Adipotide: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Prohibitin-TP01, TP01, FTPP (Fat-Targeted Proapoptotic Peptide)
Attribute
Administration
- Detail
- Subcutaneous injection
Attribute
Research Status
- Detail
- Research Compound -- No FDA Approval. Phase I trial (NCT01262664) terminated; clinical development discontinued by 2019.
Attribute
Typical Dose Range
- Detail
- 250-1000 mcg/day subcutaneous (preclinical primate dose: 0.43 mg/kg/day)
Attribute
Half-Life
- Detail
- Not formally characterized in humans; preclinical data suggests rapid clearance
Attribute
Cycle Length
- Detail
- 28 days (based on primate and Phase I trial protocols)
Attribute
Storage
- Detail
- Lyophilized: -20C long-term; Reconstituted: 2-8C, use within 4 weeks
Overview / What Is Adipotide?
The Basics
Adipotide is unlike any other peptide in the fat loss space. Where most compounds work by suppressing appetite, boosting metabolism, or signaling fat cells to release their stored contents, Adipotide takes a fundamentally different approach: it cuts off the blood supply to fat tissue, causing the fat cells themselves to die.
The concept borrows from cancer therapy. Tumors need blood vessels to grow, and a class of anti-cancer drugs called anti-angiogenic agents work by starving tumors of their blood supply. Researchers at the University of Texas applied the same logic to fat tissue. White adipose tissue (the kind of fat that accumulates around the abdomen and organs) has its own dedicated blood vessel network. Adipotide was designed to home in on those specific blood vessels, bind to a protein called prohibitin on their surface, and deliver a cell-killing payload that destroys them. Without blood flow, the fat cells lose their oxygen and nutrient supply and undergo programmed cell death.
In obese monkeys, this approach produced dramatic results: roughly 11% body weight loss and 27% reduction in abdominal fat volume in just four weeks, along with substantial improvements in insulin sensitivity. However, the same studies revealed a significant safety concern. The compound caused reversible kidney damage, elevating creatinine levels in a pattern consistent with proximal tubular dysfunction. A Phase I human trial was initiated at MD Anderson Cancer Center in obese men with advanced prostate cancer, but the trial was terminated, and clinical development was discontinued by 2019.
Adipotide should be understood as a proof-of-concept agent that demonstrated the feasibility of vascular-targeted anti-adipose therapy, not as a viable current therapeutic option. Its historical significance lies in establishing that fat tissue can be pharmacologically reduced by attacking its blood supply, a concept that continues to inform newer nanoparticle-based approaches.
The Science
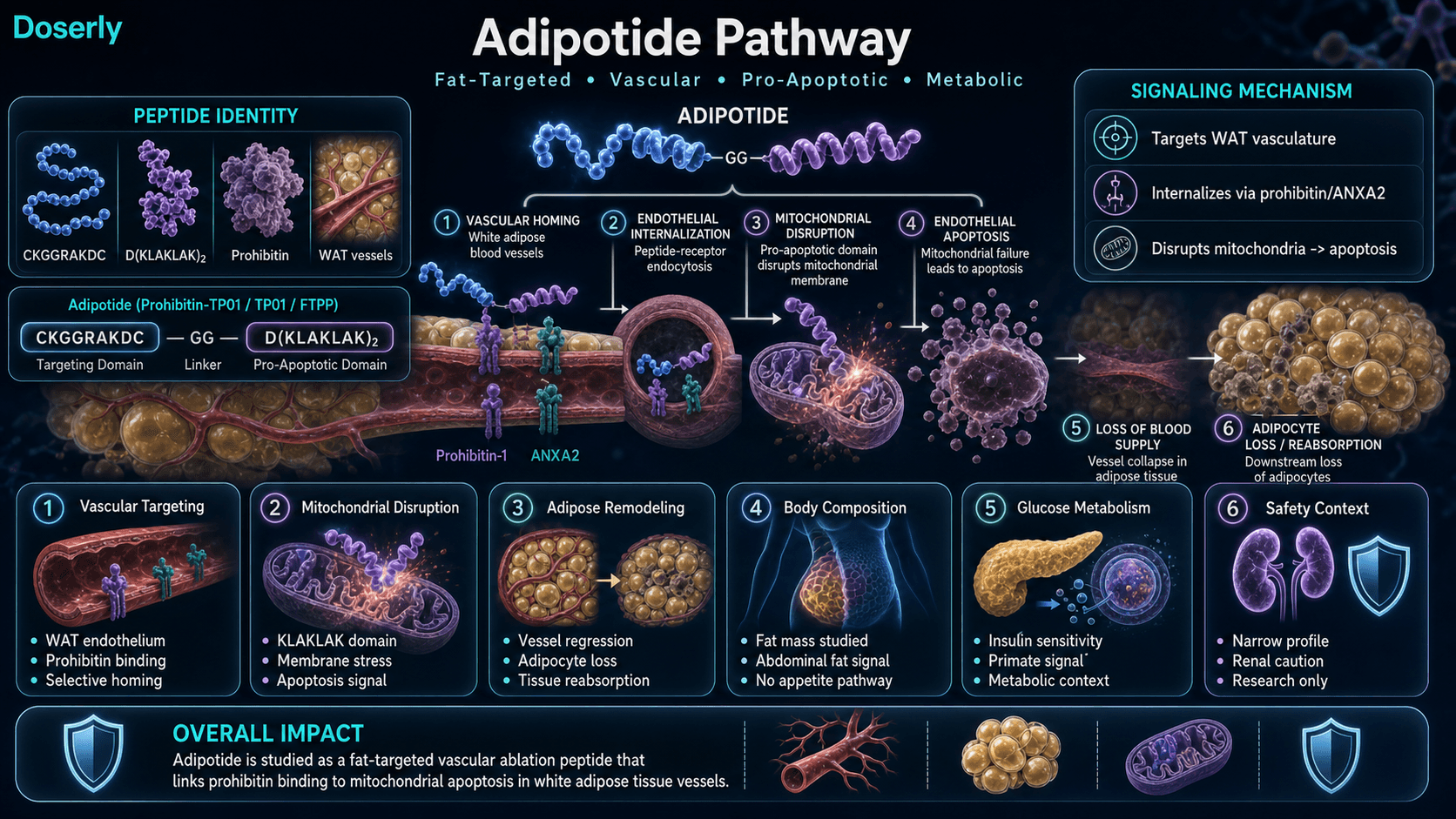
Adipotide (Prohibitin-TP01) is a chimeric peptidomimetic with the sequence CKGGRAKDC-GG-D(KLAKLAK)2. It comprises two functional domains: a targeting peptide (CKGGRAKDC) that binds to prohibitin and annexin A2 (ANXA2) on the endothelial surface of blood vessels supplying white adipose tissue, and a pro-apoptotic domain [D(KLAKLAK)2] that disrupts mitochondrial membranes upon internalization, triggering apoptosis of the targeted endothelial cells [1][2].
