Glutathione: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- GSH, L-Glutathione, Gamma-L-Glutamyl-L-Cysteinyl-Glycine, Master Antioxidant, Reduced Glutathione
Attribute
Administration
- Detail
- Injectable (subcutaneous, intramuscular, intravenous), Oral (standard, liposomal), Intranasal
Attribute
Research Status
- Detail
- Dietary supplement (not FDA-approved for specific therapeutic indications). Decades of clinical use for acetaminophen overdose (as NAC precursor). IV use studied in oncology and neurology.
Attribute
Typical Dose Range
- Detail
- Oral: 250-1000 mg/day; Liposomal: 500-1000 mg/day; Subcutaneous: 100-200 mg/day; IM: 200-600 mg per injection; IV: 600-1400 mg per session
Attribute
Half-Life
- Detail
- Short plasma half-life (minutes); biological activity window varies by route
Attribute
Cycle Length
- Detail
- Oral/liposomal: continuous daily use; Injectable: 4-8 weeks on, 2-4 weeks off
Attribute
Storage
- Detail
- Lyophilized: -20°C; Reconstituted: 2-8°C, use within 2-3 weeks
Overview / What Is Glutathione?
The Basics
Glutathione is a small molecule that every cell in your body produces naturally. Made from just three amino acids (glutamate, cysteine, and glycine), it works as your body's primary internal defense system. If your cells were a house, glutathione would be the combined security system, cleaning crew, and maintenance team all rolled into one.
It handles three critical jobs. First, it neutralizes the damaging byproducts that cells generate during normal energy production, preventing those byproducts from wrecking your DNA and cell membranes. Second, it tags toxins, heavy metals, and drug metabolites so your liver can package them up and flush them out. Third, and perhaps most importantly, it determines whether your immune cells can actually activate and multiply when your body detects a threat [1][2].
What makes glutathione different from most supplements is that you are not introducing something foreign. You are replenishing a molecule your body already produces, one that declines 30-50% by age 60 [1]. That decline tracks with slower recovery, weakened immunity, and increased vulnerability to everything from infections to chronic disease.
The challenge is getting it where it needs to go. Oral glutathione was long considered useless because digestive enzymes break it apart before absorption. More recent research, including a well-controlled six-month trial, has changed that picture [9]. Liposomal formulations, precursor strategies (GlyNAC), and injectable delivery routes each offer different tradeoffs between convenience, speed, and evidence quality.
The Science
Glutathione (gamma-L-glutamyl-L-cysteinyl-glycine, GSH) is the most abundant intracellular thiol, present in virtually all mammalian cells at concentrations of 1-10 mM [1]. It functions as the primary non-enzymatic antioxidant defense, the principal substrate for Phase II detoxification conjugation reactions, and a critical regulator of immune cell metabolic reprogramming [1][2][4].
The molecule exists in two interconvertible forms: the reduced, active thiol form (GSH) and the oxidized disulfide form (GSSG). The GSH:GSSG ratio serves as a real-time indicator of cellular redox status, with healthy cells maintaining ratios above 100:1 [1][3]. Glutathione reductase catalyzes GSSG reduction back to GSH using NADPH as the electron donor, creating a continuous recycling system rather than a consumable buffer [1].
Synthesis occurs through a two-step ATP-dependent process: gamma-glutamylcysteine ligase (GCL, the rate-limiting enzyme) conjugates glutamate and cysteine, followed by glutathione synthetase adding glycine [1]. Cysteine availability is typically rate-limiting for synthesis, which is the mechanistic basis for N-acetylcysteine (NAC) supplementation as a glutathione-boosting strategy [12].
Tissue glutathione levels decline 30-50% with aging, driven by both increased oxidative consumption and impaired recycling capacity secondary to NAD+ depletion [1][8]. This decline is most pronounced in the liver, skeletal muscle, and brain, the most metabolically active tissues [1].
Molecular Identity
Attribute
Common Names
- Detail
- Glutathione, GSH, L-Glutathione, Reduced Glutathione
Attribute
Amino Acid Sequence
- Detail
- gamma-Glu-Cys-Gly (gamma-glutamylcysteinylglycine)
Attribute
Molecular Formula
- Detail
- C₁₀H₁₇N₃O₆S
Attribute
Molecular Weight
- Detail
- 307.32 g/mol
Attribute
CAS Number
- Detail
- 70-18-8
Attribute
PubChem CID
- Detail
- 124886
Attribute
Structural Type
- Detail
- Linear tripeptide with gamma-peptide bond (non-standard linkage between glutamate and cysteine)
Attribute
Active Group
- Detail
- Cysteine thiol (-SH) group (electron donor for antioxidant function)
Attribute
Biosynthesis
- Detail
- Nonribosomal; enzymatic two-step synthesis by GCL and GSS
Attribute
Highest Concentration
- Detail
- Liver (up to 10 mM)
Mechanism of Action
The Basics
Glutathione does three things, and understanding each one explains why it matters across so many different health contexts.
The first job is damage control. Every time your cells produce energy, they generate waste products called reactive oxygen species (ROS). Think of these like sparks flying off a grinding wheel. A few sparks are harmless, even useful as signals. But too many sparks, and things start catching fire: DNA gets damaged, cell membranes develop holes, and proteins stop working properly. Glutathione acts as the fire extinguisher, donating electrons to neutralize these sparks before they cause structural damage [1].
The second job is cleanup. Your liver processes everything from alcohol and medications to environmental pollutants. Glutathione physically attaches itself to these substances, essentially putting a shipping label on them that says "export this." The tagged substances get pumped out of cells and eliminated through bile or urine [1].
The third job is the one most sources overlook: immune gating. Research published in Immunity in 2017 demonstrated that T cells (a critical type of immune cell) without glutathione could detect threats normally but could not multiply in response [2]. Glutathione is not just helpful for immunity; it is a prerequisite for immune cells to mount a full response.
