Typical Dose Range
- Detail
- 50-300 mcg per administration; frequency and route vary by protocol
Attribute
Half-Life
- Detail
- Approximately 28 minutes (kisspeptin-54, IV); shorter for kisspeptin-10 (estimated minutes)
Attribute
Cycle Length
- Detail
- 4-12 weeks with planned washout periods to avoid tachyphylaxis
Attribute
Storage
- Detail
- Lyophilized: -20°C for long-term; Reconstituted: 2-8°C, use within 28 days
Overview / What Is Kisspeptin?
The Basics
Kisspeptin is a naturally occurring hormone produced in a small region of your brain called the hypothalamus. Its job is straightforward but critical: it tells your body to start making sex hormones. Without kisspeptin, the entire hormonal cascade that drives testosterone production, estrogen production, fertility, and sexual function simply does not fire.
Think of your reproductive hormone system as a relay race. Kisspeptin is the starting gun. When it fires, it triggers gonadotropin-releasing hormone (GnRH), which passes the baton to luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which then tell the testes or ovaries to produce testosterone, estrogen, and mature reproductive cells. If the starting gun fails, nothing downstream moves.
This is why kisspeptin has attracted intense research interest. People whose kisspeptin system is impaired, whether through genetic mutations, stress, extreme dieting, or the aftereffects of certain medications, can experience reproductive shutdown: low testosterone, absent periods, infertility, and diminished libido. Clinical researchers have explored whether administering kisspeptin externally can restart that system, and the early results are promising [1][2].
The name itself comes from Hershey, Pennsylvania, where the KISS1 gene was discovered at Penn State Hershey Medical Center. The "KISS" in KISS1 stands for the Hershey Kisses, not an acronym [3]. Beyond reproduction, research has revealed that kisspeptin also plays roles in mood, emotional processing, energy balance, and even cancer metastasis suppression, making it one of the more multifaceted neuropeptides under active investigation.
The Science
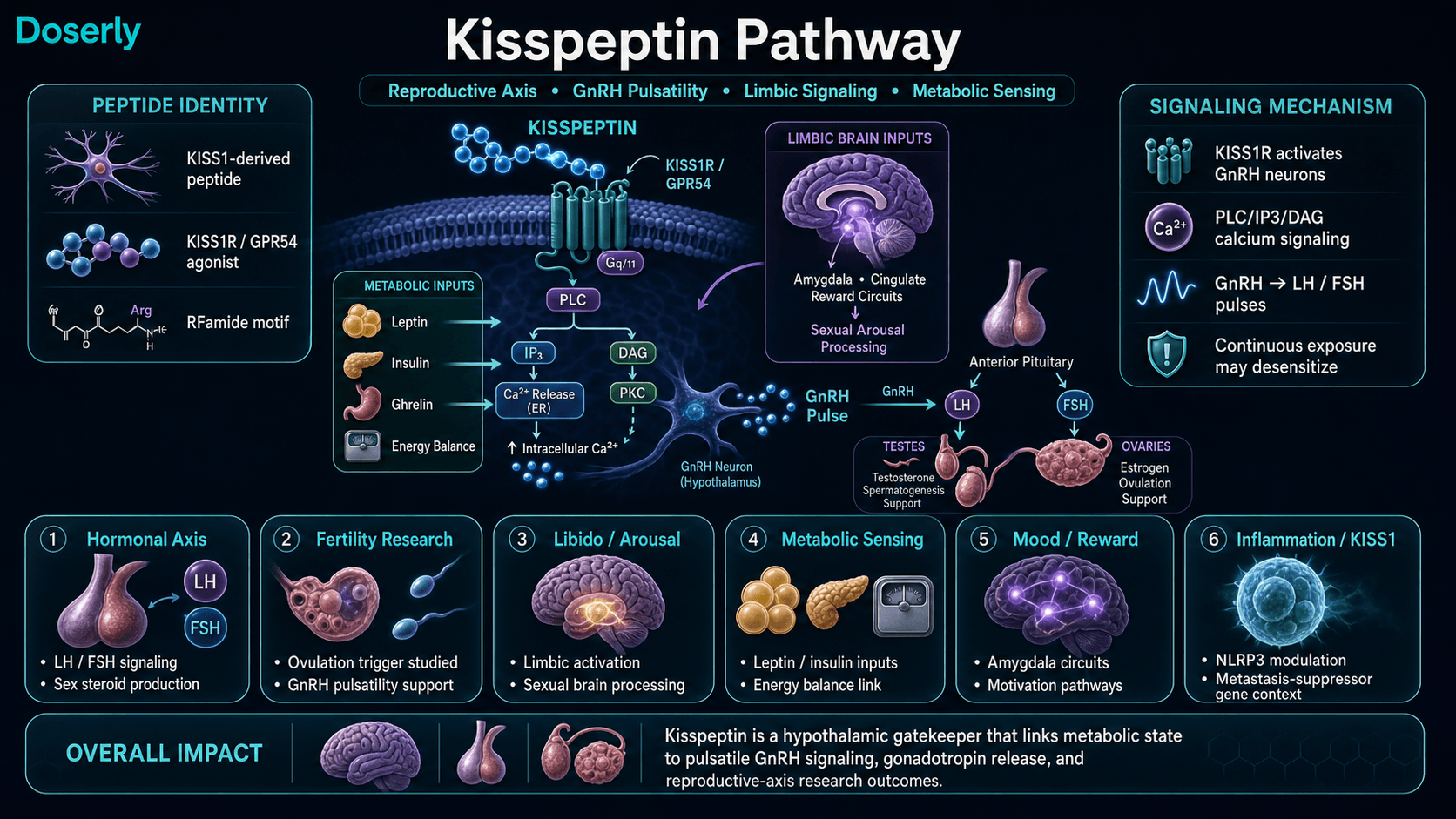
Kisspeptin refers to a family of neuropeptides encoded by the KISS1 gene (originally identified as a metastasis-suppressor gene in melanoma), with kisspeptin-10 (KP-10) being the C-terminal decapeptide fragment most commonly used in research applications. The full-length gene product, kisspeptin-54 (also called metastin), undergoes proteolytic processing to generate active fragments of varying lengths (kisspeptin-54, -14, -13, and -10), all sharing an identical C-terminal RFamide motif (Arg-Phe-NH2) that is essential for receptor activation [1][3].