The selectivity of the targeting domain is mediated by prohibitin's preferential expression on WAT vasculature. Staquicini et al. (2011) confirmed the ANXA2-prohibitin receptor system as the binding partner in human white adipose tissue vasculature through combinatorial selection in cancer patients [3].
The original construct was developed by Kolonin et al. (2004), who demonstrated that targeted ablation of adipose vasculature in diet-induced obese and genetically obese (Lep ob/ob) C57BL/6 mice produced approximately 30% body weight reduction with resorption of white adipose tissue, improved hepatic steatosis, and normalization of serum lipids, without apparent acute systemic toxicity [4].
Barnhart et al. (2011) extended this work to obese rhesus macaques, demonstrating 11% mean body weight loss in 28 days at 0.43 mg/kg subcutaneous once daily, with 27% reduction in abdominal fat volume confirmed by MRI and DEXA. Insulin sensitivity improved substantially, with approximately 50% reduction in insulin requirements on clamp testing [1]. GLP toxicology studies in lean monkeys at 0.25, 0.43, and 0.75 mg/kg SC daily for 28 days revealed dose-dependent elevations in serum creatinine without proportional BUN increases, interpreted as reversible proximal tubular transport dysfunction rather than glomerular injury [1].
A first-in-human Phase I trial (NCT01262664) was designed for men with metastatic castrate-resistant prostate cancer and obesity, using subcutaneous once-daily dosing for 28 days starting at 0.03 mg/kg/day in a 3+3 dose-escalation design [5]. The trial was terminated, and a later systems-biology review noted that the program was discontinued by 2019 for unspecified reasons [5].
Molecular Identity
Attribute
Common Names
- Detail
- Adipotide, Prohibitin-TP01, TP01, FTPP (Fat-Targeted Proapoptotic Peptide)
Attribute
Sequence
- Detail
- CKGGRAKDC-GG-D(KLAKLAK)2
Attribute
Full Amino Acid Sequence
- Detail
- Cys-Lys-Gly-Gly-Arg-Ala-Lys-Asp-Cys-Gly-Gly-(D-Lys-Leu-Ala-D-Lys-Leu-Ala-D-Lys)2
Attribute
Molecular Formula
- Detail
- C152H252N44O42
Attribute
Molecular Weight
- Detail
- 2611.41 g/mol
Attribute
Structural Type
- Detail
- Chimeric peptidomimetic (targeting domain + pro-apoptotic domain connected by GG linker)
Attribute
Targeting Domain
- Detail
- CKGGRAKDC (binds prohibitin/ANXA2 on WAT vasculature)
Attribute
Pro-Apoptotic Domain
- Detail
- D(KLAKLAK)2 (D-amino acid form; disrupts mitochondrial membranes)
Attribute
Binding Target
- Detail
- Prohibitin-1 and Annexin A2 on endothelial cells of white adipose tissue vasculature
Attribute
Appearance
- Detail
- White to off-white lyophilized powder
Mechanism of Action
The Basics
Most fat loss compounds work like turning down the thermostat or reducing the food supply to fat cells. Adipotide works more like cutting the power lines. Instead of telling fat cells to shrink or release their contents, it destroys the blood vessels that keep them alive.
Here is how it works in two steps. First, the front end of the Adipotide molecule acts like a homing device. It circulates through the bloodstream looking for a specific protein called prohibitin, which appears on the surface of blood vessels that feed white fat tissue. This protein is not typically found on blood vessels elsewhere in the body, which is what gives Adipotide its selectivity.
Second, once Adipotide locks onto prohibitin and gets pulled inside the endothelial cell, its back end goes to work. This portion of the molecule is specifically designed to punch holes in mitochondrial membranes (the energy-producing structures inside cells). When the mitochondria are disrupted, the cell triggers its own self-destruct sequence, a process called apoptosis. The endothelial cells lining the blood vessel die, the vessel collapses, and the fat cells it was supplying lose their oxygen and nutrient delivery. Without blood flow, the fat cells die too and are gradually reabsorbed by the body.
The reason this approach generated excitement in research circles is that it could theoretically produce permanent fat reduction. Unlike dieting, which shrinks fat cells but leaves them intact and ready to refill, destroying fat cells through vascular starvation could reduce the total number of fat cells in the body. Whether this actually translates to lasting benefit in humans remains unknown.
The Science
Adipotide's mechanism operates through a two-step ligand-directed apoptosis cascade targeting the WAT vascular endothelium [1][2][4]:
Step 1: Vascular Homing. The N-terminal targeting domain (CKGGRAKDC) binds to a receptor complex comprising prohibitin-1 (PHB1) and annexin A2 (ANXA2) on the luminal surface of endothelial cells in white adipose tissue microvasculature. Staquicini et al. (2011) validated this receptor system through phage display-based vascular ligand-receptor mapping in human subjects, confirming that the ANXA2-PHB heterodimer serves as a functional receptor for the CKGGRAKDC motif on WAT endothelium [3]. Prohibitin expression appears to be selectively enriched on adipose vasculature under normal physiological conditions, providing the basis for tissue-targeted delivery [1][3].