The Science
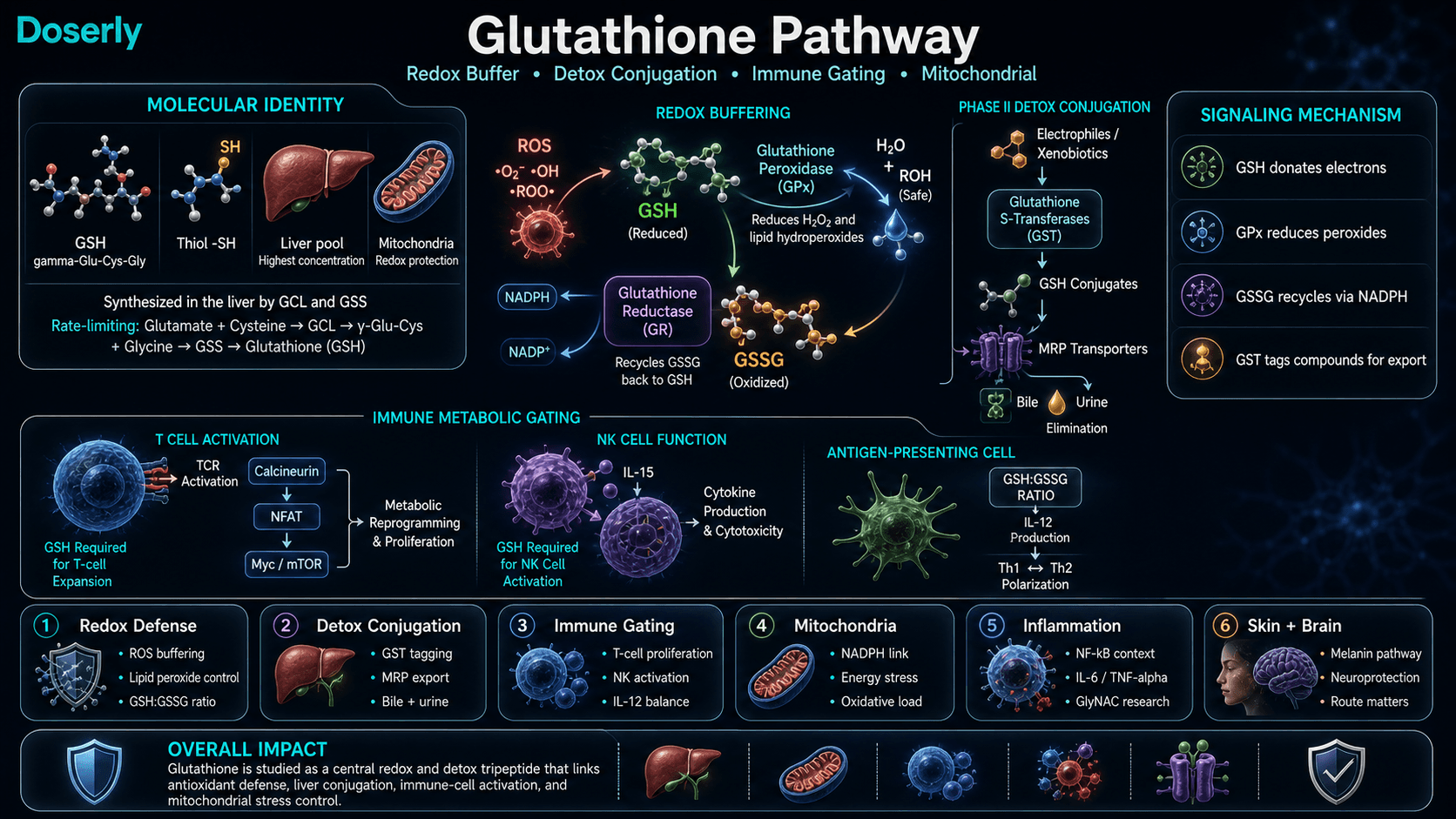
GSH functions through multiple biochemically distinct pathways [1][2][4]:
Redox buffering: GSH donates electrons via its cysteine thiol group to neutralize reactive oxygen and nitrogen species. Glutathione peroxidase (GPx) catalyzes the reduction of hydrogen peroxide and lipid hydroperoxides using GSH as the electron donor. The resulting GSSG is recycled back to GSH by glutathione reductase in an NADPH-dependent reaction [1].
Phase II conjugation: Glutathione S-transferases (GSTs) catalyze the conjugation of GSH to electrophilic substrates, including xenobiotics, drug metabolites, and endogenous reactive intermediates. The resulting GSH conjugates are exported via MRP transporters and processed to mercapturic acids for renal excretion [1].
Immune metabolic gating: The Mak laboratory (2017) demonstrated via Gclc conditional knockout in murine T cells that glutathione is required for the metabolic reprogramming (oxidative phosphorylation to aerobic glycolysis switch) that enables T-cell proliferation following TCR activation. The mechanism involves glutathione maintaining ROS within a permissive signaling window for the calcineurin-NFAT-Myc-mTOR cascade [2][4].
NK cell function: Gclc-deficient NK cells show impaired IL-15-driven metabolic activation, defective cytokine production, and inability to control viral and tumor spread in experimental models [6].
Th1/Th2 polarization: The GSH:GSSG ratio in antigen-presenting cells (macrophages, dendritic cells) controls IL-12 production, which directs downstream T-cell responses toward Th1 (cell-mediated, antiviral) rather than Th2 (antibody-mediated) immunity [7].
Pathway Visualization Image
Pharmacokinetics
The Basics
Understanding how glutathione moves through your body explains why delivery route matters so much for this compound.
When you take glutathione by mouth, digestive enzymes break most of it apart before it reaches your bloodstream. It is not that oral glutathione does nothing; a well-controlled six-month trial showed it does raise blood levels [9]. It just takes longer (1-3 months for measurable changes) and works less efficiently than other routes.
Liposomal formulations wrap glutathione in tiny fat-based capsules that protect it during digestion. A pilot study showed liposomal delivery produced measurable changes within 2 weeks compared to months for standard oral [10]. The evidence is promising but still early stage.
Injectable glutathione (subcutaneous, intramuscular, or intravenous) bypasses digestion entirely and delivers 100% of the dose to the bloodstream. The tradeoff is a short plasma half-life: once in the blood, glutathione is rapidly taken up by cells or broken down. This means injectable glutathione works fast but clears quickly [1].
Precursor strategies like NAC and GlyNAC take a different approach entirely. Instead of delivering finished glutathione, they supply the raw materials so your cells can build their own. This bypasses the absorption problem because the individual amino acids absorb well, and it leverages your body's existing manufacturing capacity [12].
The Science
Glutathione pharmacokinetics are route-dependent and complicated by the distinction between plasma levels, intracellular concentrations, and tissue-specific pools (particularly the mitochondrial glutathione pool, which is maintained independently) [1].