Kisspeptin acts through the kisspeptin receptor KISS1R (formerly designated GPR54), a G-protein coupled receptor expressed on GnRH neurons in the arcuate and anteroventral periventricular nuclei of the hypothalamus. Receptor binding activates Gq/11-mediated signaling, triggering phospholipase C activation, IP3 generation, and intracellular calcium mobilization, resulting in depolarization of GnRH neurons and pulsatile GnRH secretion [1][4].
Loss-of-function mutations in either KISS1 or KISS1R cause hypogonadotropic hypogonadism and failure of puberty in humans, establishing kisspeptin as an indispensable gatekeeper of reproductive function [4]. Conversely, gain-of-function mutations in KISS1R have been associated with precocious puberty [5].
Clinical studies at Imperial College London have demonstrated that exogenous kisspeptin administration can stimulate gonadotropin secretion in both healthy volunteers and patients with reproductive disorders, including hypoactive sexual desire disorder (HSDD), where kisspeptin enhanced sexual brain processing via limbic pathway activation [2][6].
Molecular Identity
Attribute
Common Names
- Detail
- Kisspeptin-10, KP-10, Metastin 45-54, KISS-1 Decapeptide
Attribute
Amino Acid Sequence
- Detail
- H-Tyr-Asn-Trp-Asn-Ser-Phe-Gly-Leu-Arg-Phe-NH2 (YNWNSFGLRF)
Attribute
Sequence Length
- Detail
- 10 amino acids (decapeptide)
Attribute
Molecular Formula
- Detail
- C63H83N17O14
Attribute
Molecular Weight
- Detail
- 1302.4 g/mol
Attribute
CAS Number
- Detail
- 374675-21-5 (human kisspeptin-10)
Attribute
PubChem CID
- Detail
- 25240297
Attribute
UniProt
- Detail
- Q15726 (human kisspeptin/metastin precursor protein)
Attribute
NCBI Gene ID
- Detail
- 3881 (human KISS1 gene)
Attribute
Structural Type
- Detail
- Linear peptide with C-terminal amidation; RFamide motif
Attribute
Salt Forms
- Detail
- Free peptide, acetate salt, trifluoroacetate salt; lyophilized powder
Attribute
Key Features
- Detail
- Tryptophan at position 3 critical for receptor binding; RFamide C-terminus essential for all biological activity; highly conserved across mammalian species
All kisspeptin variants (10, 13, 14, 54) share the identical C-terminal decapeptide sequence, meaning kisspeptin-10 contains the minimum active fragment necessary for full KISS1R activation [1].
Mechanism of Action
The Basics
Kisspeptin works by waking up your body's own hormone-production system at the very top of the chain. Rather than replacing testosterone or estrogen directly (as hormone replacement therapy does), kisspeptin tells the brain to restart the natural signaling process.
Here is how the cascade works: kisspeptin binds to receptors on specific brain cells (GnRH neurons) in the hypothalamus. These neurons then release GnRH in rhythmic pulses. Each GnRH pulse tells the pituitary gland to release LH and FSH. LH then acts on the testes (in men) to produce testosterone, or on the ovaries (in women) to trigger ovulation and produce estrogen. FSH supports sperm production in men and egg development in women.
This is an important distinction from direct hormone replacement. Testosterone replacement therapy (TRT) provides the end product but shuts down your brain's signaling system in the process, because the brain senses enough testosterone and stops sending the "make more" signal. Kisspeptin works at the top of the chain, preserving (and in some cases restoring) the body's own production capability [1][7].
Kisspeptin also has effects beyond reproduction. Receptors for kisspeptin have been found in the limbic system (the brain's emotional and reward centers), which may explain why some people report improvements in mood, drive, and sexual desire that seem to go beyond what testosterone changes alone would predict [6].
The Science
Kisspeptin-10 binds to the KISS1R (GPR54) receptor on GnRH neurons, activating Gq/11-coupled intracellular signaling. This triggers phospholipase C (PLC)-mediated hydrolysis of phosphatidylinositol 4,5-bisphosphate (PIP2), generating inositol 1,4,5-trisphosphate (IP3) and diacylglycerol (DAG). IP3-mediated calcium release from intracellular stores depolarizes GnRH neurons, stimulating pulsatile GnRH secretion into the hypophyseal portal system [1][4].
Critically, kisspeptin's action is entirely GnRH-dependent. GnRH antagonist co-administration abolishes kisspeptin-induced LH/FSH secretion, confirming that kisspeptin does not act directly on the pituitary but rather through GnRH neuron activation [8].
Kisspeptin neurons integrate metabolic signals (leptin, insulin, ghrelin) with reproductive output. Under conditions of negative energy balance, kisspeptin neuron activity is suppressed, mediating the well-characterized link between energy deficit and reproductive suppression (hypothalamic amenorrhea, exercise-induced hypogonadism) [9].
Additionally, KISS1R expression in the limbic brain (amygdala, hippocampus, cingulate cortex) provides the neuroanatomical substrate for kisspeptin's effects on sexual arousal and emotional processing demonstrated in human fMRI studies [6].
The NLRP3 inflammasome inhibition observed with kisspeptin-10 suggests anti-inflammatory properties that may contribute to cardiovascular and renal effects beyond the reproductive axis [10].
Pathway Visualization Image
Pharmacokinetics
The Basics
Kisspeptin works fast but does not stay in the bloodstream for long. After injection, it reaches the brain within minutes and begins triggering GnRH release almost immediately. The LH surge that follows typically peaks within 30 to 60 minutes.
The rapid clearance is actually a feature, not a bug. Your body's natural kisspeptin signaling works in pulses, not as a continuous stream. Short bursts followed by pauses allow the GnRH receptors to reset between signals. When kisspeptin is present continuously (or dosed too frequently), the receptors stop responding. This phenomenon, called tachyphylaxis or receptor desensitization, is one of the most important practical considerations for anyone researching this peptide [11].
This is why researchers who study kisspeptin protocols tend to favor intermittent dosing (a few times per week with rest days) rather than daily injections, even though daily protocols appear in some community discussions [11][12].
The Science
Kisspeptin-54 administered intravenously demonstrates a plasma half-life of approximately 28 minutes, with peak LH response occurring within 30-60 minutes post-infusion [1][13]. Kisspeptin-10, being a smaller fragment, is expected to have an even shorter half-life due to increased susceptibility to enzymatic degradation by matrix metalloproteinases and other serum peptidases.
