AOD-9604: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- AOD 9604, Tyr-hGH fragment 177-191, HGH fragment 176-191, Fragment 177-191, Advanced Obesity Drug 9604
Attribute
Administration
- Detail
- Subcutaneous injection (primary); oral formulations exist but have significantly lower bioavailability
Attribute
Research Status
- Detail
- Research Compound — No FDA Approval. Phase IIb trials discontinued in 2007. FDA GRAS status as food ingredient (2019).
Attribute
Typical Dose Range
- Detail
- 200-500 mcg/day subcutaneous (most commonly cited: 300 mcg/day)
Attribute
Half-Life
- Detail
- ~4 minutes (plasma); metabolic effects may persist 12-24 hours
Attribute
Cycle Length
- Detail
- 8-16 weeks on, 4-6 weeks off
Attribute
Storage
- Detail
- Lyophilized: -20°C long-term; Reconstituted: 2-8°C, use within 4 weeks
Overview / What Is AOD-9604?
The Basics
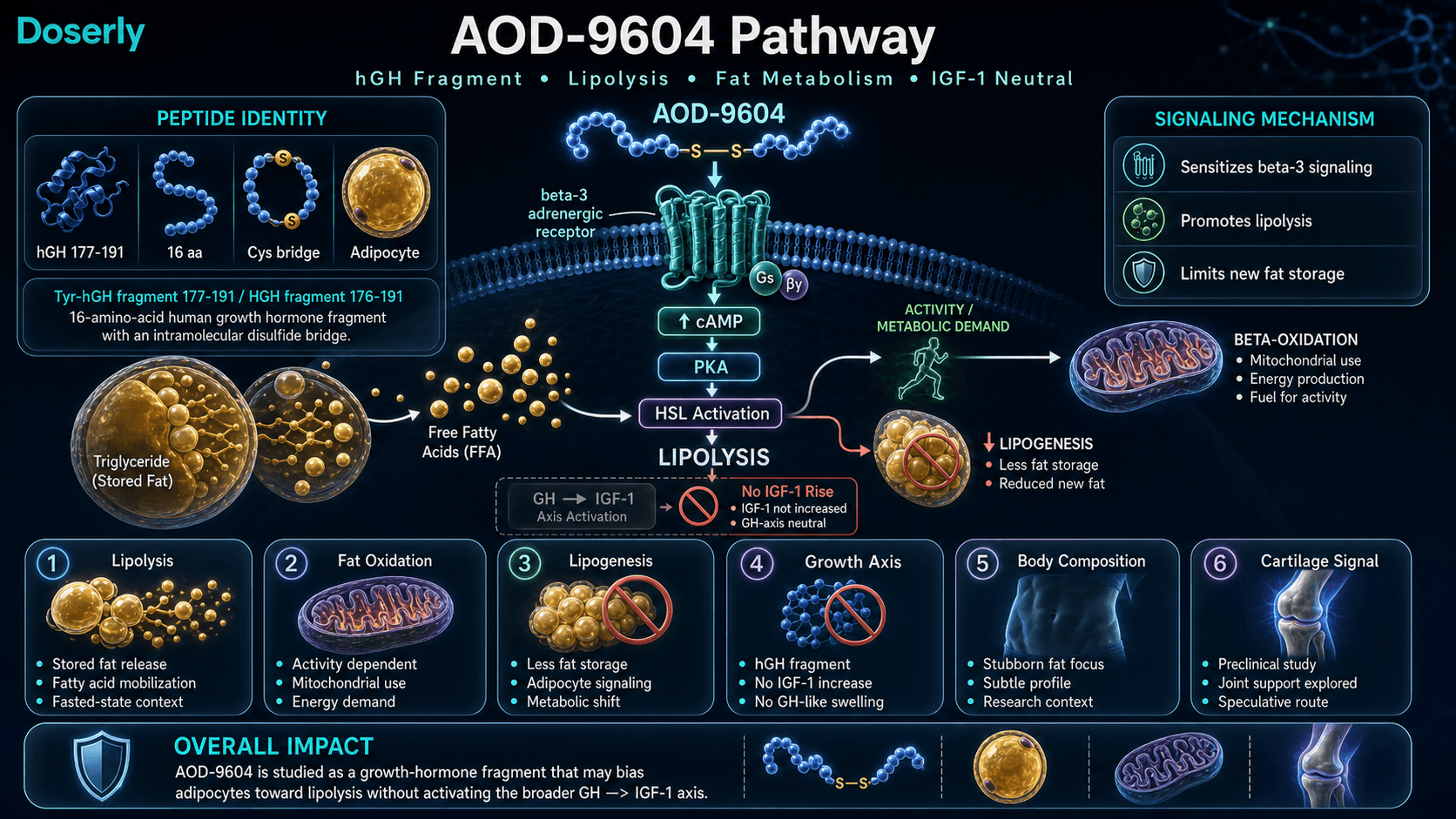
AOD-9604 is a small synthetic peptide designed to capture the fat-burning properties of human growth hormone (HGH) while leaving behind the side effects that make full-strength HGH problematic. The name stands for "Advanced Obesity Drug," and 9604 was its development code at Metabolic Pharmaceuticals in Australia during the 1990s.