Oral bioavailability: Historically considered negligible due to GGT-mediated hydrolysis in the intestinal lumen and brush border. The Richie 2015 RCT (n=54, 6 months) challenged this, demonstrating dose-dependent increases: 1000 mg/day produced 30-35% GSH increases in erythrocytes, plasma, and lymphocytes, with 260% increase in buccal cells [9]. Whether these peripheral compartment increases reflect deep tissue repletion (liver, brain, mitochondria) remains unresolved.
Liposomal delivery: Phospholipid vesicle encapsulation protects against enzymatic hydrolysis. The Sinha 2018 pilot (n=12, 4 weeks) showed approximately 100% PBMC GSH increase and NK cytotoxicity increases up to 400% within 2 weeks at 500-1000 mg/day. Onset was substantially faster than oral administration [10]. Replication in larger, blinded trials is needed.
Parenteral routes (IV/IM/SC): Achieve 100% systemic bioavailability. Plasma half-life is short (minutes) due to rapid cellular uptake via gamma-glutamyl transferase-mediated transport and direct thiol exchange mechanisms. IV glutathione has been studied at 1.5-3 g/m2 for cisplatin chemoprotection and 1400 mg IV 3x/week in Parkinson's pilots [1].
Precursor pharmacokinetics: NAC (cysteine donor) has well-established oral bioavailability (6-10%) with a half-life of 4-6 hours. Glycine absorbs efficiently with a long half-life. The Kumar 2022 GlyNAC RCT (24 weeks, Baylor College of Medicine) demonstrated that combined glycine and NAC corrected glutathione deficiency in older adults with improvements in oxidative stress, mitochondrial function, and inflammation markers [12].
Research & Clinical Evidence
Glutathione and Immune Function
The Basics
The immune system connection is where glutathione research has produced some of its most striking findings. Your immune cells need glutathione not just as general protection, but as a specific biochemical requirement for multiplication. Without adequate glutathione, immune cells can detect a threat but cannot mount a full-scale response to fight it [2].
Natural killer (NK) cells, which are your body's first-line defense against viruses and abnormal cells, show a direct relationship with glutathione status. In a controlled trial, high-dose oral glutathione more than doubled NK cell killing capacity over three months [9]. A liposomal glutathione pilot study reported even more dramatic increases within two weeks, though these results await confirmation in larger trials [10].
The Science
The immunological evidence rests on three mechanistic pillars:
T-cell metabolic gating: Conditional Gclc knockout in murine T cells demonstrated that GSH is required for the metabolic switch from oxidative phosphorylation to aerobic glycolysis that enables clonal expansion following TCR activation. GSH-deficient T cells retained antigen recognition capability but failed to proliferate [2][4].
NK cell effector function: Gclc-deficient NK cells showed impaired IL-15-driven metabolic reprogramming, defective IFN-gamma and TNF-alpha production, and failure to control MCMV infection and B16 melanoma in murine models [6].
APC polarization: Peterson et al. (1998) demonstrated in PNAS that the intracellular GSH:GSSG ratio in macrophages and dendritic cells determines IL-12 production, which controls Th1/Th2 polarization. Low GSH shifts immune responses toward Th2 dominance [7].
Clinical correlations: COVID-19 severity analysis revealed that all major risk factors (age, diabetes, hypertension, obesity, CVD) share baseline glutathione depletion. A 2022 Frontiers in Microbiology review synthesized evidence linking GSH deficiency to cytokine storm amplification and lymphopenia in severe cases, though causality remains unestablished [14][15].
Glutathione and Liver Health
The Basics
The liver is glutathione's home base, containing the highest concentrations of any organ in the body. This makes sense: the liver is where your body processes medications, alcohol, environmental chemicals, and metabolic waste. Glutathione is the molecule that makes this processing possible, physically attaching to toxins so the liver can package and eliminate them [1].
When liver glutathione runs low, the organ's ability to clear toxins slows down. This is why NAC (a glutathione precursor) is the standard emergency treatment for acetaminophen (paracetamol) overdose: it rapidly restores the liver glutathione that the drug's toxic metabolite has depleted [12].
The Science
GSH is critical for hepatic Phase II conjugation, the primary pathway for xenobiotic and drug metabolite clearance. Glutathione S-transferases catalyze GSH conjugation to electrophilic metabolites, including the reactive acetaminophen metabolite NAPQI [1]. NAC-mediated GSH restoration is the established standard of care for acetaminophen hepatotoxicity.
Open-label pilot studies have demonstrated improvements in ALT, AST, and bilirubin in NAFLD patients receiving glutathione supplementation, though large-scale RCTs are lacking [1]. The hepatoprotective mechanism involves both direct antioxidant protection of hepatocytes and maintenance of Phase II conjugation capacity under toxic load.
Glutathione and Skin Effects
The Basics
Glutathione's influence on skin lightening generates significant public interest, particularly for its potential effects on skin tone and complexion. The mechanism involves glutathione's interaction with the melanin synthesis pathway, where it can shift production toward lighter pigments. Some small trials have reported measurable skin lightening effects, but the evidence base is limited by small sample sizes, short durations, and inconsistent methodology. This is not the primary clinical application of glutathione [9].
The Science
GSH influences melanogenesis by inhibiting tyrosinase activity and shifting melanin synthesis from eumelanin (darker pigments) toward pheomelanin (lighter pigments). A systematic review identified several small trials reporting skin lightening effects with both oral and topical glutathione, but methodological limitations (small n, short duration, lack of blinding) preclude definitive conclusions [9]. Regulatory advisories in some jurisdictions caution against parenteral glutathione for skin lightening due to safety concerns and unproven efficacy.
Glutathione and Aging / Longevity
The Basics
The age-related decline in glutathione levels is one of the most consistent findings in aging research. By age 60, tissue levels can drop 30-50% below young adult values [1]. This decline is not simply because the body "uses up" glutathione faster with age. The recycling machinery itself deteriorates, partly because NAD+, which powers glutathione recycling, also declines with age. This creates a compounding problem: less NAD+ means less recycling, which means lower glutathione, which means more oxidative damage, which further depletes both [8].
The GlyNAC (glycine + NAC) trial at Baylor College of Medicine demonstrated that supplementing both precursors corrected glutathione deficiency in older adults and improved markers of oxidative stress, mitochondrial function, and inflammation over 24 weeks [12].