Subcutaneous bioavailability has not been precisely characterized in published human pharmacokinetic studies. Community reports suggest intranasal administration is also viable, though bioavailability by this route is unquantified.
A critical pharmacodynamic consideration is tachyphylaxis: continuous or twice-daily subcutaneous administration of kisspeptin-54 over 14 days in women with hypothalamic amenorrhea produced initial robust LH/FSH responses that progressively diminished, with significantly reduced gonadotropin responses by day 14 compared to acute administration [11]. This phenomenon parallels the well-characterized downregulation seen with continuous GnRH agonist exposure and argues strongly for intermittent, pulsatile administration schedules.
Research & Clinical Evidence
Reproductive Hormone Stimulation
The Basics
The most well-studied effect of kisspeptin is its ability to stimulate reproductive hormones. In healthy men, even small doses produce rapid, measurable increases in LH and testosterone. In one study, a brief kisspeptin infusion doubled the frequency of LH pulses and significantly raised testosterone levels within 90 minutes [14].
For women, kisspeptin has shown promise in conditions where the brain's hormonal signaling has shut down. In functional hypothalamic amenorrhea (where periods stop due to stress, extreme exercise, or low body weight), kisspeptin administration restored GnRH and LH pulsatility, suggesting it could help restart the menstrual cycle [15].
The Science
George et al. (2011) demonstrated that intravenous kisspeptin-10 administration in healthy men produced dose-dependent increases in LH pulse frequency and amplitude, with concomitant testosterone elevation [14]. Dhillo et al. (2005) showed that kisspeptin-54 infusion (4 pmol/kg/min over 90 minutes) stimulated robust LH, FSH, and testosterone responses in six healthy men, establishing proof-of-mechanism for the kisspeptin-GnRH-LH/FSH-testosterone cascade in humans [13].
Jayasena et al. (2009) investigated twice-daily subcutaneous kisspeptin-54 in women with hypothalamic amenorrhea. Acute responses were robust, with significant LH/FSH elevations, but tachyphylaxis developed by approximately day 14 of continuous administration [11].
IVF and Ovulation Triggering
The Basics
One of the most exciting clinical applications is using kisspeptin to trigger ovulation during IVF (in vitro fertilization). The standard ovulation trigger, hCG, carries a risk of ovarian hyperstimulation syndrome (OHSS), a potentially dangerous condition. Kisspeptin triggers ovulation through a more physiological pathway and appears to carry a lower OHSS risk, making it particularly valuable for high-risk patients [16].
The Science
Abbara et al. (2015) demonstrated that a single subcutaneous injection of kisspeptin-54 effectively triggered oocyte maturation in women undergoing IVF, with successful egg retrieval and fertilization rates. Importantly, kisspeptin triggering was associated with a reduced risk of OHSS compared to conventional hCG triggering, attributed to the more physiological, self-limiting nature of kisspeptin-induced LH surges [16].
Sexual Desire and Brain Processing
The Basics
Kisspeptin does something that simple testosterone boosting does not: it appears to activate the brain's sexual and emotional processing centers directly. In clinical trials, people given kisspeptin showed increased brain activity in areas associated with sexual arousal, reward-seeking, and attraction, even before measurable testosterone changes occurred. This suggests kisspeptin has a direct effect on sexual desire at the brain level, separate from its hormonal effects [6].
This finding has generated interest for conditions like hypoactive sexual desire disorder (HSDD), where people have low sexual interest that causes personal distress. Two clinical trials (one in 32 women, one in 32 men with HSDD) showed kisspeptin administration improved sexual brain processing and sexual behavior compared to placebo [2].
The Science
Comninos et al. (2017) demonstrated via fMRI that intravenous kisspeptin-54 (1 nmol/kg/h over 75 minutes) enhanced limbic and hypothalamic activation in response to sexual and bonding stimuli in healthy men, with concurrent modest LH elevation. The enhanced brain responses were observed in the amygdala, cingulate cortex, and globus pallidus, regions involved in sexual arousal, emotional processing, and reward [6].
Mills et al. (2023) and Comninos et al. (2023) extended these findings to patients with HSDD, demonstrating in two JAMA Network Open-published trials that kisspeptin administration improved sexual brain processing in both pre-menopausal women (N=32) and men (N=32) with clinically diagnosed HSDD [2].
Energy Balance and Metabolic Regulation
The Basics
Kisspeptin neurons serve as metabolic sensors. Research shows they respond to your nutritional status: undereating or extreme overweight can suppress kisspeptin activity, which is one reason why extreme dieting can cause menstrual irregularity or low testosterone. Interestingly, kisspeptin itself may also influence energy expenditure. Mice lacking the kisspeptin receptor showed increased body fat and reduced energy expenditure, with kisspeptin receptors identified in fat tissue [9][17].
The Science
Navarro (2020) reviewed the bidirectional relationship between kisspeptin and metabolic homeostasis. Kisspeptin neurons in the arcuate nucleus express receptors for leptin, insulin, and ghrelin, positioning them as integrators of metabolic state and reproductive output. Kiss1r knockout mice exhibit increased adiposity and decreased energy expenditure, with KISS1R expression confirmed in white and brown adipose tissue, suggesting direct peripheral metabolic actions [9].
Cancer Metastasis Suppression
The Basics
The KISS1 gene was originally discovered not as a reproductive hormone but as a metastasis suppressor. Research has shown that kisspeptin can suppress the spread of cancer cells by reducing their ability to migrate and invade other tissues. Decreased kisspeptin levels have been found across many metastatic cancer types, including breast, prostate, bladder, pancreatic, ovarian, and skin cancers [3][18].
The Science
The KISS1 gene was identified in 1996 as a metastasis suppressor gene in melanoma, with kisspeptin expression capable of suppressing metastasis by up to 95% without affecting primary tumor growth [3]. The anti-metastatic mechanism involves inhibition of cancer cell migration, potentially through modulation of angiogenesis and cell adhesion pathways. Ly et al. (2020) reviewed the complex and sometimes paradoxical roles of KISS1 in various cancer types, noting that while reduced KISS1 expression generally correlates with increased metastatic potential, the relationship varies across tumor types [18].