Step 2: Mitochondrial Disruption and Apoptosis. Following receptor-mediated internalization, the C-terminal pro-apoptotic domain D(KLAKLAK)2, composed of D-amino acids for protease resistance, integrates into mitochondrial membranes and disrupts membrane potential. This triggers cytochrome c release, caspase cascade activation, and ultimately apoptosis of the targeted endothelial cells [1][4]. The resulting vascular rarefaction deprives downstream adipocytes of perfusion, leading to ischemic injury, adipocyte apoptosis, and resorption of white adipose tissue [4].
Downstream Metabolic Effects. In preclinical models, the ablation of WAT vasculature and subsequent adipose resorption produced improvements in metabolic parameters including increased energy expenditure, reversal of hepatic steatosis, normalization of serum lipids, and improved glucose handling [1][4]. In obese primates, insulin sensitivity improved substantially, with approximately 50% reduction in insulin requirements measured by hyperinsulinemic-euglycemic clamp [1].
Pathway Visualization Image
Pharmacokinetics
The Basics
Formal pharmacokinetic data for Adipotide in humans is extremely limited. The compound has not been characterized with the same level of detail as most therapeutic peptides, because clinical development was discontinued early.
What is known comes primarily from the primate studies. The compound is administered subcutaneously and appears to be absorbed into the bloodstream where it circulates until encountering its target (prohibitin on fat tissue blood vessels). The timeline of effects in primates suggests that the biological activity unfolds over days to weeks rather than hours. Weight loss in the primate study was progressive over the 28-day dosing period, and some community reports suggest that fat reduction may continue for several weeks after the last injection, as blood vessels that were damaged during the dosing period continue to deteriorate and the fat cells they supplied continue to die.
The pro-apoptotic domain is constructed from D-amino acids (mirror-image versions of the natural L-amino acids), which makes it resistant to the enzymes that normally break down peptides. This design feature likely extends the functional half-life of the molecule compared to standard L-amino acid peptides, though the exact duration has not been quantified.
The compound is eliminated through normal peptide degradation pathways. The principal safety signal from primate studies (elevated serum creatinine) suggests that degradation products or metabolic byproducts from fat cell death are processed through the kidneys, potentially creating a burden on proximal tubular transport mechanisms.
The Science
Formal pharmacokinetic parameters (Cmax, Tmax, AUC, clearance, volume of distribution) have not been published for Adipotide in any species. The D-amino acid composition of the pro-apoptotic domain [D(KLAKLAK)2] confers resistance to endogenous peptidases, which would be expected to extend plasma half-life relative to L-amino acid peptides of comparable size [1].
In the primate efficacy study, subcutaneous administration at 0.43 mg/kg once daily for 28 days produced progressive weight loss throughout the treatment period, with metabolic improvements (insulin sensitivity, fat volume reduction) documented by MRI, DEXA, and clamp testing at study conclusion [1]. The absence of published PK data from the terminated Phase I human trial (NCT01262664) represents a significant knowledge gap [5].
The renal signal observed in primate GLP toxicology studies (elevated creatinine without proportional BUN elevation at 0.25-0.75 mg/kg/day) was interpreted as proximal tubular transport dysfunction rather than glomerular damage, and was dose-dependent and reversible upon treatment cessation [1]. This suggests that either the intact compound, its metabolites, or the metabolic load from adipocyte apoptosis and resorption creates a transient burden on renal tubular function.
Research & Clinical Evidence
Adipotide and Fat Loss
The Basics
The fat loss evidence for Adipotide is a study in contrasts: spectacular results in animals, a terminated human trial, and deeply mixed community reports.
In mice, the results were striking. Diet-induced obese mice treated with the Adipotide precursor construct showed approximately 30% body weight reduction with resorption of white adipose tissue. The effect was not dependent on reduced food intake, confirming that the weight loss came from destroying fat tissue rather than appetite suppression.
In obese rhesus monkeys, a 28-day course of Adipotide at 0.43 mg/kg/day produced roughly 11% mean body weight loss and 27% reduction in abdominal fat volume, confirmed by MRI and DEXA imaging. These are impressive numbers for a 4-week intervention, and they came with a substantial bonus: approximately 50% reduction in insulin requirements, suggesting meaningful improvement in metabolic health.
The human picture is far less clear. A Phase I trial was initiated in 2011 at MD Anderson Cancer Center, enrolling obese men with metastatic prostate cancer. The trial used a 3+3 dose-escalation design starting at 0.03 mg/kg/day for 28 days. However, the trial was terminated and detailed efficacy data were never published. Community reports from individuals who have self-administered Adipotide are mixed, with some reporting modest fat loss (3-7 lbs over 28 days) and others reporting no measurable change. A recurring theme in community discussion is whether the doses commonly used (0.5-1 mg/day regardless of body weight) are too low to achieve the effects seen in primate studies, where the effective dose translated by body surface area scaling would be substantially higher.
The Science
Mouse Studies: Kolonin et al. (2004) demonstrated that targeted ablation of adipose vasculature in diet-induced obese C57BL/6 mice and genetically obese Lep(ob/ob) mice using the CKGGRAKDC-GG-D(KLAKLAK)2 construct produced approximately 30% body weight reduction over 4 weeks. White adipose tissue was resorbed, with improved hepatic and skeletal muscle fat content, without apparent acute systemic toxicity [4].
Primate Studies: Barnhart et al. (2011) treated spontaneously obese rhesus macaques with metabolic syndrome at 0.43 mg/kg SC once daily for 28 days. Results included 11% mean body weight loss, 27% reduction in abdominal fat volume (MRI/DEXA), and approximately 50% reduction in insulin requirements on hyperinsulinemic-euglycemic clamp. Weight loss was not associated with reduced food intake, confirming a direct fat-ablation mechanism rather than appetite-mediated effects [1].
Glucose Tolerance: Kim et al. (2012) demonstrated rapid and weight-independent improvement in glucose tolerance induced by Adipotide in preclinical models, suggesting that the metabolic benefits extend beyond simple weight reduction and may reflect direct effects of adipose tissue reduction on insulin signaling [6].