Here is the core idea: growth hormone does many things in the body, including promoting tissue growth, elevating IGF-1 levels, and breaking down fat. Researchers found that the fat-burning action is concentrated in a small section at the tail end of the growth hormone molecule, specifically amino acids 177 through 191. AOD-9604 is that fragment, isolated and slightly modified with an extra tyrosine residue to make it stable and prevent it from triggering the growth-related effects of full HGH.
The result is a peptide that targets fat cells directly without raising IGF-1, without disrupting blood sugar, and without causing the water retention or joint problems associated with growth hormone therapy. That selectivity is both its appeal and its limitation. AOD-9604 went through clinical trials for obesity treatment in Australia but was discontinued in 2007 after producing only modest results (roughly 2% additional weight loss compared to placebo in severely obese patients). For obesity treatment, that effect size was insufficient. However, for individuals already near their target body composition who are looking for a marginal edge in stubborn fat areas, the equation may look different.
The Science
AOD-9604 (Tyr-hGH 177-191) is a synthetic hexadecapeptide comprising amino acids 177-191 of the C-terminal region of human growth hormone, with an N-terminal tyrosine substitution replacing the native phenylalanine at position 177 [1]. This modification was engineered to isolate the lipolytic activity of hGH from its somatotropic and diabetogenic properties.
The peptide was developed by Metabolic Pharmaceuticals Ltd in collaboration with Monash University (Melbourne, Australia) during the 1990s as part of a program to identify the minimal functional domain responsible for hGH's fat-metabolizing effects. Preclinical studies in obese Zucker rats demonstrated that AOD-9604 reduced body weight gain by approximately 25% compared to controls without inducing insulin resistance, as confirmed by euglycemic clamp testing [1]. Subsequent Phase IIb clinical trials enrolled approximately 836 subjects across multiple studies. A 12-week trial showed modest but statistically significant weight loss (2.6 kg vs 0.8 kg placebo at 1 mg/day oral dosing) [2]. However, a pivotal 24-week trial in 536 obese adults failed to demonstrate sufficient efficacy to meet regulatory thresholds, leading to discontinuation of pharmaceutical development in 2007 [2][3].
Despite the clinical failure as an obesity drug, AOD-9604 received FDA Generally Recognized As Safe (GRAS) status as a food ingredient in 2019, reflecting favorable toxicology data across the clinical program [4].
Molecular Identity
Attribute
Common Names
- Detail
- AOD-9604, AOD 9604, Tyr-hGH fragment 177-191, HGH fragment 176-191
Attribute
Amino Acid Sequence
- Detail
- Tyr-Leu-Arg-Ile-Val-Gln-Cys-Arg-Ser-Val-Glu-Gly-Ser-Cys-Gly-Phe (16 amino acids)
Attribute
Single-Letter Code
- Detail
- YLRIVQCRSVEGSCGF
Attribute
Molecular Formula
- Detail
- C78H123N23O23S2
Attribute
Molecular Weight
- Detail
- 1815.1 g/mol
Attribute
CAS Number
- Detail
- 221231-10-3 (primary); 386264-39-7 (alternative)
Attribute
PubChem CID
- Detail
- 71300630
Attribute
Disulfide Bridge
- Detail
- Cys7-Cys14 (intramolecular, constrained cyclic structure)
Attribute
Parent Protein
- Detail
- Human growth hormone (hGH); AOD-9604 comprises <10% of hGH molecular mass
Attribute
Structural Type
- Detail
- Linear peptide with intramolecular disulfide bond
Attribute
Appearance
- Detail
- White to off-white lyophilized powder
Attribute
Solubility
- Detail
- Poorly soluble in water; enhanced via acetate salt formulation
Attribute
Plasma Half-Life
- Detail
- ~4 minutes (rapid N-terminal truncation degradation)
Mechanism of Action
The Basics
AOD-9604 works by turning up the activity of specific receptors on fat cells called beta-3 adrenergic receptors. Think of these receptors as switches on the surface of fat cells that, when activated, tell the cell to start breaking down stored fat and releasing it into the bloodstream for use as energy.