Biomarker Evidence Matrix
The following matrix summarizes available evidence across Doserly's biomarker tracking categories. Evidence Strength reflects the quality of published research (human trials, animal studies, in-vitro data). Reported Effectiveness reflects community-reported outcomes from the sentiment analysis.
Category
Libido
- Evidence Strength
- 8/10
- Reported Effectiveness
- 8/10
- Summary
- Human clinical trials demonstrate enhanced sexual brain processing and desire via limbic activation. Community reports consistently describe dramatic libido restoration, particularly in sexually dysfunctional populations.
Category
Sexual Function
- Evidence Strength
- 7/10
- Reported Effectiveness
- 7/10
- Summary
- Clinical data shows LH/FSH/testosterone stimulation supporting sexual function. Community reports improved erection quality, morning erections, and orgasm quality.
Category
Hormonal Symptoms
- Evidence Strength
- 8/10
- Reported Effectiveness
- 7/10
- Summary
- Strong human data: kisspeptin reliably increases LH, FSH, and downstream sex steroids. Multiple community reports include lab-verified testosterone increases. Estradiol elevation risk noted.
Category
Mood & Wellbeing
- Evidence Strength
- 6/10
- Reported Effectiveness
- 6/10
- Summary
- fMRI studies show limbic activation and reward-seeking behavior enhancement. Community reports modest mood improvements, though difficult to isolate from sexual restoration.
Category
Motivation & Drive
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Clinical studies show reward-seeking behavior increase. Community reports link to restored libido/sexual confidence; independent motivation effects unclear.
Category
Energy Levels
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Animal data on metabolic regulation via Kiss1r in adipose tissue. Sparse community reports of subtle energy improvement.
Category
Sleep Quality
- Evidence Strength
- 2/10
- Reported Effectiveness
- 4/10
- Summary
- No direct sleep research. One community report of severe sleep disruption attributed to secondary estradiol elevation, not direct kisspeptin effect.
Category
Focus & Mental Clarity
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Animal study on kissorphin (kisspeptin analog) improving spatial memory. Minimal community discussion.
Category
Side Effect Burden
- Evidence Strength
- 7/10
- Reported Effectiveness
- 6/10
- Summary
- Clinical trials report excellent short-term tolerability. Community largely confirms mild side effect profile with notable estradiol-related risk on prolonged daily use.
Categories with insufficient data for scoring: Fat Loss, Muscle Growth, Weight Management, Appetite & Satiety, Food Noise, Memory & Cognition, Anxiety, Stress Tolerance, Emotional Aliveness, Emotional Regulation, Joint Health, Inflammation, Pain Management, Recovery & Healing, Physical Performance, Gut Health, Digestive Comfort, Nausea & GI Tolerance, Skin Health, Hair Health, Heart Health, Blood Pressure, Heart Rate & Palpitations, Temperature Regulation, Fluid Retention, Body Image, Immune Function, Bone Health, Longevity & Neuroprotection, Cravings & Impulse Control, Social Connection, Daily Functioning.
Benefits & Potential Effects
The Basics
Kisspeptin's most compelling benefit is its ability to restart your body's own hormone production rather than replacing it from the outside. For men, this means the potential for increased testosterone, improved libido, and better fertility while keeping the testes active and sperm production running. For women, it may help restore menstrual regularity, support ovulation, and improve fertility, particularly in cases where hormonal signaling has shut down due to stress or low body weight.
Beyond hormone production, kisspeptin appears to influence sexual desire at the brain level. This is notable because many people with low libido have adequate hormone levels on blood tests but still feel no desire. Kisspeptin's action on brain circuits involved in attraction, arousal, and emotional connection may address this gap where testosterone alone cannot.
The IVF application is also significant. For women undergoing fertility treatment who are at risk of ovarian hyperstimulation syndrome, kisspeptin offers a potentially safer way to trigger egg maturation compared to the standard hCG trigger [16].
The Science
Demonstrated benefits from human clinical data include:
- Gonadotropin stimulation: Dose-dependent increases in LH pulse frequency and amplitude, with downstream testosterone elevation in men [13][14] and restoration of GnRH pulsatility in hypothalamic amenorrhea [15].
- Sexual brain processing: Enhanced limbic activation (amygdala, cingulate cortex) in response to sexual stimuli, independent of testosterone changes, observed in both healthy volunteers and HSDD patients [2][6].
- IVF ovulation triggering: Effective oocyte maturation triggering with reduced OHSS risk compared to hCG [16].
- Metabolic integration: Kisspeptin neurons integrate metabolic signals with reproductive output; KISS1R identified in adipose tissue with potential direct effects on energy expenditure [9].
- Anti-metastatic activity: KISS1-mediated suppression of cancer cell migration demonstrated across multiple tumor types, though clinical therapeutic development remains in early stages [3][18].
The benefits outlined above span multiple body systems, and your experience will be uniquely yours. Rather than guessing which effects are attributable to this compound versus other factors in your life, Doserly helps you log specific outcomes alongside your protocol details, building a clear picture of what's changing and when.
Over weeks and months, this creates something more useful than any anecdotal report: your own evidence-based record of how this compound affects you personally, at your specific dose, within the context of your full health protocol. When it's time to decide whether to continue, adjust, or discontinue, you have real data to inform that conversation with your healthcare provider.
Keep sensitive protocol records in a purpose-built app.
Doserly is designed for private health tracking with structured records, offline-ready workflows, and exportable history when you need it.