The Science
The age-related GSH decline involves a compounding "redox trap" mechanism. Increased mitochondrial ROS production with age accelerates GSH oxidation to GSSG. GSSG recycling requires NADPH, which is generated through pathways dependent on NAD+ (pentose phosphate pathway via G6PD, mitochondrial IDH2). NAD+ itself declines approximately 50% by middle age, bottlenecking NADPH generation and consequently GSH recycling [1][8][11].
The Kumar 2022 GlyNAC RCT (randomized, double-blind, 24 weeks, Baylor College of Medicine) demonstrated that supplementation with glycine (1.33 mmol/kg/day) and NAC (0.81 mmol/kg/day) in older adults corrected GSH deficiency, reduced oxidative stress markers, improved mitochondrial fatty acid oxidation, decreased inflammation (IL-6, TNF-alpha), and improved multiple functional measures [12].
Biomarker Evidence Matrix
The Biomarker Evidence Matrix scores each health category on two dimensions: Evidence Strength (quality of published research) and Reported Effectiveness (community-reported outcomes from the sentiment analysis). Categories are only scored when sufficient data exists.
Category
Immune Function
- Evidence Strength
- 8/10
- Reported Effectiveness
- 7/10
- Summary
- Strong mechanistic evidence (Gclc knockout studies, NK cell RCTs showing 2-4x killing capacity increase). Community consistently reports immune support.
Category
Energy Levels
- Evidence Strength
- 4/10
- Reported Effectiveness
- 6/10
- Summary
- Limited direct evidence for energy; GlyNAC trial showed mitochondrial function improvements. Community reports moderate energy benefits.
Category
Skin Health
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Several small trials on skin lightening with mixed methodology. High community interest but limited rigorous evidence.
Category
Recovery & Healing
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Mechanistic support through antioxidant protection during exercise and tissue repair. Community reports smoother recovery.
Category
Focus & Mental Clarity
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- GlyNAC mouse study showed cognitive improvements. Intranasal delivery raises brain GSH on MRS. Limited human cognitive outcome data.
Category
Longevity & Neuroprotection
- Evidence Strength
- 6/10
- Reported Effectiveness
- 6/10
- Summary
- GlyNAC RCT showed aging hallmark improvements. Strong mechanistic rationale for neuroprotection. r/longevity community actively discusses.
Category
Inflammation
- Evidence Strength
- 7/10
- Reported Effectiveness
- 6/10
- Summary
- GlyNAC trial demonstrated inflammatory marker reduction. GSH's role in NF-kB modulation well-characterized. Limited direct community reports.
Category
Mood & Wellbeing
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Minimal direct evidence. A few community reports of mild mood boost. NAC associated with mood side effects in some users.
Category
Side Effect Burden
- Evidence Strength
- 8/10
- Reported Effectiveness
- 7/10
- Summary
- Well-documented safety profile across routes. Detox reactions at high initial doses are the main concern. Generally well tolerated.
Category
Nausea & GI Tolerance
- Evidence Strength
- 6/10
- Reported Effectiveness
- 5/10
- Summary
- Oral forms can cause GI discomfort. NAC causes nausea/heartburn in some. Injectable routes avoid GI issues. Route-dependent.
Category
Stress Tolerance
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- Indirect mechanistic support through cortisol/oxidative stress pathways. Minimal community reports.
Category
Daily Functioning
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- GlyNAC trial measured functional improvements in older adults. Very few direct community reports.
Categories not scored (insufficient data): Fat Loss, Muscle Growth, Weight Management, Appetite & Satiety, Food Noise, Sleep Quality, Memory & Cognition, Anxiety, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Joint Health, Pain Management, Physical Performance, Gut Health, Digestive Comfort, Hair Health, Heart Health, Blood Pressure, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Fluid Retention, Body Image, Bone Health, Cravings & Impulse Control, Social Connection, Treatment Adherence, Withdrawal Symptoms
Benefits & Potential Effects
The Basics
Glutathione's benefits span several systems, reflecting its fundamental role in cellular health rather than a targeted therapeutic effect. The strongest evidence supports immune function enhancement, liver protection, and antioxidant defense. Other reported benefits, including skin effects and cognitive improvements, have supporting research but with less rigorous evidence.
The key benefits most consistently supported by available research include:
- Immune system support. Glutathione directly determines whether immune cells can activate and multiply. NK cell killing capacity more than doubled in a controlled trial of high-dose oral glutathione over three months [9]. This is not a subtle effect; it is a fundamental requirement for immune function [2].
- Liver protection and detoxification. As the primary molecule enabling Phase II liver detoxification, maintaining glutathione status supports the liver's ability to process medications, environmental toxins, and metabolic waste [1]. This is why NAC (which restores glutathione) is the standard treatment for acetaminophen poisoning.
- Antioxidant protection. Glutathione neutralizes the damaging byproducts of normal cell metabolism, protecting DNA, cell membranes, and proteins from oxidative damage. It also regenerates other antioxidants, including vitamins C and E, in their active forms [1].
- Mitochondrial health. Mitochondria maintain their own dedicated glutathione pool because they generate the most oxidative stress during energy production. Declining mitochondrial glutathione is linked to reduced energy production and accelerated aging [1][12].
- Skin quality. Some small trials have reported skin lightening effects and improvements in skin tone, though the evidence is limited and inconsistent [9].
The Science
The evidence hierarchy for glutathione benefits spans from robust mechanistic data and controlled human trials (immune function, hepatoprotection) to preliminary clinical signals (skin effects, cognitive markers) [1][2][9][12]:
Immune function (strong evidence): The Richie 2015 RCT demonstrated >2x NK cytotoxicity increase with 1000 mg/day oral GSH at 3 months (n=54) [9]. Liposomal GSH pilot showed up to 400% NK killing increase at 2 weeks (n=12, unblinded) [10]. Gclc knockout studies provide mechanistic causality for the GSH-immune link [2][6].
Hepatoprotection (strong evidence): GSH conjugation is essential for Phase II detoxification. NAC-mediated GSH restoration is established standard of care for NAPQI hepatotoxicity. Open-label pilots show ALT/AST improvement in NAFLD [1].
Antioxidant defense (strong evidence): GSH/GPx system is the primary intracellular defense against ROS. Extensive in vitro, animal, and human biomarker data. GlyNAC trial demonstrated oxidative stress marker correction [1][12].
Longevity markers (moderate evidence): GlyNAC RCT showed improvement in multiple aging hallmarks over 24 weeks in older adults [12]. Mouse lifespan extension with GlyNAC [12]. Correlational data linking GSH status to aging outcomes.