In people who carry excess weight, these switches tend to become sluggish. AOD-9604 restores their sensitivity, essentially re-wiring fat cells to respond to the body's natural "burn fat" signals more effectively. At the same time, it reduces the ability of fat cells to store new fat, creating a two-pronged effect: more fat released, less fat stored.
There is one important caveat. Releasing fat into the bloodstream is only half the battle. Those fat molecules need to actually be burned for energy, which requires physical activity or at least some metabolic demand. Without it, the freed-up fat simply circles back and gets re-stored. This is why practitioners who work with AOD-9604 emphasize fasted-state administration followed by activity.
What makes AOD-9604 distinct from full growth hormone is what it does not do. It does not raise IGF-1 levels (the growth factor that drives tissue growth and raises cancer risk concerns), it does not affect blood sugar or insulin sensitivity, and it does not cause the water retention or joint swelling common with HGH. It targets fat metabolism through a separate pathway entirely.
The Science
AOD-9604 exerts its lipolytic effects primarily through upregulation of beta-3 adrenergic receptor (beta-3-AR) expression in white adipose tissue [5][6]. Chronic administration in obese mice restored beta-3-AR mRNA levels from obesity-suppressed baselines to near-lean levels, with corresponding increases in hormone-sensitive lipase (HSL) activity and glycerol release (a marker of triglyceride hydrolysis) [5].
The mechanistic dependence on beta-3-AR was conclusively demonstrated in a knockout study by Heffernan et al. (2001). When AOD-9604 was administered to beta-3-AR knockout mice, the chronic lipolytic effect was abolished, confirming beta-3-AR as the primary mediator of sustained fat reduction [6]. However, acute fat oxidation effects persisted in knockout animals, suggesting at least one additional, currently unidentified pathway contributes to short-term metabolic effects [6].
Downstream, beta-3-AR activation by AOD-9604 elevates intracellular cyclic adenosine monophosphate (cAMP), activating protein kinase A (PKA), which phosphorylates HSL and perilipin-1 on the lipid droplet surface. This cascade liberates free fatty acids (FFAs) and glycerol from stored triglycerides [5].
Simultaneously, AOD-9604 inhibits lipogenesis by reducing acetyl-CoA carboxylase activity, limiting the conversion of carbohydrate substrates into new fat stores [1]. This dual mechanism, enhanced lipolysis coupled with suppressed lipogenesis, differentiates it from interventions that address only one side of the fat balance equation.
Critically, AOD-9604 does not bind the growth hormone receptor (GHR) and does not activate the JAK2/STAT5 signaling pathway responsible for IGF-1 production, glucose dysregulation, and anabolic tissue growth [3][7]. This explains the placebo-like safety profile observed across six clinical trials involving approximately 900 human subjects [3].
Pathway Visualization Image
Pharmacokinetics
The Basics
AOD-9604 has an unusually short plasma half-life of about 4 minutes when measured by how quickly the intact peptide disappears from the blood. This sounds alarmingly brief, but it is somewhat misleading. While the peptide itself is broken down quickly by enzymes that clip amino acids from its ends, the downstream metabolic effects (the beta-3 receptor upregulation and the signals sent to fat cells) appear to persist for considerably longer, likely in the 12-24 hour range. This is why once-daily dosing protocols are standard even though the peptide itself is gone within minutes.
When injected subcutaneously, AOD-9604 is absorbed into the bloodstream and distributed primarily to adipose tissue, where its target receptors are located. The peptide degrades through a process called N-terminal truncation, where enzymes progressively clip off amino acids from one end. Its degradation products (-1aa, -2aa, through -6aa forms) have been characterized for anti-doping purposes.
Oral formulations of AOD-9604 have been studied in clinical trials, but bioavailability via the oral route is substantially lower than subcutaneous injection. The clinical trials that reached Phase IIb used oral dosing at 0.25-30 mg/day, which is orders of magnitude higher than the 200-500 mcg subcutaneous doses commonly reported by practitioners, reflecting the absorption differential.
The Science
AOD-9604 exhibits rapid plasma clearance with an estimated terminal half-life of approximately 4 minutes following intravenous administration [7]. Degradation proceeds through sequential N-terminal amino acid truncation, producing characterized metabolites including -1aa through -6aa fragments, which have been catalogued for WADA anti-doping detection purposes [7].
Preclinical pharmacokinetic studies in porcine models confirmed rapid oral degradation, which limits systemic exposure but paradoxically contributes to the favorable safety profile by reducing off-target tissue exposure [3]. Clinical oral dosing (0.25-30 mg/day) in Phase IIb trials reflects the low oral bioavailability relative to subcutaneous routes [2].