Human Trial: The Phase I trial (NCT01262664) at MD Anderson enrolled men with metastatic castrate-resistant prostate cancer and obesity. The protocol specified SC once-daily dosing for 28 days starting at 0.03 mg/kg/day with 3+3 dose escalation. The trial was terminated, and publicly available summaries emphasize safety and renal effects rather than efficacy outcomes. Detailed results were not published [5].
Adipotide and Cancer Research
The Basics
Prohibitin, the protein that Adipotide targets on fat tissue blood vessels, is also found on certain cancer cells. This overlap has generated interest in whether Adipotide or similar vascular-targeting strategies could be applied to cancer treatment. The original Phase I human trial was designed specifically for cancer patients (men with metastatic prostate cancer), reflecting the hypothesis that modifying adiposity and the adipokine milieu could influence tumor biology.
This remains a theoretical area of research. The potential to develop compounds that target prohibitin in cancer tissue could lead to therapies that attack tumors by cutting their blood supply, similar to existing anti-angiogenic cancer drugs but with potentially greater selectivity.
The Science
Staquicini et al. (2011) performed vascular ligand-receptor mapping through direct combinatorial selection in cancer patients, identifying prohibitin as a receptor for peptide-based vascular targeting [3]. The dual expression of prohibitin on both adipose vasculature and certain tumor vasculature has positioned the Adipotide paradigm as a platform for vascular-targeted nanotherapies, with newer research incorporating the targeting principle into nanoparticle-based drug delivery systems [3][5].
Biomarker Evidence Matrix
The table below scores Adipotide across relevant biomarker categories based on two dimensions: Evidence Strength (quality of research data) and Reported Effectiveness (community-reported outcomes from the Sentiment Analysis).
Category
Fat Loss
- Evidence Strength
- 6/10
- Reported Effectiveness
- 4/10
- Summary
- Strong preclinical data in mice (~30% BW reduction) and primates (~11% BW loss, ~27% abdominal fat reduction in 4 weeks). Phase I trial terminated without published efficacy data. Community reports are deeply mixed, with many users reporting no measurable change.
Category
Weight Management
- Evidence Strength
- 5/10
- Reported Effectiveness
- 3/10
- Summary
- Primate data shows substantial weight reduction, but no human efficacy data published. Community reports range from 0 to 12 lbs over 28 days, with most users reporting modest or no results.
Category
Side Effect Burden
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Primate GLP toxicology identified dose-dependent reversible renal tubular dysfunction. Most community users at low doses (0.5-1mg/day) report tolerable side effects with clean kidney labs. Injection site reactions (burning, itching) are consistently reported but manageable.
Category
Nausea & GI Tolerance
- Evidence Strength
- 3/10
- Reported Effectiveness
- 7/10
- Summary
- No preclinical data on GI effects. Community reports show no nausea or GI issues, which is notable compared to GLP-1 agonists.
Category
Appetite & Satiety
- Evidence Strength
- 3/10
- Reported Effectiveness
- 3/10
- Summary
- Primate study found decreased food consumption secondary to fat loss, not through appetite pathway targeting. Most community users report no appetite changes.
Category
Fluid Retention
- Evidence Strength
- 2/10
- Reported Effectiveness
- 5/10
- Summary
- No formal data. Community reports note increased urination and dehydration risk during use.
Category
Treatment Adherence
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Daily injection protocol for 28 days is straightforward, but injection site discomfort and anxiety about kidney safety create adherence challenges.
Category
Inflammation
- Evidence Strength
- 3/10
- Reported Effectiveness
- 3/10
- Summary
- No direct anti-inflammatory data. The mechanism involves inducing vascular destruction and cell death, which would be expected to trigger local inflammatory responses.
Category
Skin Health
- Evidence Strength
- 1/10
- Reported Effectiveness
- 3/10
- Summary
- Single community report of improved vascularity, likely secondary to subcutaneous fat reduction.
Category
Daily Functioning
- Evidence Strength
- 2/10
- Reported Effectiveness
- 6/10
- Summary
- No clinical data. Community users generally report no impairment to daily activities or strength during use.
Categories not scored (insufficient data): Muscle Growth, Food Noise, Sleep Quality, Focus & Mental Clarity, Memory & Cognition, Mood & Wellbeing, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Joint Health, Pain Management, Recovery & Healing, Physical Performance, Gut Health, Digestive Comfort, Hair Health, Heart Health, Blood Pressure, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Body Image, Immune Function, Bone Health, Longevity & Neuroprotection, Cravings & Impulse Control, Social Connection, Withdrawal Symptoms, Other.
Benefits & Potential Effects
The Basics
Adipotide's benefit profile is narrow and highly theoretical. Its primary claimed benefit is targeted fat cell destruction through vascular ablation, a mechanism distinct from every other fat loss approach available. Rather than shrinking fat cells (which can refill), Adipotide aims to permanently eliminate them by cutting their blood supply.
In primate studies, this mechanism produced three notable effects: substantial body weight reduction (11% in 4 weeks), dramatic reduction in abdominal fat volume (27%), and meaningful improvement in insulin sensitivity (50% reduction in insulin requirements). These effects occurred without changes in food intake, confirming that the mechanism is direct fat ablation rather than appetite suppression.
The appeal of permanent fat cell reduction is significant in theory. When people lose weight through diet and exercise, their fat cells shrink but remain present and metabolically active, ready to refill when caloric surplus returns. This is a major driver of weight regain after dieting. If Adipotide could safely reduce the total number of fat cells, it could theoretically address this problem at its root.
However, several important caveats apply. First, the human data is essentially nonexistent. The terminated Phase I trial never published efficacy results. Second, the compound causes kidney problems at effective doses in primates. Third, community reports from self-administration are mixed at best, with many users reporting no detectable benefit. Fourth, the dose commonly used by community members (0.5-1 mg/day) may be far below the therapeutically effective dose based on body surface area scaling from primate studies.