Privacy
Health records
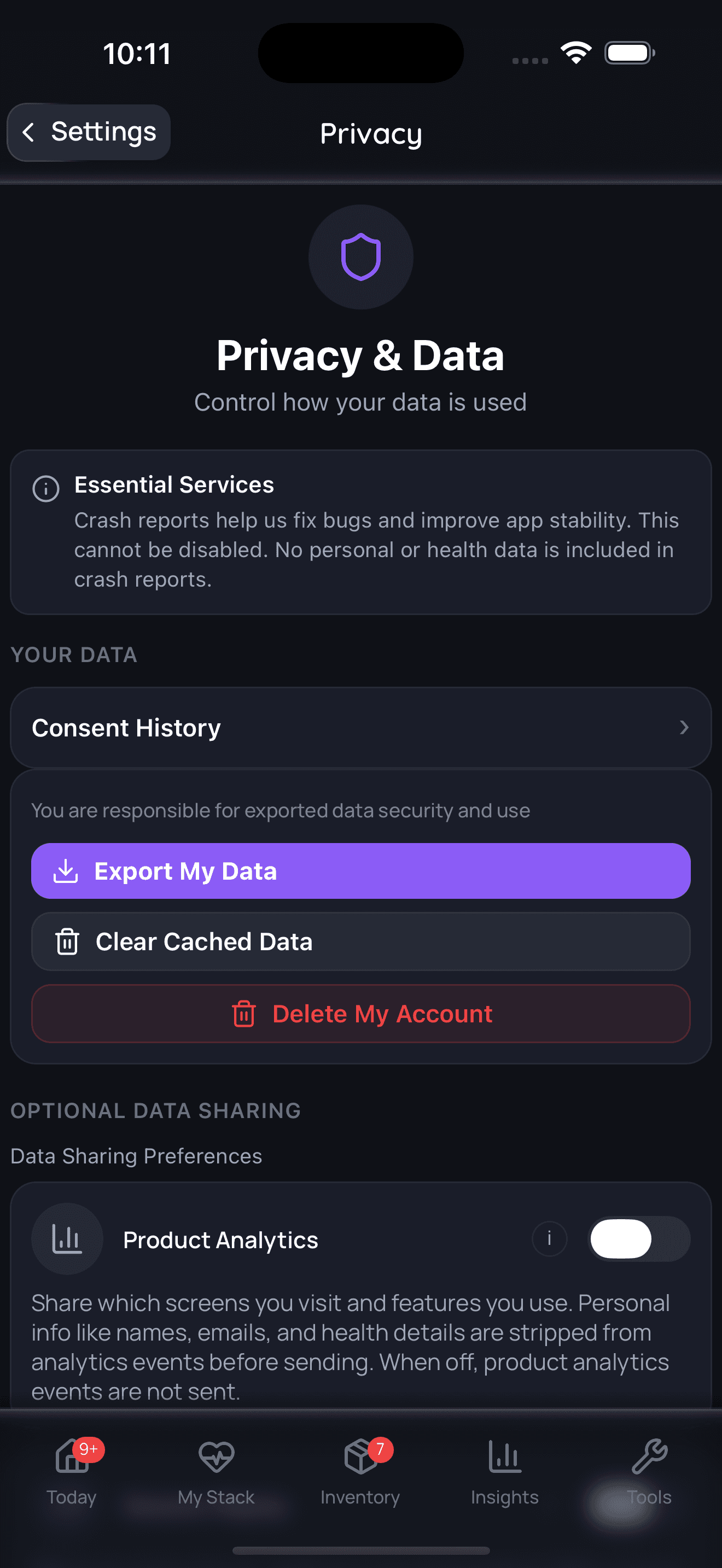
Privacy controls help you manage records; keep clinical records where required.
Side Effects & Safety Considerations
The Basics
Kisspeptin is generally well tolerated in clinical studies and community reports. The most commonly mentioned side effects are mild and transient: slight redness at the injection site, brief flushing, mild headache, and occasional nausea. These typically resolve quickly and are not considered serious [1][2].
The more significant concern is not a direct side effect of kisspeptin itself but a downstream consequence: because kisspeptin increases testosterone (and testosterone can be converted to estradiol by the aromatase enzyme), prolonged use can lead to elevated estradiol levels. One well-documented community report described estradiol doubling over three months of daily use, causing poor sleep, heavy legs, and emotional instability. These symptoms resolved after stopping kisspeptin and managing estradiol with an aromatase inhibitor.
The other critical safety consideration is tachyphylaxis: using kisspeptin too frequently or continuously causes the receptors to stop responding, diminishing or eliminating the desired effects. Clinical data shows this can begin within as few as two weeks of twice-daily dosing [11]. This is not a typical "side effect" in the traditional sense, but it is arguably the most important practical safety issue to understand.
Kisspeptin should be avoided during pregnancy (safety unknown), in the presence of hormone-dependent cancers (prostate, breast, endometrial), and in uncontrolled hypothalamic or pituitary pathology [1].
The Science
Clinical trial safety data:
- Injection site reactions: Mild, transient erythema and pruritus at subcutaneous injection sites, consistent with other peptide formulations [1][2].
- Cardiovascular: One community report of mild tachycardia (10-15 bpm increase lasting approximately 30 minutes post-injection). No significant cardiovascular adverse events reported in clinical trials.
- Hormonal: Secondary estradiol elevation due to increased aromatization of kisspeptin-stimulated testosterone. This is a dose- and duration-dependent risk, particularly relevant for prolonged daily protocols.
- Tachyphylaxis: Jayasena et al. (2009) demonstrated declining LH responses over 14 days of twice-daily subcutaneous kisspeptin-54, establishing that continuous exposure leads to KISS1R desensitization [11].
- Contraindications: Hormone-dependent malignancies (theoretical risk of stimulating hormone-sensitive tumor growth), pregnancy/lactation (no safety data), uncontrolled hypothalamic/pituitary disease.
Side effect profiles are most useful when you can compare them against your own experience in real time. Doserly lets you log symptoms, severity, and timing alongside your dosing data, creating a side-by-side view of your protocol and your body's response.
This kind of systematic tracking catches things that memory alone misses. A subtle mood shift that began three days after a dose increase. Sleep disruption that correlates with evening administration. These patterns become visible when the data is laid out on a timeline, and they give your healthcare provider actionable information rather than vague concerns. Early detection of emerging side effects means earlier intervention.
Keep side effects, flags, and follow-up notes visible.
Doserly helps you document safety observations, side effects, medication changes, and follow-up questions so important context is not scattered.
Safety log
Flags and notes

Safety notes are not emergency guidance; seek medical help when appropriate.
Dosing Protocols
The Basics
Dosing kisspeptin correctly is more nuanced than most peptides because of the tachyphylaxis issue described above. The receptors need time between doses to reset, which means "more is not better" and daily dosing is not necessarily optimal.
Sources report a wide range of protocols. The most commonly cited approach across reference sites is 100-200 mcg per day subcutaneously for 8-12 weeks. However, clinical trial data and evidence-based community sources argue that this daily approach may lead to receptor desensitization (tachyphylaxis) within as few as two weeks, reducing or eliminating the peptide's effectiveness [11].
A more evidence-aligned protocol cited by clinically oriented community sources uses higher individual doses (equivalent to roughly 3-5 nmol/kg body weight) administered three times per week with at least 48 hours between injections, in cycles of 3-4 weeks on followed by a 1-week washout, with a longer 2-week washout after the second cycle. This intermittent approach aims to maintain receptor sensitivity over time [11][12].