The disconnect between the short plasma half-life and the sustained metabolic effects likely reflects the mechanism of action: AOD-9604 induces transcriptional upregulation of beta-3-AR expression rather than simply binding as a transient agonist. Once receptor expression is upregulated, the lipolytic machinery remains enhanced until receptor turnover returns expression to baseline [5][6]. This distinction between pharmacokinetic half-life (peptide clearance) and pharmacodynamic duration (biological effect persistence) is analogous to other receptor-modulating peptides where the downstream signal outlasts the initiating molecule.
Research & Clinical Evidence
AOD-9604 and Fat Loss
The Basics
The fat loss story for AOD-9604 starts strong in the laboratory and gets complicated in humans. In animal studies, the results were encouraging: obese rats and mice treated with AOD-9604 showed meaningful reductions in body weight and fat mass without the blood sugar problems or insulin resistance that come with full growth hormone.
When testing moved to humans, results were more modest. A 12-week trial in about 300 obese participants showed that people taking AOD-9604 lost roughly triple the weight of those on placebo. That sounds impressive until you look at the actual numbers: about 2.6 kg of loss compared to 0.8 kg on placebo. In a later, larger study over 24 weeks, the difference between AOD-9604 and placebo narrowed further when participants followed a structured diet and exercise program, suggesting that much of the benefit may overlap with what lifestyle changes alone can achieve.
The company developing AOD-9604 discontinued it as a pharmaceutical weight loss drug after these results. For context, modern GLP-1 receptor agonists like semaglutide and tirzepatide produce 15-24% body weight reduction, making AOD-9604's roughly 2% effect look modest by comparison.
The Science
Ng et al. (2000) demonstrated that chronic oral administration of AOD-9604 at 500 mcg/kg/day in obese Zucker rats produced a >50% reduction in body weight gain compared to controls over 19 days, with increased adipose tissue lipolytic activity. Euglycemic clamp testing confirmed no impairment of insulin sensitivity [1].
Heffernan et al. (2001) showed that AOD-9604 increased in vivo fat oxidation in ob/ob mice, with plasma glycerol levels (a marker of fat breakdown) increasing by over 40%. Both hGH and AOD-9604 reduced weight gain, but AOD-9604 did so without the diabetogenic effects observed with full hGH [5].
In human trials, a 12-week randomized, double-blind, placebo-controlled trial in approximately 300 obese subjects demonstrated statistically significant weight loss at the 1 mg/day oral dose: 2.6 kg vs 0.8 kg placebo (p < 0.05) [2]. Notably, the rate of weight loss remained steady throughout the 12-week period, suggesting resistance to the compound is unlikely with continued administration [2].
A subsequent pivotal 24-week Phase IIb trial (n=536) tested oral doses of 0.25, 0.5, and 1 mg/day alongside structured lifestyle intervention. This trial failed to demonstrate clinically meaningful efficacy beyond lifestyle modification alone, leading to discontinuation of pharmaceutical development [2][3].
A separate short multiple-dose safety study evaluated oral doses of 9, 27, and 54 mg/day for 7 days in obese adults, confirming tolerability across a wide dose range [3].
AOD-9604 and Joint/Cartilage Health
The Basics
An unexpected finding from AOD-9604 research is its potential effect on cartilage and joint health. In a rabbit model of osteoarthritis, researchers injected AOD-9604 directly into affected joints and observed improvements in cartilage structure and reduced joint damage. The effect was enhanced when AOD-9604 was combined with hyaluronic acid, a common joint injection treatment.
This is an early-stage finding based on a single animal study, and the protocol used (direct injection into the joint) differs significantly from the subcutaneous fat-loss protocols most people associate with AOD-9604. Whether the joint benefits translate to humans, or whether subcutaneous dosing can produce similar effects at distant joint sites, remains unknown.
The Science
Kwon and Park (2015) evaluated intra-articular injection of AOD-9604, alone and in combination with hyaluronic acid (HA), in a collagenase-induced rabbit osteoarthritis model. The combination group demonstrated significant improvements in gross morphological appearance and microscopic cartilage structure compared to both control and AOD-9604-alone groups [8]. The study suggested that AOD-9604 may promote chondrocyte proliferation and extracellular matrix remodeling, though the mechanisms remain poorly characterized. No human studies have investigated AOD-9604 for joint health applications.
Biomarker Evidence Matrix
The table below scores AOD-9604 across relevant biomarker categories based on two dimensions: Evidence Strength (quality of research data) and Reported Effectiveness (community-reported outcomes from the Sentiment Analysis).