For these reasons, Adipotide should be understood as a fascinating research tool and proof-of-concept rather than a practical fat loss option. Modern GLP-1 receptor agonists (semaglutide, tirzepatide, retatrutide) achieve 15-24% body weight reduction with well-characterized safety profiles, making them far more practical alternatives.
The Science
The demonstrated and proposed benefits of Adipotide, based on available preclinical evidence:
Targeted Adipose Vascular Ablation: The chimeric peptidomimetic selectively targets prohibitin/ANXA2 on WAT endothelium and induces apoptosis through mitochondrial membrane disruption, producing vascular rarefaction, adipocyte ischemia, and WAT resorption [1][4].
Fat Mass Reduction: Preclinical data demonstrates approximately 30% body weight reduction in obese mice [4] and approximately 11% body weight loss with 27% reduction in abdominal fat volume in obese primates over 28 days [1].
Insulin Sensitivity Improvement: Obese primates treated with Adipotide showed approximately 50% reduction in insulin requirements on hyperinsulinemic-euglycemic clamp testing [1]. Kim et al. (2012) demonstrated rapid, weight-independent glucose tolerance improvement, suggesting metabolic benefits beyond simple adipose reduction [6].
Hepatic and Lipid Improvements: In rodent models, adipose ablation reversed hepatic steatosis and normalized serum lipid profiles [4].
Potential Permanent Fat Cell Reduction: Unlike compounds that modulate fat cell metabolism (lipolysis, lipogenesis), Adipotide's mechanism destroys adipocytes entirely, which could theoretically reduce fat cell hyperplasia and lower the set point for fat regain. This hypothesis remains untested in humans.
The benefits outlined above span multiple body systems, and your experience will be uniquely yours. Rather than guessing which effects are attributable to this compound versus other factors in your life, Doserly helps you log specific outcomes alongside your protocol details, building a clear picture of what's changing and when.
Over weeks and months, this creates something more useful than any anecdotal report: your own evidence-based record of how this compound affects you personally, at your specific dose, within the context of your full health protocol. When it's time to decide whether to continue, adjust, or discontinue, you have real data to inform that conversation with your healthcare provider.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
Side Effects & Safety Considerations
The Basics
Adipotide's safety profile is the primary reason clinical development was discontinued, and it is the central concern in any discussion of this compound. The core issue is kidney toxicity.
In obese rhesus monkeys, Adipotide caused elevations in serum creatinine without proportional increases in BUN (blood urea nitrogen). This pattern suggests damage to the proximal tubules in the kidneys (the structures responsible for reabsorbing filtered substances) rather than damage to the glomeruli (the primary filtering units). The finding was dose-dependent, appearing most prominently at higher doses (0.75 mg/kg/day), and was reversible when treatment was stopped.
The interpretation from researchers is that the kidney signal is "predictable and reversible renal tubular toxicity," likely resulting from the metabolic burden of processing dead fat cells and their breakdown products. When large volumes of adipose tissue are destroyed rapidly, the debris must be cleared through the kidneys, potentially overwhelming the proximal tubular transport capacity.
Community users who have self-administered Adipotide at lower doses (0.5-1 mg/day) generally report tolerable side effects. Injection site reactions are the most consistent complaint: mild burning, itching, and occasional sharp pin-prick sensations at the injection site that resolve within minutes to hours. Several users who checked kidney function via blood work during or after 28-day cycles reported normal results at these lower doses.
The most publicized safety concern involves the death of bodybuilder Bostin Loyd, which was widely attributed to Adipotide in community discussions. However, detailed investigation reveals that Loyd was reportedly using 5+ mg/day (5-10 times the commonly cited dose), was concurrently using multiple other anabolic and performance-enhancing substances, and his actual cause of death was a retrograde aortic dissection with a suspected genetic component. While Adipotide may have contributed to kidney stress, attributing his death solely to this compound oversimplifies a case with many confounding factors.
Other potential concerns based on mechanism and limited data include: alteration of adipose vasculature that could impact wound healing and local tissue perfusion; chronic exposure risks including adipose atrophy, adipokine dysregulation, or off-target vascular effects; and constitutional symptoms (malaise, fatigue) that are plausible but insufficiently characterized.
The Science
Renal Toxicity (Primary Safety Signal): GLP toxicology studies in lean rhesus macaques at 0.25, 0.43, and 0.75 mg/kg SC daily for 28 days demonstrated dose-dependent elevations in serum creatinine without proportional BUN elevation, consistent with proximal tubular transport dysfunction rather than glomerular injury [1]. The finding was reversible upon treatment cessation and was described as predictable based on the mechanism of action [1].
Injection Site Reactions: Community reports consistently describe mild, transient burning and itching at subcutaneous injection sites, typically resolving within 3-5 minutes. Occasional sharp pin-prick sensations reported throughout the day at injection sites [community data].
No Systemic Toxicity in Rodents: Kolonin et al. (2004) reported no obvious acute systemic toxicity in diet-induced obese mice treated with the Adipotide construct over 4 weeks [4].
Clinical Trial Safety: The Phase I trial (NCT01262664) was terminated. Publicly available summaries emphasize safety, pharmacokinetics, and renal effects, but detailed adverse event data has not been published [5].
Potential Off-Target Effects: Prohibitin expression, while enriched on WAT vasculature, has been identified on other tissue types including certain cancer cells [3]. The theoretical risk of off-target vascular effects in non-adipose tissues has not been systematically evaluated in humans.
Side effect profiles are most useful when you can compare them against your own experience in real time. Doserly lets you log symptoms, severity, and timing alongside your dosing data, creating a side-by-side view of your protocol and your body's response.
This kind of systematic tracking catches things that memory alone misses. A subtle mood shift that began three days after a dose increase. Sleep disruption that correlates with evening administration. These patterns become visible when the data is laid out on a timeline, and they give your healthcare provider actionable information rather than vague concerns. Early detection of emerging side effects means earlier intervention.
Keep side effects, flags, and follow-up notes visible.
Doserly helps you document safety observations, side effects, medication changes, and follow-up questions so important context is not scattered.
Safety log
Flags and notes

Safety notes are not emergency guidance; seek medical help when appropriate.