Gender-specific considerations have been noted. Some sources suggest women may use lower doses (50-150 mcg per administration), particularly when targeting specific phases of the menstrual cycle (follicular phase through ovulation window).
All protocols should include monitoring of LH, FSH, testosterone (men) or estradiol (women), and estradiol (men, to catch elevation). Lab assessment is recommended at baseline and periodically during use to guide dosing adjustments. Anyone considering research with this compound should discuss protocol design with a qualified healthcare provider.
The Science
Published human study protocols:
- Dhillo et al. (2005): Kisspeptin-54, 4 pmol/kg/min IV infusion over 90 minutes in healthy men [13].
- George et al. (2011): Kisspeptin-10, microgram-scale IV bolus and infusion in healthy men, demonstrating dose-dependent LH pulse frequency increases [14].
- Jayasena et al. (2009): Kisspeptin-54, subcutaneous twice daily over 2 weeks in hypothalamic amenorrhea; demonstrated tachyphylaxis by day 14 [11].
- Comninos et al. (2017): Kisspeptin-54, 1 nmol/kg/h IV over 75 minutes in healthy men [6].
- Abbara et al. (2015): Kisspeptin-54, single subcutaneous injection for IVF ovulation triggering [16].
No standardized subcutaneous dosing protocol for kisspeptin-10 has been established through controlled clinical trials. The community-reported ranges (100-300 mcg subcutaneous) are extrapolated from clinical kisspeptin-54 data and empirical observation.
The dosing protocols above involve numbers that matter: specific microgram amounts, reconstitution ratios, and timing windows. Getting any of these wrong compounds across every subsequent dose from that vial.
Doserly's dose and reconstitution calculators eliminate the guesswork. Enter your vial size, peptide amount, and target dose, and get the exact bacteriostatic water volume, units per tick mark, and doses per vial. The injection site tracker maps your administration history as a visual heat map across your body, flagging areas that need rest and suggesting rotation patterns. Combined with dose reminders that include compound name, amount, and route, every aspect of your daily protocol is handled with the precision it requires.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders

Reminder tracking supports consistency; it does not select a protocol for you.
What to Expect
Timelines reported in community experiences and clinical studies suggest the following general progression, though individual responses vary significantly:
Week 1-2: Some users report subtle effects within days, including a slight improvement in energy and the first signs of increased libido. Morning erections may begin to return. These early effects are often described as "subtle but noticeable." Clinical studies show measurable LH and testosterone increases within hours of the first dose, though full hormonal adaptation takes longer [13][14].
Week 2-4: Effects typically become more pronounced. Libido improvement is the most consistently reported change during this period. Users report increased sexual interest, improved erection quality, and a return of what some describe as "the spark" of sexual desire. Mood may improve. Blood work during this period generally shows LH and testosterone elevation [14].
Week 4-8: For those on well-designed intermittent protocols, benefits tend to stabilize. Hormonal improvements should be reflected in lab work. If on a daily protocol without washouts, this is the window where tachyphylaxis may begin to emerge, with diminishing returns in both subjective experience and lab values [11].
After cycle completion: Upon discontinuation, some users report a gradual return of pre-treatment symptoms over days to weeks. This appears to be a return to baseline rather than a withdrawal effect. Some community members report sustained improvements after a full cycle, suggesting potential lasting benefits to HPG axis function, though this is not established in clinical literature.
Interaction Compatibility
Good With (Commonly Reported Synergistic Combinations)
- HCG: Used alongside kisspeptin in fertility and HPG axis restoration protocols. HCG acts directly on the testes (mimicking LH) while kisspeptin works upstream at the hypothalamic level. Some community members use both, though others report kisspeptin alone is more effective for libido than HCG.
- Gonadorelin: Both act on the HPG axis at different levels. Gonadorelin is synthetic GnRH; kisspeptin stimulates endogenous GnRH release. The two represent different approaches to the same goal.
- Enclomiphene: A selective estrogen receptor modulator sometimes combined with kisspeptin in axis recovery protocols. Not currently in the Doserly registry as a standalone peptide.
- SS-31: Mentioned in community stacking protocols as part of a mitochondrial/cell-health layer alongside fertility protocols.
- MOTS-C: Included in community fertility support stacks for metabolic optimization.
- Glutathione: Antioxidant support in fertility protocols, particularly for egg and sperm quality.
- NAD+: Cellular energy support included in community conception/fertility optimization stacks.
Not Good With (Caution Advised)
- Continuous GnRH agonists (leuprolide, goserelin): These suppress LH/FSH through receptor downregulation, which would counteract kisspeptin's stimulatory mechanism.
- PT-141 / Melanotan II: While these address libido through melanocortin receptor activation (a completely different pathway), combining them with kisspeptin is rarely discussed and could complicate hormonal monitoring. One community member reported preferring Melanotan over kisspeptin for direct libido effects.
- Aromatase inhibitors (ongoing): While occasionally necessary to manage kisspeptin-induced estradiol elevation, chronic aromatase inhibitor use may suppress the estrogen needed for bone health, cardiovascular protection, and brain function.
Administration Guide
Kisspeptin-10 is most commonly administered via subcutaneous injection. Community reports also describe intranasal administration using commercially available nasal spray formulations, though this route has not been studied in controlled clinical settings and bioavailability is uncharacterized.
Materials typically required:
- Kisspeptin-10 lyophilized vials (commonly available in 10 mg size)
- Bacteriostatic water for reconstitution
- Insulin syringes (U-100; 29-31 gauge recommended)
- Alcohol swabs
- Sharps disposal container
Recommended reconstitution solution: Bacteriostatic water (0.9% benzyl alcohol). Sources commonly recommend adding 3.0 mL to a 10 mg vial, yielding a concentration of approximately 3.33 mg/mL.
Timing considerations: Sources do not report a strong consensus on optimal time of day. Some community members prefer morning administration to align with natural GnRH rhythms. Clinical studies have administered kisspeptin at various times without reported timing-dependent differences in response. For those using intermittent protocols (3x/week), spacing injections at least 48 hours apart is recommended to avoid tachyphylaxis [11][12].