Category
Fat Loss
- Evidence Strength
- 5/10
- Reported Effectiveness
- 4/10
- Summary
- Strong preclinical data (animal studies) showing lipolysis enhancement, but human clinical trials showed only modest results (~2% vs placebo). Community reports are mixed, with many users reporting no noticeable difference beyond caloric deficit.
Category
Weight Management
- Evidence Strength
- 5/10
- Reported Effectiveness
- 3/10
- Summary
- Phase IIb clinical data exists but failed to meet efficacy thresholds. Community consensus positions AOD-9604 as the "mildest" fat loss peptide, far behind GLP-1 agonists.
Category
Joint Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Single rabbit OA study with intra-articular injection showed cartilage repair potential. No human data. Community reports mention joint benefits anecdotally but no specific user outcomes documented.
Category
Side Effect Burden
- Evidence Strength
- 8/10
- Reported Effectiveness
- 8/10
- Summary
- Six RCTs (~900 subjects) demonstrate placebo-like tolerability. No IGF-1 elevation, no glucose disruption, no antibody formation. Community unanimously reports excellent tolerance. Strongest signal for AOD-9604.
Category
Nausea & GI Tolerance
- Evidence Strength
- 7/10
- Reported Effectiveness
- 8/10
- Summary
- Clinical trials showed no meaningful GI adverse events vs placebo. Community confirms excellent GI tolerance, especially favorable compared to GLP-1 agonists.
Category
Appetite & Satiety
- Evidence Strength
- 3/10
- Reported Effectiveness
- 3/10
- Summary
- AOD-9604 does not appear to affect appetite pathways. Works through beta-3 receptors on fat cells, not through GLP-1 or other appetite signaling. No appetite effects reported by community.
Category
Energy Levels
- Evidence Strength
- 2/10
- Reported Effectiveness
- 4/10
- Summary
- No clinical data on energy effects. Community does not associate AOD-9604 with energy changes.
Category
Inflammation
- Evidence Strength
- 2/10
- Reported Effectiveness
- 4/10
- Summary
- No direct anti-inflammatory data. Does not worsen inflammatory markers.
Category
Treatment Adherence
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Daily injection protocol with fasting requirement creates moderate adherence burden. Some users report reconstitution challenges with certain vial sizes.
Categories not scored (insufficient data): Muscle Growth, Food Noise, Sleep Quality, Focus & Mental Clarity, Memory & Cognition, Mood & Wellbeing, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Pain Management, Recovery & Healing, Physical Performance, Gut Health, Digestive Comfort, Skin Health, Hair Health, Heart Health, Blood Pressure, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Fluid Retention, Body Image, Immune Function, Bone Health, Longevity & Neuroprotection, Cravings & Impulse Control, Social Connection, Daily Functioning, Withdrawal Symptoms, Other.
Benefits & Potential Effects
The Basics
AOD-9604's benefit profile is narrow but well-defined. Its primary application is as a supplementary tool for fat metabolism, specifically targeting the lipolysis side of the equation by signaling fat cells to release their stored contents. It is most commonly discussed in the context of stubborn fat areas that resist diet and exercise in individuals who are already relatively lean.
A secondary benefit that has generated interest is potential joint and cartilage support, based on a single preclinical study showing cartilage repair when injected directly into arthritic joints. This remains speculative for typical subcutaneous users.
Perhaps the most notable aspect of AOD-9604 is what it does not do. It does not raise IGF-1 levels, which means no concerns about growth factor-related risks. It does not disrupt blood sugar or insulin sensitivity. It does not cause the water retention, joint swelling, or carpal tunnel symptoms associated with growth hormone therapy. For individuals who want to avoid these issues while still accessing a compound that targets fat metabolism, that safety profile is the primary draw.
It is important to set realistic expectations. Based on both clinical trial data and community reports, AOD-9604 is not a primary fat loss tool. It occupies a marginal-benefit niche, best suited as a fine-tuning layer after nutrition, training, sleep, and potentially more potent compounds (GLP-1 agonists, tesamorelin) are already in place.
The Science
The demonstrated and proposed benefits of AOD-9604, based on available preclinical and clinical evidence:
Lipolysis Enhancement: AOD-9604 upregulates beta-3-AR expression and activates HSL-mediated triglyceride hydrolysis in adipose tissue [5][6]. Preclinical studies show preferential reduction of abdominal fat mass [1][5].
Lipogenesis Inhibition: The compound reduces new fat storage by inhibiting acetyl-CoA carboxylase activity, limiting de novo lipogenesis independently of caloric intake in animal models [1].