Dosing Protocols
The Basics
Dosing information for Adipotide is characterized by significant uncertainty. Unlike most peptides discussed in these guides, Adipotide has no established human dosing protocol. The available information comes from primate studies, a terminated Phase I trial protocol, and community self-experimentation.
The most commonly cited community protocol is weight-based: approximately 0.01 mg/kg/day (4.53 mcg per pound of body weight), administered subcutaneously once daily for 28 days. For a 200 lb (91 kg) person, this equates to roughly 910 mcg (0.91 mg) per day.
An alternative approach favored by some sources involves conservative titration: starting at 250 mcg/day for 2 weeks, increasing by 250 mcg every 2 weeks, up to a maximum of 1000 mcg (1 mg) by weeks 7-8. This graduated approach is intended to mitigate potential renal side effects by allowing monitoring at each dose level before escalation.
The 28-day cycle length is derived directly from the primate efficacy study and the Phase I trial protocol. Most community sources recommend a rest period of at least 4-6 weeks between cycles, during which kidney function should be assessed.
A critical observation from community discussion and pharmacological scaling calculations: the doses most people use (0.5-1 mg/day) may be substantially sub-therapeutic. The effective primate dose of 0.43 mg/kg/day translates to a much higher human dose when properly scaled by body surface area. This dosing gap is a plausible explanation for the many reports of inefficacy in community self-experiments.
The Science
No standardized human dosing protocol exists for Adipotide. Available dosing data comes from:
Primate Efficacy Study: Barnhart et al. (2011) demonstrated efficacy at 0.43 mg/kg SC once daily for 28 days in obese rhesus macaques. GLP toxicology evaluated 0.25, 0.43, and 0.75 mg/kg/day [1].
Phase I Human Trial: NCT01262664 specified a starting dose of 0.03 mg/kg/day SC with 3+3 dose escalation over 28 days. This starting dose represents approximately 2.1 mg/day for a 70 kg human, substantially higher than the 0.5-1 mg/day doses used in community self-experimentation [5].
Body Surface Area Scaling: Applying FDA body surface area allometric scaling from the primate efficacy dose (0.43 mg/kg in rhesus macaque; Km = 12) to human (Km = 37) yields a human equivalent dose of approximately 0.14 mg/kg/day, or approximately 9.8 mg/day for a 70 kg human. This is approximately 10x higher than typical community doses [1].
Community Protocols: Weight-based dosing at 0.01 mg/kg/day (4.53 mcg/lb) for 28 days is the most commonly cited protocol, with no published evidence supporting this specific dose level. The discrepancy between this dose and BSA-scaled doses may explain the inconsistent efficacy reports [community data].
The dosing protocols above involve numbers that matter: specific microgram amounts, reconstitution ratios, and timing windows. Getting any of these wrong compounds across every subsequent dose from that vial.
Doserly's dose and reconstitution calculators eliminate the guesswork. Enter your vial size, peptide amount, and target dose, and get the exact bacteriostatic water volume, units per tick mark, and doses per vial. The injection site tracker maps your administration history as a visual heat map across your body, flagging areas that need rest and suggesting rotation patterns. Combined with dose reminders that include compound name, amount, and route, every aspect of your daily protocol is handled with the precision it requires.
Turn symptom and safety notes into a clearer timeline.
Doserly helps you log doses, symptoms, and safety observations side by side so patterns are easier to discuss with a qualified clinician.
Pattern view
Logs and observations

Pattern visibility is informational and should be reviewed with a clinician.
What to Expect
Adipotide's expected timeline is less well-characterized than most peptides due to limited human data and mixed community reports. The following is based on the primate study timeline and community N=1 reports.
Days 1-3: Injection site reactions are the most commonly reported early experience. Mild burning and itching at the injection site lasting 3-5 minutes, with occasional sharp pin-prick sensations throughout the day. Some users report these diminish after the first few injections. No systemic effects are typically noticed.
Days 4-14: Most community users report no perceptible changes during the first two weeks. The mechanism of action (vascular destruction leading to adipocyte death) is a slow-onset process. Users who track body weight may see some fluctuation, but this is difficult to distinguish from normal daily variation. Increased urination has been reported by some users, possibly reflecting early metabolic processing of damaged tissue.
Days 15-28: If efficacy is going to be observed, subtle changes may begin to emerge during this period. The primate study showed progressive weight loss throughout the 28-day treatment period. Community users who report positive results typically describe gradual fat reduction in areas with high white adipose tissue concentration (abdomen, love handles).
Days 29-56 (Post-Cycle): Several community reports and the primate data suggest that fat loss may continue for weeks after the last injection. The hypothesis is that blood vessels damaged during the dosing period continue to deteriorate, and fat cells progressively lose viability as their compromised vascular supply fails. One user reported continued weight loss of 1 lb/week for 3 weeks post-cycle before stalling.
Setting Expectations: Community data is deeply divided. Roughly half of detailed N=1 reports describe modest positive results (3-7 lbs fat loss over a full cycle), while the other half report no measurable change. The "delayed onset" hypothesis suggests that evaluating results at day 28 may be premature, with full effects potentially not apparent until 4-6 weeks post-cycle. However, this remains unconfirmed in controlled settings.
Interaction Compatibility
Good With (Potentially Complementary Compounds)
- Retatrutide -- Triple agonist (GLP-1/GIP/glucagon) provides appetite suppression and metabolic support through entirely different receptor pathways. One community user reported maintaining Adipotide-induced fat loss with retatrutide. No known pharmacological interaction.
- Semaglutide -- GLP-1 agonist for appetite suppression. Different mechanism (incretin signaling vs vascular ablation). Several community members switched from Adipotide to GLP-1 agonists after finding them more effective.
- Tirzepatide -- Dual GIP/GLP-1 agonist. Same complementary logic as semaglutide.
- AOD-9604 -- One community user reported combining Adipotide with AOD-9604, though the added benefit of AOD-9604 in this context is unclear given both target fat loss through different mechanisms.