Post-administration monitoring: Track LH, FSH, testosterone (men), estradiol (both sexes), and prolactin at baseline and periodically during use. Monitor for injection site reactions (redness, itching), flushing, headache, and signs of estradiol elevation (sleep disturbance, mood changes, fluid retention) with prolonged use.
Supplies & Planning
The following general supplies are typically associated with kisspeptin-10 research protocols:
- Peptide vials: Kisspeptin-10, commonly available in 10 mg lyophilized vials
- Reconstitution solution: Bacteriostatic water (10 mL bottles)
- Syringes: U-100 insulin syringes (29-31 gauge, 1 mL). For very small-volume injections (under 10 units), 30-unit or 50-unit insulin syringes provide improved measurement accuracy
- Alcohol swabs: For vial stopper and injection site preparation
- Sharps container: For safe disposal of used syringes
- Storage: Freezer space for lyophilized vials; refrigerator space for reconstituted vials
Specific quantities depend on the chosen protocol (dose, frequency, cycle length) and should be discussed with a healthcare provider. Doserly's reconstitution calculator can help determine bacteriostatic water volumes and doses per vial based on your specific parameters.
Storage & Handling
Lyophilized (powder) form:
- Long-term storage: -20°C (-4°F) or below, in a dry, dark environment with desiccant if available
- Short-term storage: 2-8°C (35.6-46.4°F) for weeks to months
- Allow vials to reach room temperature before opening to prevent condensation
Reconstituted (liquid) form:
- Refrigerate immediately at 2-8°C (35.6-46.4°F), protected from light
- Use within approximately 4 weeks (28 days) when reconstituted with bacteriostatic water
- Do not freeze reconstituted solutions
- Avoid repeated freeze-thaw cycles, which degrade peptide integrity
- Discard bacteriostatic water 28 days after opening
Handling best practices:
- Inspect reconstituted solution before each use; it should be clear and colorless with no particles or cloudiness
- Gently swirl or roll vials when mixing; never shake vigorously (may cause foaming and degradation)
- Use sterile technique when drawing doses; swab vial stopper with alcohol before each use
- Label vials with reconstitution date
Lifestyle Factors
Several lifestyle factors significantly influence kisspeptin's effectiveness, because the kisspeptin system is inherently sensitive to metabolic and stress signals:
Nutrition: Maintaining adequate caloric intake and a nutrient-dense diet supports kisspeptin neuron activity. Severe caloric restriction suppresses kisspeptin signaling and can negate the peptide's effects. Zinc and healthy fats are particularly relevant for supporting downstream testosterone and estrogen production.
Stress management: Elevated cortisol directly inhibits kisspeptin secretion. Chronic stress can counteract the peptide's goal of restoring pulsatile GnRH release. Stress reduction practices (adequate rest, manageable workload, relaxation techniques) are not optional extras but directly relevant to outcomes.
Sleep: Aim for 7-9 hours of quality sleep. Hormonal signaling, particularly GnRH pulsatility, is closely tied to sleep architecture. Poor sleep can blunt the HPG axis response that kisspeptin is designed to stimulate.
Exercise: Regular physical activity supports metabolic health and healthy hormone levels. However, excessive exercise (particularly endurance training at high volumes) can suppress the HPG axis, similar to caloric restriction. Moderate resistance training is generally considered supportive.
Body composition: Both very low and very high body fat percentages affect kisspeptin neuron activity. Higher body fat increases aromatase activity (converting more testosterone to estradiol), which may explain why some users experience estradiol elevation. Maintaining a healthy body composition supports optimal hormonal response.
Regulatory Status & Research Classification
United States (FDA): Kisspeptin is not FDA-approved for therapeutic use. It is classified as a research compound. Kisspeptin-54 has been used in investigational clinical trials, including studies at Imperial College London and registered trials on ClinicalTrials.gov. No IND (Investigational New Drug) application for commercial development has been publicly announced.
United Kingdom (MHRA): Kisspeptin has been studied extensively at Imperial College London under clinical trial authorizations. The research group led by Professor Waljit Dhillo has conducted multiple funded clinical studies on kisspeptin for reproductive disorders and HSDD. Not approved as a licensed medicine.
Canada (Health Canada): No approved therapeutic indication. Not listed as a Natural Health Product.
Australia (TGA): No specific scheduling or approval. Classified as a research substance.
European Union (EMA): No marketing authorization. Research use only.
WADA Status: Not specifically listed on the WADA Prohibited List as of current publications. However, athletes should exercise caution as kisspeptin's gonadotropin-stimulating effects could theoretically be classified under the category of substances that affect the HPG axis.
Active clinical trials: Clinical studies have been conducted primarily at Imperial College London, funded by the National Institute for Health and Care Research (NIHR) and the Medical Research Council. Published trials include JAMA Network Open-published studies on HSDD in both men and women [2].
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is kisspeptin-10 and how is it different from kisspeptin-54?
Kisspeptin-10 is the smallest active fragment of the kisspeptin family, consisting of 10 amino acids. Kisspeptin-54 is the full-length form with 54 amino acids. Both activate the same receptor (KISS1R/GPR54) through their shared C-terminal sequence. Kisspeptin-54 has a longer half-life (approximately 28 minutes IV) and has been used in most published clinical trials. Kisspeptin-10, being smaller and cheaper to synthesize, is more commonly available in research peptide markets. The two are not interchangeable in terms of dosing, as kisspeptin-54 is roughly five times the molecular weight [1].
What dosing protocol do sources generally report?
Based on available sources, commonly reported ranges are 100-200 mcg per day for subcutaneous kisspeptin-10. However, evidence-based sources note that intermittent dosing (2-3 times per week with at least 48 hours between doses) may better preserve receptor sensitivity and avoid tachyphylaxis compared to daily protocols [11][12]. Protocols should be discussed with a qualified healthcare provider.
Can kisspeptin increase testosterone?
Clinical studies demonstrate that kisspeptin stimulates the HPG axis cascade: kisspeptin triggers GnRH release, which stimulates LH and FSH, which in turn stimulate testosterone production. Published human studies show measurable testosterone elevation following kisspeptin administration [13][14]. The magnitude of the increase depends on dose, duration, baseline hormonal status, and individual physiology.
Does kisspeptin cause tachyphylaxis?