Skin (limited evidence): Systematic review identifies several small trials with methodological limitations. Tyrosinase inhibition and melanin shifting mechanism is established, but clinical translation is weak [9].
Reading about potential benefits is the starting point. Knowing whether you're actually experiencing them is where real value begins. Doserly lets you track the specific health markers that matter for your protocol, from body composition and energy levels to sleep quality, mood, and recovery time, building a personal dataset that goes beyond subjective impressions.
The app's proactive monitoring doesn't wait for you to notice a problem. It surfaces patterns in your logged data that might suggest suboptimal timing, flags potential interactions with other items in your health stack, and helps you identify which benefits are tracking with what the research suggests and which aren't materializing. Think of it as a second set of eyes on your protocol, always watching the trends.
Connect protocol changes to labs and health markers.
Doserly can keep lab results, biomarkers, symptoms, and dose history close together so follow-up conversations have better context.
Insights
Labs and trends

Doserly organizes data; it does not diagnose or interpret labs for you.
Side Effects & Safety Considerations
The Basics
Glutathione has a strong overall safety profile, which makes sense given that it is a molecule your body already produces naturally. At standard supplemental doses (500-1000 mg/day oral or liposomal), the most common complaint is mild GI discomfort with oral forms [9][10].
The one experience that catches many people off guard is the "detox reaction" when starting too high. When glutathione mobilizes stored toxins faster than your liver and kidneys can eliminate them, you can experience flu-like symptoms: headaches, body aches, fatigue, brain fog, nausea, and chills. This is not a true allergic reaction or a sign that glutathione is harmful. It is a sign that the dose exceeded your body's clearance capacity. The solution is straightforward: start with a lower dose and increase gradually over several weeks [community data].
For injectable forms, mild injection site reactions (redness, itching) are occasionally reported. Some users note a burning sensation with subcutaneous glutathione, which may be related to the solution's pH. Buffering with sodium bicarbonate solution is discussed in some community protocols [community data].
NAC, the most commonly used glutathione precursor, can cause nausea and heartburn at higher doses. Some individuals report mood changes (irritability) with NAC, though this is uncommon [community data].
The Science
Safety data from controlled trials: The Richie 2015 RCT (1000 mg/day oral, 6 months) reported no serious adverse events [9]. The Kumar 2022 GlyNAC trial (24 weeks) similarly showed favorable tolerability [12]. Animal studies with repeated IM glutathione (approximately 124 mg/kg twice weekly) showed no organ toxicity on histological or biochemical assessment.
Herxheimer-like detox reactions: Reported primarily in community and clinical practice settings when initiating glutathione at doses exceeding the individual's elimination capacity. The mechanism involves mobilization of stored xenobiotics and heavy metal conjugates triggering cytokine release (TNF-alpha, IL-6, IL-8), producing flu-like symptoms. Management is dose reduction and gradual titration [community data].
Parenteral safety considerations: National drug regulatory advisories in some jurisdictions caution against parenteral (IV/IM) glutathione for skin lightening due to safety concerns including rare infusion reactions (fever, rigors, hypotension reported with contaminated lots) and insufficient efficacy evidence for this indication.
Drug interactions: Theoretical interaction with platinum chemotherapy protocols (glutathione is studied as a chemoprotective adjunct but may affect drug efficacy). Concomitant high-dose antioxidant regimens may confound oxidative stress monitoring endpoints. Acetaldehyde (from alcohol metabolism) directly binds and depletes glutathione, reducing its effectiveness. A minimum 12-hour wait after alcohol consumption before glutathione administration is recommended in community protocols [community data].
The side effects and contraindications above give you a map of what to watch for. Doserly turns that map into a daily practice. Log the specific biomarkers and symptoms associated with this compound's known risk profile, and the app builds a timeline of how your body is responding across your cycle.
Trending in the wrong direction on a key marker? Noticing a pattern that started two weeks into your protocol? Doserly connects the dots between your protocol timeline and your logged data, making it easier to spot emerging issues early and have informed, data-backed conversations with your healthcare provider about what's working and what needs attention.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
Dosing Protocols
The Basics
Glutathione dosing depends heavily on the delivery route you choose, and the ranges reported across sources vary more than for most compounds in this guide series. This variation reflects the genuine uncertainty: there are no large-scale, standardized dosing trials for supplemental glutathione outside of specific medical uses like acetaminophen overdose.
For oral supplementation, commonly cited ranges fall between 250 and 1000 mg per day. The six-month controlled trial used 250 mg and 1000 mg daily groups, with the higher dose showing stronger effects [9]. Liposomal oral forms are typically reported at 500-1000 mg per day [10].
For the precursor approach (GlyNAC), the Baylor College of Medicine trial used weight-based dosing: glycine at 1.33 mmol/kg/day and NAC at 0.81 mmol/kg/day, which translates to substantial daily amounts of both amino acids [12].
For injectable protocols, subcutaneous doses reported in the community range from 50 to 400 mg per injection, with frequency varying from daily to 2-3 times weekly. A conservative starting approach reported in community sources begins at 50 mg three times per week and gradually increases over six weeks, which helps avoid the detox reactions described in the Side Effects section. Intramuscular protocols typically cite 300-600 mg per injection, 1-2 times weekly.
The most important principle across all routes and doses is to start conservatively and increase gradually, allowing the body's elimination pathways to keep pace with the mobilized toxins.
The Science
Oral (RCT-supported): 250-1000 mg/day. The Richie 2015 RCT demonstrated dose-dependent responses at 250 mg and 1000 mg daily over 6 months. The higher dose produced 30-35% erythrocyte GSH increases and >2x NK cytotoxicity [9].
Liposomal (pilot data): 500-1000 mg/day. Sinha 2018 pilot showed rapid onset (2 weeks) with approximately 100% PBMC GSH increase [10].
GlyNAC (RCT-supported): Glycine 1.33 mmol/kg/day + NAC 0.81 mmol/kg/day for 12-24 weeks. The Kumar 2022 Baylor RCT demonstrated correction of glutathione deficiency, reduced oxidative stress, improved mitochondrial function [12].
IV (clinical use): 1.5-3 g/m2 IV for cisplatin chemoprotection (RCT-supported). 1400 mg IV 3x/week for Parkinson's pilots (limited evidence, mixed results). 600-1200 mg IV for "wellness" protocols (no RCT support).