Not Good With (Caution or Contraindication)
- Nephrotoxic Compounds -- Given Adipotide's primary safety signal of renal tubular dysfunction, concurrent use of any compound with known kidney toxicity should be avoided. This includes high-dose NSAIDs, certain antibiotics, and other compounds processed through the kidneys.
- Anti-Angiogenic Agents -- Compounds that inhibit blood vessel formation could theoretically amplify Adipotide's vascular destruction beyond the intended target tissue.
- Concurrent SARMs/AAS -- The case of Bostin Loyd, who was on multiple anabolic and performance-enhancing substances alongside high-dose Adipotide, suggests that stacking with compounds that stress multiple organ systems simultaneously significantly increases risk.
Administration Guide
Adipotide is administered via subcutaneous injection. The following general practices are reported in community and research protocols:
Materials typically required:
- Insulin syringes (U-100, 29-31 gauge)
- Alcohol swabs
- Bacteriostatic water (for reconstitution)
- Sharps disposal container
Recommended reconstitution solution: Bacteriostatic water is the standard reconstitution solution. A common reconstitution volume is 3.0 mL per 10 mg vial, yielding a concentration of approximately 3.33 mg/mL. At this concentration, 1 unit on a U-100 insulin syringe equals approximately 33.33 mcg.
Timing considerations: No specific timing requirements (fasted vs fed) have been established for Adipotide. Community protocols typically specify daily administration at any consistent time. Injection site rotation is important due to the localized tissue effects reported by some users.
Post-administration care: Monitor for injection site reactions (burning, itching, sharp pain), which are commonly reported but typically resolve within minutes. Adequate hydration is emphasized by community users, as the metabolic processing of destroyed fat tissue creates additional renal burden. Some community protocols recommend kidney function monitoring (serum creatinine, BUN) at baseline, mid-cycle (day 14), end of cycle (day 28), and 4 weeks post-cycle.
Supplies & Planning
The following materials are generally associated with Adipotide subcutaneous protocols:
Peptide vials: Adipotide is commonly available in 10 mg vial sizes.
Reconstitution solution: Bacteriostatic water in 10 mL bottles. A recommended reconstitution volume of 3.0 mL per 10 mg vial yields approximately 3.33 mg/mL concentration.
Syringes: U-100 insulin syringes (29-31 gauge) for subcutaneous injection. One syringe per injection; never reuse syringes. For doses requiring small volumes (under 10 units), consider 30-unit or 50-unit insulin syringes for improved readability.
Alcohol swabs: For cleaning the vial stopper and injection site before each administration.
Sharps container: For safe disposal of used syringes and needles.
Blood work: Kidney function panels (at minimum: serum creatinine, BUN, eGFR) at baseline and post-cycle are strongly recommended given the known renal safety signal.
Consult with a healthcare provider for specific quantities and protocol planning.
Storage & Handling
Lyophilized (powder) form:
- Store at -20C (-4F) in dry, dark conditions for long-term storage
- Minimize moisture exposure; keep in sealed packaging with desiccant
- Allow vials to reach room temperature (10-30 minutes) before opening to prevent condensation
Reconstituted (liquid) form:
- Refrigerate immediately at 2-8C (35.6-46.4F) after reconstitution
- Use within 3-4 weeks (28 days) for optimal potency
- Do NOT freeze reconstituted solutions
- Avoid repeated freeze-thaw cycles
- Protect from light
Handling best practices:
- Swab vial stopper with alcohol before each draw
- Use sterile syringes for each draw
- Gently swirl or roll to dissolve during reconstitution; do not shake
- Inject bacteriostatic water slowly down the vial wall to avoid foaming
- Inspect reconstituted solution before each use; discard if cloudy, discolored, or contains particles
Lifestyle Factors
The lifestyle context around Adipotide differs from most peptides because the compound's mechanism (vascular ablation) is less dependent on metabolic state than compounds that modulate fat metabolism directly. However, several factors remain relevant:
Hydration: This is the single most important lifestyle factor for Adipotide use. The destruction of fat cells creates metabolic debris that must be cleared through the kidneys. Multiple community users emphasize the importance of aggressive hydration during and after Adipotide cycles. Inadequate water intake could exacerbate the renal tubular stress that represents the compound's primary safety concern.
Nutrition: While Adipotide does not require fasted administration or specific dietary timing, maintaining adequate nutrition supports the metabolic processing of destroyed adipose tissue. Protein intake is particularly important for preserving lean mass during any fat-loss period.
Exercise: Community reports do not indicate specific exercise requirements for Adipotide, and the compound's mechanism does not depend on creating metabolic demand for mobilized fatty acids (unlike lipolytic compounds such as AOD-9604). However, general physical activity supports metabolic health and may complement the insulin sensitivity improvements observed in preclinical studies.
Kidney Monitoring: Given the renal safety signal, proactive monitoring of kidney function through blood work is an important component of responsible use. Baseline labs before starting, mid-cycle testing if extending beyond 14 days, and post-cycle testing are commonly recommended practices in community protocols.
Sleep and Stress: While Adipotide does not directly interact with sleep or stress pathways, general metabolic health (which supports kidney function and tissue remodeling) benefits from adequate sleep and stress management.
Regulatory Status & Research Classification
United States (FDA): Adipotide (Prohibitin-TP01) has no FDA approval for any indication. It is classified as a research compound. The Phase I trial (NCT01262664) at MD Anderson Cancer Center was terminated, and clinical development was discontinued.
WADA Status: Adipotide's WADA status has not been explicitly addressed in published prohibited substance lists. However, as a non-approved pharmacological substance, it would likely fall under S0 (Non-Approved Substances) of the WADA Prohibited List. Athletes subject to drug testing should avoid Adipotide.
Clinical Development Status: As of 2019, clinical development of Adipotide has been discontinued. The compound originated from academic research at the University of Texas and was developed with Arrowhead Pharmaceuticals (formerly Arrowhead Research Corporation) involvement. No active clinical trials are registered as of 2026.