Based on available clinical data, continuous or twice-daily kisspeptin administration can lead to receptor desensitization (tachyphylaxis) within approximately two weeks. The Jayasena 2009 study documented progressive decline in gonadotropin responses over 14 days of twice-daily subcutaneous kisspeptin-54 [11]. Intermittent dosing with washout periods is the most commonly recommended approach to mitigate this risk.
Is intranasal kisspeptin effective?
Community reports describe successful use of kisspeptin-10 via intranasal spray, with one detailed account reporting significant improvement in sexual function and libido over several weeks. However, no published clinical data exists on intranasal kisspeptin bioavailability or efficacy. This route remains uncharacterized in the scientific literature.
What blood work should be monitored?
Sources consistently recommend monitoring LH, FSH, total testosterone, free testosterone, estradiol, prolactin, and SHBG at baseline and periodically during use. For women, estradiol, progesterone (mid-luteal), AMH, and thyroid panel are recommended. Estradiol monitoring is particularly important for men on longer protocols, as elevated estradiol has been reported with prolonged daily use.
Sources & References
[1] Tsoutsouki J, Abbara A, Dhillo W (2022). "The Role of Kisspeptin in the Control of the Hypothalamic-Pituitary-Gonadal Axis and Reproduction." Endocrine Reviews. https://academic.oup.com/edrv
[2] Mills EG, Sheridan A, Sheridan R, et al. (2023). "Kisspeptin Administration Improves Sexual Brain Processing in Women and Men with Hypoactive Sexual Desire Disorder." JAMA Network Open.
[3] Lee JH, Miele ME, Hicks DJ, et al. (1996). "KiSS-1, a novel human malignant melanoma metastasis-suppressor gene." Journal of the National Cancer Institute, 88(23), 1731-1737.
[4] Seminara SB, Messager S, Chatzidaki EE, et al. (2003). "The GPR54 gene as a regulator of puberty." New England Journal of Medicine, 349(17), 1614-1627. https://pubmed.ncbi.nlm.nih.gov/14573733/
[5] Teles MG, Bianco SDC, Brito VN, et al. (2008). "A GPR54-Activating Mutation in a Patient with Central Precocious Puberty." New England Journal of Medicine, 358(7), 709-715.
[6] Comninos AN, Wall MB, Demetriou L, et al. (2017). "Kisspeptin modulates sexual and emotional brain processing in humans." Journal of Clinical Investigation, 127(2), 709-719. https://doi.org/10.1172/JCI89519
[7] Xie Q, Kang Y, Zhang C, et al. (2022). "Metabolic regulation of kisspeptin - the link between energy balance and reproduction."
[8] Dhillo WS, et al. "GnRH-dependent action of kisspeptin confirmed through antagonist studies." Endocrine Reviews (Oxford Academic).
[9] Navarro VM (2020). "Kisspeptin and Glucose Homeostasis." Nature Reviews Endocrinology, 16(8), 407-420.
[10] Harter CJL, Kavanagh GS, Smith JT (2018). "The role of kisspeptin neurons in reproduction and metabolism." The Journal of Endocrinology, 238(3), R173-R183. https://doi.org/10.1530/JOE-18-0108
[11] Jayasena CN, et al. (2009). "Subcutaneous kisspeptin-54 administration in women with hypothalamic amenorrhea: tachyphylaxis with twice-daily dosing." Clinical studies referenced in Endocrine Reviews.
[12] Izzi-Engbeaya C, Hill TG, Bowe JE (2019). Additional kisspeptin research on glucose homeostasis.
[13] Dhillo WS, Chaudhri OB, Patterson M, et al. (2005). "Kisspeptin-54 stimulates the hypothalamic-pituitary gonadal axis in human males." Journal of Clinical Endocrinology & Metabolism, 90(12), 6609-6615. https://doi.org/10.1210/jc.2005-1468
[14] George JT, Veldhuis JD, Roseweir AK, et al. (2011). "Kisspeptin-10 is a potent stimulator of LH and increases pulse frequency in men." Journal of Clinical Endocrinology & Metabolism, 96(8), E1228-1236. https://doi.org/10.1210/jc.2011-0089
[15] Jayasena CN, et al. "Restoration of GnRH pulsatility in functional hypothalamic amenorrhea." Endocrine Reviews.
[16] Abbara A, et al. (2015). "Kisspeptin-54 triggers egg maturation in IVF with reduced OHSS risk." Journal of Clinical Investigation.
[17] Bhattacharya M, Babwah AV (2015). "Kisspeptin: Beyond the Brain." Endocrinology, 156(4), 1218-1227. https://doi.org/10.1210/en.2014-1915
[18] Ly T, Harihar S, Welch DR (2020). "KISS1 in metastatic cancer research and treatment: potential and paradoxes." Cancer Metastasis Reviews. https://doi.org/10.1007/s10555-020-09868-9
[19] Mead EJ, Maguire JJ, Kuc RE, Davenport AP (2007). "Kisspeptins: a multifunctional peptide system with a role in reproduction, cancer and the cardiovascular system." British Journal of Pharmacology, 151(8), 1143-1153.
[20] Gibula-Tarlowska E, Kotlinska JH (2020). "Kissorphin improves spatial memory and cognitive flexibility impairment induced by ethanol treatment in the Barnes maze task in rats." Behavioural Pharmacology, 31(2&3), 272-282. https://doi.org/10.1097/FBP.0000000000000557
[21] Pazarci P, et al. (2020). "The effects of daylight exposure on melatonin levels, Kiss1 expression, and melanoma formation in mice." Croatian Medical Journal, 61(1), 55-61.
Related Peptide Guides
- Gonadorelin - Synthetic GnRH; acts one step downstream from kisspeptin in the HPG axis
- HCG - Human chorionic gonadotropin; mimics LH for direct gonadal stimulation
- PT-141 - Melanocortin-based sexual function peptide; different mechanism from kisspeptin
- Melanotan II - Melanocortin receptor agonist with reported sexual function effects
- Oxytocin - Reproductive and bonding neuropeptide
- Ipamorelin - Growth hormone secretagogue; sometimes combined in broader protocols
- SS-31 - Mitochondrial peptide; mentioned in fertility optimization stacks
- MOTS-C - Mitochondrial peptide; included in community fertility protocols
- Glutathione - Antioxidant; used in fertility support protocols
- NAD+ - Cellular energy support; paired in community conception stacks
Need the reconstitution math for Kisspeptin: Complete Research Guide?
Open the calculator with Kisspeptin: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.