SC/IM (practice-derived): SC 100-200 mg/day with gradual titration. IM 300-600 mg 1-2x/week (clinical practice extrapolation). These doses are empirical and not validated by randomized controlled trials. Reconstitution: 2.0 mL bacteriostatic water per 600 mg vial yields 300 mg/mL concentration.
What to Expect
The timeline for experiencing effects from glutathione depends significantly on the delivery route and starting glutathione status.
Weeks 1-2: For injectable routes (SC/IM), some users report feeling worse initially if the starting dose is too high, experiencing flu-like symptoms, fatigue, and brain fog. This typically resolves with dose reduction. Starting at a conservative dose, this period should be uneventful. For oral supplementation, no noticeable changes are typically reported in this early window. Liposomal glutathione users may notice subtle energy changes within 2 weeks based on pilot data showing rapid biomarker changes [10].
Weeks 3-4: Users who started low on injectable protocols and have gradually increased may begin noticing improved energy and recovery. Skin clarity improvements sometimes become apparent in this window, particularly with higher-dose protocols. The body's elimination pathways have had time to adapt to the increased detox load.
Weeks 5-8: This is when most oral glutathione users begin to see measurable changes in blood biomarkers. For injectable users, this represents the typical assessment window. Community sources recommend evaluating whether objective benefits (lab values, symptom improvements) justify continuing beyond 8 weeks. If no measurable benefit has emerged by week 8, reassessment of the approach (route, dose, or whether glutathione is the appropriate intervention) is warranted.
Months 3-6: The Richie 2015 RCT showed continued improvement through month 3 (NK cell doubling) and sustained effects through month 6 with oral dosing [9]. The GlyNAC trial showed progressive improvements across multiple markers through 24 weeks [12]. Long-term functional benefits (reduced illness frequency, sustained energy, skin quality maintenance) are reported by community members using glutathione for extended periods.
Ongoing maintenance: Oral and liposomal glutathione do not require cycling per available evidence. Injectable protocols commonly use 4-8 week cycles with 2-4 week breaks, though this cycling pattern is practice-derived rather than evidence-based.
Interaction Compatibility
Synergistic Combinations ("Good With")
- NAD+ — Addresses the glutathione recycling bottleneck. NAD+ powers NADPH generation, which glutathione reductase requires to recycle oxidized glutathione back to its active form. Mechanistically complementary [8][11].
- SS-31 — Targets mitochondrial protection through a different mechanism (cardiolipin stabilization). Combined with glutathione's mitochondrial antioxidant role, these compounds address mitochondrial health from two angles.
- Thymosin Alpha-1 — When TA1 drives T-cell expansion in immune protocols, dividing cells require glutathione to maintain the oxidative balance needed for proliferation. Glutathione supports TA1's immune expansion effects.
- KPV — Glutathione addresses the antioxidant/redox environment while KPV modulates the NF-kB inflammatory pathway. Complementary anti-inflammatory approaches.
- MOTS-C — Mitochondrial-derived peptide that enhances metabolic function. Both compounds support mitochondrial health through different pathways.
- Selank — Paired in immune protocol stacks for cortisol normalization alongside glutathione's antioxidant infrastructure.
- Vitamin C — Glutathione regenerates oxidized vitamin C; vitamin C can help spare glutathione. Synergistic antioxidant recycling.
- Vitamin E — Glutathione (via GPx) reduces lipid hydroperoxides, working alongside vitamin E's lipid-phase antioxidant activity.
- Selenium — Cofactor for glutathione peroxidase (GPx) enzymes. Supports the enzymatic pathway that uses glutathione to neutralize peroxides.
- CoQ10 — Mitochondrial electron transport chain support complements glutathione's mitochondrial antioxidant role.
Cautions ("Use With Care")
- High-dose antioxidant regimens — Combining multiple high-dose antioxidants may confound oxidative stress monitoring and could theoretically interfere with beneficial ROS signaling in exercise adaptation.
- Platinum chemotherapy agents (cisplatin, carboplatin) — While glutathione is studied as a chemoprotective adjunct (reducing neuro/ototoxicity), timing relative to chemotherapy is critical. Concurrent administration could theoretically reduce drug efficacy. Clinical use requires oncologist oversight.
- Alcohol — Acetaldehyde from alcohol metabolism directly binds and depletes glutathione. Wait at least 12 hours after alcohol consumption before glutathione administration.
Administration Guide
Glutathione is available through multiple administration routes, each with different practical requirements.
Injectable (subcutaneous): Requires reconstitution of lyophilized glutathione powder with bacteriostatic water. Common vial sizes include 200 mg and 600 mg. For the 600 mg vial, 2.0 mL of bacteriostatic water produces a 300 mg/mL concentration suitable for insulin syringe measurement. Subcutaneous injections are typically administered in the abdomen, thigh, or upper arm. Some users report a burning sensation with SC glutathione, which may be pH-related.
Injectable (intramuscular): Same reconstitution requirements as subcutaneous. IM injections allow for larger volumes per injection site. Typically administered in the deltoid or gluteal muscles.
Oral (standard): Available as capsules or tablets, typically in 250 mg or 500 mg strengths. Can be taken with or without food. No reconstitution needed.
Oral (liposomal): Available as liquid or softgel formulations with phospholipid encapsulation. Taken orally, often on an empty stomach for optimal absorption.
Precursors (GlyNAC/NAC): Glycine and NAC are available as capsules or powders. The high daily amounts required (particularly for weight-based GlyNAC dosing) may be more practical in powder form. NAC is sometimes better tolerated when taken with food to reduce GI effects.
Timing considerations: No strict timing requirements for most routes. Injectable protocols are often administered at a consistent daily or weekly time. Oral forms may be taken morning or evening based on individual preference. Community sources recommend waiting at least 12 hours after alcohol consumption before any glutathione administration.
Post-administration monitoring: Watch for signs of detox reactions (headache, fatigue, flu-like symptoms) especially in the first 2 weeks of a new protocol. If symptoms occur, the standard recommendation is to reduce the dose rather than stop entirely.