Metabolic Neutrality: Across six human trials involving ~900 subjects, AOD-9604 demonstrated no effect on IGF-1 levels, glucose tolerance (oral glucose tolerance test), insulin sensitivity, or HbA1c. No anti-AOD-9604 antibodies were detected [3].
Chondroprotective Potential: A single preclinical study in a rabbit osteoarthritis model showed intra-articular AOD-9604 improved cartilage morphology and enhanced the effects of hyaluronic acid co-administration [8]. The mechanism may involve stimulation of chondrocyte proliferation, though this pathway remains poorly characterized.
Cardiovascular Indirect Benefits: Some researchers have proposed that AOD-9604 may improve cardiovascular risk markers beyond its effects on adiposity, possibly through the same secondary pathway (independent of beta-3-AR) that contributes to acute fat oxidation effects observed in knockout mice [6]. This hypothesis remains unvalidated.
Side Effects & Safety Considerations
The Basics
If there is one area where AOD-9604 genuinely excels, it is safety. The clinical trial program involved roughly 900 people across six studies, and the side effect profile was essentially identical to placebo. This is not a case of side effects being "mild" or "manageable," they were statistically indistinguishable from taking nothing at all.
The most commonly reported issue is mild injection site reactions (slight redness or itching), which is common to virtually all subcutaneous peptides and typically resolves within minutes. Occasional headache and rare nausea have been reported, but at rates no higher than placebo groups.
What AOD-9604 does not cause is equally important. There is no IGF-1 elevation, which means no growth-factor-related concerns. Blood sugar and insulin function remain unaffected. There is no water retention or edema. There is no carpal tunnel or joint pain. There is no antibody formation (meaning your immune system does not learn to attack it). And there is no evidence of pituitary suppression, meaning it does not interfere with your body's own growth hormone production.
This safety profile is AOD-9604's most defensible characteristic and the primary reason practitioners continue to include it in protocols despite its modest efficacy data.
The Science
Stier et al. (2013) conducted a comprehensive safety analysis across six randomized, double-blind, placebo-controlled clinical trials of AOD-9604, spanning intravenous, oral, and subcutaneous administration routes [3]. Key findings:
- IGF-1: No significant changes from baseline or placebo at any dose level (0.25 mg to 54 mg/day) [3]
- Glucose Metabolism: Oral glucose tolerance testing (OGTT) showed no differences between AOD-9604 and placebo groups. Fasting glucose, insulin, and HbA1c were unaffected [3]
- Immunogenicity: No anti-AOD-9604 antibodies detected in any subject across all trials [3]
- Adverse Events: Incidence and severity of adverse events were comparable between active and placebo groups. No treatment-related serious adverse events were reported [3]
- Cardiovascular: No clinically significant changes in blood pressure or heart rate [3]
The FDA reviewed available toxicology and safety data and granted GRAS (Generally Recognized As Safe) status for AOD-9604 as a food ingredient in 2019 [4]. This determination, while not constituting therapeutic approval, reflects an independent regulatory assessment that the compound poses no safety concerns at food-ingredient exposure levels.
Nonclinical chronic oral toxicity studies in rats and monkeys showed no target organ toxicity at sustained dosing [3].
Side effect profiles are most useful when you can compare them against your own experience in real time. Doserly lets you log symptoms, severity, and timing alongside your dosing data, creating a side-by-side view of your protocol and your body's response.
This kind of systematic tracking catches things that memory alone misses. A subtle mood shift that began three days after a dose increase. Sleep disruption that correlates with evening administration. These patterns become visible when the data is laid out on a timeline, and they give your healthcare provider actionable information rather than vague concerns. Early detection of emerging side effects means earlier intervention.
Keep side effects, flags, and follow-up notes visible.
Doserly helps you document safety observations, side effects, medication changes, and follow-up questions so important context is not scattered.
Safety log
Flags and notes

Safety notes are not emergency guidance; seek medical help when appropriate.
Dosing Protocols
The Basics
Dosing information reported across sources shows broad agreement on the general approach, with some variation in specifics. The most commonly cited protocol involves subcutaneous injection once daily, taken in a fasted state, at doses ranging from 200 to 500 mcg per day.
Many practitioners describe a graduated approach: starting at a lower dose (200-300 mcg) for the first few weeks and increasing to 400-500 mcg if well tolerated. The typical cycle length ranges from 8 to 16 weeks, followed by a 4-6 week break.
One factor that nearly all sources emphasize is the importance of fasted administration. Because insulin suppresses lipolysis (fat breakdown), taking AOD-9604 after a meal, particularly one containing carbohydrates, may substantially reduce its effectiveness. Most protocols call for injection first thing in the morning, at least 30-60 minutes before eating. Some practitioners describe a split-dose approach (250 mcg morning, 250 mcg before bedtime, at least 1-4 hours after the last meal), though once-daily morning dosing is more common.