NCI Drug Dictionary: Adipotide is listed in the National Cancer Institute Drug Dictionary as "Prohibitin-targeting peptide 1."
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is Adipotide and how does it work?
Adipotide is a synthetic peptidomimetic designed to destroy fat cells by cutting off their blood supply. It targets a protein called prohibitin on the blood vessels that feed white adipose tissue. Once bound, it delivers a cell-killing payload that destroys the blood vessel lining, depriving fat cells of oxygen and nutrients and causing them to die. This is fundamentally different from other fat loss compounds, which typically work by suppressing appetite or modifying fat cell metabolism.
How effective is Adipotide for fat loss?
Based on available data, results are highly variable. In obese monkeys, 28 days of treatment produced approximately 11% body weight loss and 27% reduction in abdominal fat. In human self-experimentation (not controlled trials), results range from zero measurable change to approximately 5-7 lbs of fat loss over a 28-day cycle. Multiple users have concluded the compound is ineffective at commonly used doses. A plausible explanation for this variability is that the commonly used human dose (0.5-1 mg/day) may be substantially below the therapeutically effective dose when scaled from primate studies.
Is Adipotide safe?
The primary safety concern is kidney toxicity. Primate studies showed dose-dependent, reversible proximal tubular dysfunction (elevated creatinine without proportional BUN elevation). Community users at lower doses (0.5-1 mg/day) generally report tolerable side effects with normal kidney labs, but the long-term safety profile in humans is unknown. Clinical development was discontinued, at least in part, due to safety concerns. Anyone considering this compound should discuss it with a healthcare provider and include kidney function monitoring in their protocol.
Why was clinical development of Adipotide discontinued?
The Phase I trial (NCT01262664) was terminated, and the specific reasons have not been publicly disclosed. Contributing factors likely include the renal safety signal observed in primate studies, the limited patient population (men with metastatic prostate cancer and obesity), and strategic business decisions. The compound's development history does not necessarily indicate that it is ineffective, but it does indicate that the risk-benefit profile was not considered favorable enough to continue investment.
What dosage of Adipotide do sources describe?
Commonly reported ranges include 0.01 mg/kg/day (approximately 4.53 mcg per pound of body weight) administered subcutaneously once daily for 28 days. Some sources recommend a conservative titration starting at 250 mcg/day and increasing by 250 mcg every 2 weeks. The Phase I trial started at 0.03 mg/kg/day (approximately 2.1 mg/day for a 70 kg person). Readers should consult a qualified healthcare professional for any dosing decisions.
How does Adipotide compare to GLP-1 agonists for fat loss?
GLP-1 agonists (semaglutide, tirzepatide, retatrutide) work through entirely different mechanisms (appetite suppression and metabolic signaling via incretin receptors) and have demonstrated 15-24% body weight reduction in large clinical trials with well-characterized safety profiles. Adipotide's only completed efficacy data comes from primate studies showing 11% weight loss over 4 weeks, and the compound was never successfully tested in humans. Multiple community members who tried Adipotide subsequently switched to GLP-1 agonists, citing better results and greater safety confidence.
Can Adipotide permanently reduce fat cells?
In theory, yes. Unlike caloric restriction or metabolic compounds that shrink fat cells (which remain viable and can refill), Adipotide's mechanism destroys fat cells entirely through vascular ablation. In preclinical models, white adipose tissue was resorbed after treatment. Whether this produces lasting fat cell reduction in humans, and whether that translates to sustained lower body fat, remains unknown.
Sources & References
- Barnhart KF, Christianson DR, Hanley PW, et al. A peptidomimetic targeting white fat causes weight loss and improved insulin resistance in obese monkeys. Science Translational Medicine. 2011;3(108):108ra112. PubMed: 22072637
- Kolonin MG, Saha PK, Chan L, Pasqualini R, Arap W. Reversal of obesity by targeted ablation of adipose tissue. Nature Medicine. 2004;10(6):625-632. PubMed: 15133506
- Staquicini FI, Cardo-Vila M, Kolonin MG, et al. Vascular ligand-receptor mapping by direct combinatorial selection in cancer patients. Proceedings of the National Academy of Sciences. 2011;108(46):18637-18642. PubMed: 22049339
- Kolonin MG, Saha PK, Chan L, Pasqualini R, Arap W. Reversal of obesity by targeted ablation of adipose tissue. Nature Medicine. 2004;10(6):625-632. PubMed: 15133506
- ClinicalTrials.gov. A First-in-Man, Phase I Evaluation of a Single Cycle of Prohibitin Targeting Peptide 1 in Patients With Metastatic Prostate Cancer and Obesity. NCT01262664. ClinicalTrials.gov
- Kim DH, Woods SC, Seeley RJ. Rapid and weight-independent improvement of glucose tolerance induced by a peptide designed to elicit apoptosis in adipose tissue endothelium. Diabetes. 2012;61(9):2299-2310. PubMed: 22698916
Related Peptide Guides
- AOD-9604 -- HGH fragment targeting fat metabolism through beta-3 adrenergic receptor upregulation; different mechanism (lipolysis enhancement vs vascular ablation) with a far more favorable safety profile
- Semaglutide -- GLP-1 agonist with 15-17% weight loss in clinical trials; the standard of care for pharmacological weight management
- Tirzepatide -- Dual GIP/GLP-1 agonist with up to 22.5% weight loss; superior efficacy to semaglutide in head-to-head trials
- Retatrutide -- Triple agonist (GLP-1/GIP/glucagon) with up to 24.2% weight loss in Phase II; currently in Phase III trials
- Tesamorelin -- GHRH analog specifically targeting visceral fat reduction
- 5-Amino-1MQ -- NNMT inhibitor targeting fat metabolism through NAD+ pathway; oral bioavailability
- FOXO4-DRI -- Another pro-apoptotic peptide targeting senescent cells; shares the apoptosis-induction mechanism with Adipotide but targets different cell populations
- MOTS-C -- Mitochondrial-derived peptide for metabolic support and fat oxidation
Need the reconstitution math for Adipotide: Complete Research Guide?
Open the calculator with Adipotide: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.