Supplies & Planning
For injectable (SC/IM) protocols:
- Glutathione lyophilized vials (commonly available in 200 mg and 600 mg sizes)
- Bacteriostatic water (10 mL bottles)
- Insulin syringes (U-100, 27-30 gauge for SC; larger gauge may be preferred for IM)
- Alcohol swabs (for vial stoppers and injection sites)
- Sharps disposal container
- Reconstitution syringes and needles (for drawing bacteriostatic water)
For oral protocols:
- Glutathione capsules/tablets (standard or liposomal formulations)
- No additional supplies needed
For GlyNAC precursor protocols:
- Glycine powder or capsules
- NAC capsules (commonly 600 mg)
- Note: weight-based dosing may require substantial daily quantities; powder form is often more practical
Readers should consult their healthcare provider for specific quantities based on their individual protocol. Use the reconstitution calculator for help with injectable preparation math.
Storage & Handling
Lyophilized (powder) glutathione:
- Store at -20°C (-4°F) for long-term preservation
- Protect from light and moisture
- Stable for extended periods when properly stored
Reconstituted glutathione:
- Refrigerate at 2-8°C (35.6-46.4°F) immediately after reconstitution
- Use within 2-3 weeks for optimal potency; glutathione is relatively unstable once reconstituted
- Do not freeze reconstituted solution
- Avoid repeated temperature cycling
- Allow vials to reach room temperature before opening to reduce condensation uptake
- Discard if solution becomes cloudy or discolored
Oral/liposomal glutathione:
- Follow manufacturer's storage instructions (typically room temperature or refrigerated for liposomal)
- Protect from excessive heat and direct sunlight
NAC and glycine (precursors):
- Store at room temperature in a cool, dry place
- NAC is hygroscopic (absorbs moisture); keep containers tightly sealed
Lifestyle Factors
Several lifestyle factors significantly influence glutathione status and can either support or undermine a supplementation protocol.
Diet: Sulfur-rich foods support endogenous glutathione synthesis. Cruciferous vegetables (broccoli, Brussels sprouts, kale, cabbage), garlic, onions, and allium vegetables provide sulfur-containing amino acids that feed into the glutathione synthesis pathway. Adequate protein intake ensures availability of all three precursor amino acids (glutamate, cysteine, glycine) [1].
Alcohol: This deserves special emphasis. Alcohol metabolism directly depletes hepatic glutathione through multiple mechanisms: the production of ROS during ethanol oxidation, direct binding of acetaldehyde to GSH, and competition for the liver's detoxification capacity. If glutathione is administered while the liver is still processing alcohol and acetaldehyde, the glutathione gets consumed by the alcohol cleanup rather than performing its intended antioxidant and detox functions. Community protocols consistently recommend waiting at least 12 hours after the last drink, and longer after heavy consumption [community data].
Sleep: Adequate sleep supports the body's natural antioxidant recycling processes. Sleep deprivation increases oxidative stress and accelerates glutathione depletion [1].
Exercise: Physical activity increases ROS production acutely (which is actually part of how exercise signals adaptation) but chronically improves antioxidant capacity. Moderate exercise supports glutathione status; very high-intensity or prolonged exercise temporarily depletes it.
Stress management: Chronic psychological stress elevates cortisol and systemic inflammation, both of which increase oxidative burden and accelerate glutathione consumption [1].
Complementary nutrients: Vitamin C and selenium support glutathione function. Selenium is a cofactor for glutathione peroxidase enzymes, and vitamin C participates in the antioxidant recycling network with glutathione [1].
Environmental toxin exposure: Reducing exposure to heavy metals, pesticides, air pollution, and other environmental toxins decreases the demand on glutathione's detoxification pathway, allowing more GSH to remain available for antioxidant and immune functions.
Peptide protocols don't exist in a vacuum. Your nutrition, exercise, sleep, stress, and the rest of your health stack all influence outcomes. Doserly tracks your entire health picture in one place: peptides, supplements, medications, TRT/HRT, and the lifestyle factors that determine whether your protocol reaches its potential.
This holistic view reveals correlations that compartmentalized tracking misses. You might discover that your recovery improvements stall during weeks with poor sleep, or that adding a specific supplement amplified a benefit you were already seeing. Doserly's cross-category visibility helps you understand which lifestyle factors are pulling the most weight in your results, turning health optimization from guesswork into a data-informed practice.
Keep sensitive protocol records in a purpose-built app.
Doserly is designed for private health tracking with structured records, offline-ready workflows, and exportable history when you need it.
Privacy
Health records
Privacy controls help you manage records; keep clinical records where required.
Regulatory Status & Research Classification
United States (FDA): Glutathione is marketed as a dietary supplement and is not FDA-approved for any specific therapeutic indication. NAC (the primary precursor) has FDA approval as a prescription drug for acetaminophen overdose and as a mucolytic agent, while also being available as a dietary supplement. IV glutathione has been studied in clinical trials but is not FDA-approved for conditions like Parkinson's disease or skin lightening. GlyNAC is a combination of two dietary supplement amino acids.
Canada (Health Canada): Glutathione is available as a Natural Health Product (NHP). NAC is similarly available as an NHP with recognized monograph for antioxidant support.
United Kingdom (MHRA): Available as a food supplement. Not classified as a licensed medicine. NAC is available both as a licensed medicine (acetaminophen overdose) and as a supplement.
Australia (TGA): Glutathione is available as a listed complementary medicine. Regulatory advisories in some regions caution against injectable glutathione use for skin lightening.
European Union (EMA): No centralized marketing authorization. Available as a food supplement in EU member states. NAC has marketing authorizations in several member states as a mucolytic.
WADA status: Not prohibited. Neither glutathione nor its precursors (NAC, glycine) appear on the WADA prohibited list.
Active clinical trials: Multiple trials registered on ClinicalTrials.gov investigating glutathione and GlyNAC for aging, oxidative stress, immune function, and various clinical conditions.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
Is glutathione safe to take?
Glutathione has a well-documented safety profile at standard supplemental doses. It is a molecule your body already produces naturally in every cell. The most common side effects are mild GI discomfort with oral forms and potential "detox reactions" (flu-like symptoms) when starting injectable protocols at too high a dose. Based on available trial data, no serious adverse events have been reported at doses up to 1000 mg/day oral over 6 months [9][12]. As with any supplement, consulting a healthcare professional before starting is advisable.
What is the difference between glutathione and NAC?
Glutathione is the finished protective molecule. NAC (N-acetylcysteine) is a precursor that provides cysteine, one of the three building blocks cells need to synthesize glutathione. Taking glutathione delivers the end product directly but faces absorption challenges. Taking NAC relies on your body's own synthesis capacity but absorbs well. GlyNAC (glycine + NAC) provides both rate-limiting precursors and has the strongest clinical trial evidence. These are complementary strategies, not mutually exclusive [12].