Commonly reported cycle structures range from 8 to 16 weeks of continuous daily dosing, followed by a rest period. Some sources suggest the break is less about biological necessity (since AOD-9604 does not affect hormonal axes) and more about honest assessment of whether the compound is producing noticeable results.
The Science
No standardized human dosing protocol exists for subcutaneous AOD-9604. Clinical trials evaluated oral administration at doses ranging from 0.25 mg to 30 mg/day, which are not directly comparable to subcutaneous dosing due to substantial differences in bioavailability [2][3].
Human Equivalent Dose (HED) translation from the efficacious rat model (0.5 mg/kg oral) using FDA body surface area scaling yields approximately 5.7 mg/day for a 70 kg human (oral), which falls within the range of the 12-week Phase IIb trial (1-30 mg/day) but above the 24-week trial doses (0.25-1 mg/day) [1].
Community-derived subcutaneous protocols (200-500 mcg/day) lack direct clinical trial equivalence. The pharmacological rationale for the lower subcutaneous doses rests on higher bioavailability relative to oral administration, though this ratio has not been formally quantified for AOD-9604 in human studies.
Weight-based dosing guidance circulating in practitioner communities suggests approximately 300 mcg/day for individuals under 160 lbs, 400 mcg/day for 160-200 lbs, and 500 mcg/day for individuals above 200 lbs, though these thresholds are not evidence-based [9].
The dosing protocols above involve numbers that matter: specific microgram amounts, reconstitution ratios, and timing windows. Getting any of these wrong compounds across every subsequent dose from that vial.
Doserly's dose and reconstitution calculators eliminate the guesswork. Enter your vial size, peptide amount, and target dose, and get the exact bacteriostatic water volume, units per tick mark, and doses per vial. The injection site tracker maps your administration history as a visual heat map across your body, flagging areas that need rest and suggesting rotation patterns. Combined with dose reminders that include compound name, amount, and route, every aspect of your daily protocol is handled with the precision it requires.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders

Reminder tracking supports consistency; it does not select a protocol for you.
What to Expect
AOD-9604 is frequently described as a compound with subtle, gradual effects. Based on the available clinical data and community reports, here is a general timeline of what practitioners commonly report.
Weeks 1-2: Most users report nothing noticeable during the initial period. Some may experience mild injection site reactions as they establish their protocol. This is normal and expected. AOD-9604 is not an appetite suppressant, so there is no "I forgot to eat" signal like GLP-1 agonists provide. The peptide is working at the cellular level, upregulating beta-3 receptor expression, but this process takes time to translate into visible changes.
Weeks 3-4: Some practitioners describe the first subtle signs of change around this point, particularly in users who are already at lower body fat percentages and pairing AOD-9604 with consistent fasted cardio. These changes are typically reported as slight improvements in definition or tape measurements rather than dramatic scale changes. For many users, however, weeks 3-4 still show no discernible difference.
Weeks 5-8: If AOD-9604 is going to produce noticeable results, this is typically when they emerge. Users who report positive outcomes describe gradual reduction in stubborn fat areas (lower abdomen, love handles, upper thighs) when combined with caloric deficit and regular activity. Changes are measured in fractions of inches rather than dramatic transformations.
Weeks 8-12+: Users who continue beyond 8 weeks generally report steady, incremental progress at the same modest rate. There is some evidence from the 12-week clinical trial that the rate of effect does not diminish with continued use, suggesting receptor desensitization is unlikely [2].
Setting Expectations: If no measurable change is apparent by week 4-6, many practitioners recommend reassessing whether the problem lies elsewhere (nutrition, training consistency, sleep, or the need for a higher-leverage compound). AOD-9604 is a marginal optimizer, and if the fundamentals are not in place, its small effect size will be undetectable.
Interaction Compatibility
Good With (Synergistic Compounds)
- Tesamorelin — Provides anabolic protection and muscle preservation that AOD-9604 lacks. Tesamorelin targets visceral fat specifically through GH-axis support, while AOD-9604 targets peripheral subcutaneous fat through beta-3-AR activation. Different mechanisms make them complementary. Tesamorelin taken in the evening; AOD-9604 in the morning.
- MOTS-C — Programs mitochondria to prefer fat as fuel (AMPK activation). When paired with AOD-9604's fat mobilization, MOTS-C helps ensure mobilized fatty acids are oxidized rather than re-stored.