How long does glutathione take to work?
Based on available research, liposomal glutathione showed measurable immune cell changes within 2 weeks in pilot data [10]. Oral glutathione took 1-3 months to produce measurable blood level changes [9]. GlyNAC showed improvements across multiple markers over 12-24 weeks [12]. Functional effects that are noticeable in daily life likely build over months rather than days.
Can I take glutathione if I drink alcohol?
Based on community protocols and biochemistry, glutathione administration should wait at least 12 hours after the last alcoholic drink. Alcohol metabolism produces acetaldehyde, which directly binds and depletes glutathione. Administering glutathione while the liver is still processing alcohol wastes the glutathione on alcohol cleanup rather than allowing it to perform its intended antioxidant and detox functions.
Does glutathione lighten skin?
Glutathione influences the melanin synthesis pathway by shifting production toward lighter pigments (pheomelanin). Some small clinical trials have reported measurable skin lightening effects, but the evidence base is limited by small sample sizes, short durations, and inconsistent methodology. This is not considered the primary clinical application of glutathione.
What is the "detox reaction" people report when starting glutathione?
When glutathione mobilizes stored toxins and heavy metals faster than the body's elimination pathways can clear them, the recirculating toxins trigger an inflammatory response. Symptoms mimic the flu: headaches, body aches, fatigue, brain fog, nausea, and chills. This is a temporary reaction to the pace of detoxification, not a harmful side effect of glutathione itself. The standard recommendation is to start at a low dose and increase gradually over several weeks.
Should I take glutathione or GlyNAC?
Based on available evidence, the choice depends on which bottleneck is limiting your glutathione status. If the issue is raw material shortage (common in aging, when both cysteine and glycine become limiting), GlyNAC (which has the strongest RCT evidence) addresses synthesis directly [12]. If the issue is impaired synthesis capacity, direct glutathione delivery may be more appropriate. Many practitioners suggest combining approaches. Consulting a healthcare professional can help determine the best strategy for your individual situation.
Sources & References
[1] Lu SC. "Glutathione synthesis." Biochimica et Biophysica Acta. 2013;1830(5):3143-3153. PMID: 22910582. Comprehensive review of GSH synthesis, redox biology, mitochondrial GSH pool, Phase II conjugation, and age-related decline.
[2] Mak TW et al. "Glutathione Primes T Cell Metabolism for Inflammation." Immunity. 2017;46(4):675-689. PMID: 28423341. Landmark study demonstrating T-cell metabolic gating by GSH via Gclc conditional knockout.
[3] Forman HJ et al. "Glutathione: overview of its protective roles, measurement, and biosynthesis." Molecular Aspects of Medicine. 2009;30(1-2):1-12. PMID: 18926850. GSH/GSSG ratio as cellular stress indicator.
[4] Klein Geltink RI et al. "Caught in the cROSsfire: GSH Controls T Cell Metabolic Reprogramming." Immunity. 2017;46(4):525-527. PMID: 28423332. Commentary on the calcineurin-NFAT-Myc-mTOR signaling cascade requiring GSH buffering.
[5] Referenced in Klein Geltink RI et al. (2017) and Mak TW et al. (2017). Metabolic reprogramming in T cells.
[6] Grusdat M et al. "Glutathione is critical for NK cell-mediated immunity." Cell Reports. 2026. Gclc-deficient NK cell studies.
[7] Peterson JD et al. "Glutathione levels in antigen-presenting cells modulate Th1 versus Th2 response patterns." Proceedings of the National Academy of Sciences. 1998;95(6):3071-3076. GSH:GSSG ratio in APCs controlling IL-12 and Th1/Th2 polarization.
[8] Yue M et al. "NAD+ metabolic network and immune regulation." Cell & Biosciences. 2023;13:81. NADPH-glutathione axis, NAD+ depletion cascade.
[9] Richie JP et al. "Randomized controlled trial of oral glutathione supplementation on body stores of glutathione." European Journal of Nutrition. 2015;54(2):251-263. PMID: 24791752. 6-month RCT, n=54, 250 mg and 1000 mg/day groups.
[10] Sinha R et al. "Oral supplementation with liposomal glutathione elevates body stores of glutathione and markers of immune function." European Journal of Clinical Nutrition. 2018;72(1):105-111. PMID: 28853742. Pilot study, n=12, liposomal GSH.
[11] Yan Z et al. "NAD+ metabolic network in immune regulation." Cellular & Molecular Immunology. 2022;19:1079-1101. NAD+/NADPH/glutathione recycling connection.
[12] Kumar P et al. "Supplementing Glycine and N-Acetylcysteine (GlyNAC) in Older Adults Improves Glutathione Deficiency, Oxidative Stress, Mitochondrial Dysfunction, Inflammation, Physical Function, and Aging Hallmarks." Journals of Gerontology: Series A. 2023;78(1):75-89. PMID: 35975308. Baylor College of Medicine RCT, 24 weeks.
[13] Hadzic T et al. "Dendritic cell glutathione and T-cell polarization via IL-27." PMID: 21545428.
[14] Polonikov A. "Endogenous Deficiency of Glutathione as the Most Likely Cause of Serious Manifestations and Death in COVID-19 Patients." ACS Infectious Diseases. 2020. PMID: 32463221.
[15] Labarrere CA, Kassab GS. "Glutathione deficiency in the pathogenesis of SARS-CoV-2 infection and its effects upon the host immune response in severe COVID-19 disease." Frontiers in Microbiology. 2022;13:979719. PMID: 36274722.
Related Peptide Guides
- NAD+ — The recycling cofactor glutathione depends on for regeneration
- SS-31 — Targeted mitochondrial protection (cardiolipin stabilization)
- KPV — Anti-inflammatory peptide targeting the NF-kB pathway
- Thymosin Alpha-1 — Immune modulation peptide (paired with glutathione in immune protocols)
- MOTS-C — Mitochondrial-derived peptide for metabolic function
- Selank — Anxiolytic peptide paired in immune protocol stacks
- BPC-157 — Tissue repair peptide (glutathione supports the repair environment)
- TB-500 — Healing peptide (complementary recovery support)
- GHK-Cu — Copper peptide with antioxidant and tissue remodeling effects
- Epithalon — Longevity peptide (telomere-focused aging intervention)
Need the reconstitution math for Glutathione: Complete Research Guide?
Open the calculator with Glutathione: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.