- Semaglutide — GLP-1 agonist providing appetite suppression and primary fat-loss drive through a completely different mechanism (GIP/GLP-1 receptors). AOD-9604 adds a marginal lipolytic signal alongside. No interaction concerns.
- Tirzepatide — Dual GIP/GLP-1 agonist. Same complementary logic as semaglutide, with typically stronger weight loss outcomes.
- Retatrutide — Triple agonist (GLP-1/GIP/glucagon). Provides the primary fat loss drive. AOD-9604 can serve as an adjunct for stubborn areas once primary weight loss has plateaued.
- 5-Amino-1MQ — NNMT inhibitor targeting fat metabolism through an entirely different pathway (NAD+ preservation). Complementary mechanism with no known interaction.
- Ipamorelin + CJC-1295 — GH secretagogue combination for pulsatile growth hormone release. Can enhance body composition alongside AOD-9604, though some overlap exists in fat-metabolism effects.
- L-Carnitine (injectable) — Shuttles mobilized fatty acids into mitochondria for oxidation. Directly addresses the "mobilization without oxidation" limitation of AOD-9604.
Not Good With (Caution or Contraindication)
- Exogenous HGH — Redundant. AOD-9604 is the lipolytic fragment of HGH. Using both simultaneously is pharmacologically unnecessary and adds cost without clear incremental benefit. Full HGH also introduces the IGF-1 elevation and glucose disruption that AOD-9604 was designed to avoid.
- High-carbohydrate meals near administration — Insulin suppresses lipolysis. Carbohydrate intake shortly before or after AOD-9604 injection may substantially blunt its fat-mobilizing effect. This is a timing consideration, not a pharmacological contraindication.
Administration Guide
AOD-9604 is typically administered via subcutaneous injection. Practitioners report the following general practices:
Materials typically required:
- Insulin syringes (U-100, 29-31 gauge)
- Alcohol swabs
- Bacteriostatic water (for reconstitution)
- Sharps disposal container
Recommended reconstitution solution: Bacteriostatic water is the standard reconstitution solution for AOD-9604. Some suppliers provide glacial acetic acid (GA) water as an alternative for formulations prone to gelling, though bacteriostatic water remains more common.
Timing considerations: Fasted administration is consistently emphasized across sources. Most practitioners report morning injection, at least 30-60 minutes before the first meal. The rationale is that insulin, released in response to food (particularly carbohydrates), suppresses the lipolytic cascade that AOD-9604 initiates. Some protocols describe a second daily dose taken 1-4 hours after the last meal before bedtime, though once-daily morning dosing is more commonly reported.
AOD-9604 is ideally paired with activity following injection. Zone-2 cardio or moderate exercise within 30-90 minutes after administration provides the metabolic demand needed to oxidize the fatty acids that AOD-9604 mobilizes from adipocytes.
Post-administration care: Monitor for mild injection site reactions (redness, slight itching), which typically resolve within minutes. No specific blood work monitoring is required for AOD-9604, as it does not affect IGF-1, glucose metabolism, or hormonal axes. However, general health monitoring (weight, waist circumference, fasting glucose, lipids) is prudent when pursuing any fat-loss protocol.
Supplies & Planning
The following materials are generally associated with AOD-9604 subcutaneous protocols:
Peptide vials: AOD-9604 is commonly available in 2 mg, 5 mg, and 10 mg vial sizes. The appropriate vial size depends on the target dose, as each reconstituted vial has a limited use window (typically 3-4 weeks refrigerated).
Reconstitution solution: Bacteriostatic water, typically in 10 mL bottles. The volume added to the vial determines the concentration and the number of units per tick mark on the syringe. Common reconstitution volumes are 2-3 mL per vial. Consult the reconstitution calculator for exact volumes based on your vial size and target dose.
Syringes: U-100 insulin syringes (29-31 gauge) for subcutaneous injection. One syringe per injection; never reuse syringes.
Alcohol swabs: For cleaning the vial stopper and injection site before each administration.
Sharps container: For safe disposal of used syringes and needles.
Storage equipment: A dedicated section of a refrigerator for reconstituted vials. Lyophilized (powder) vials can be stored frozen (-20°C).
Consult with a healthcare provider for specific quantities and protocol planning.
Storage & Handling
Lyophilized (powder) form:
- Store at -20°C (-4°F) in dry, dark conditions for long-term storage (stable for 1+ year)
- Short-term storage at 2-8°C (35.6-46.4°F) is acceptable for weeks to months
- Keep in sealed packaging with desiccant to minimize moisture exposure
- Allow vials to reach room temperature (10-30 minutes) before opening to prevent condensation
Reconstituted (liquid) form:
- Refrigerate immediately at 2-8°C (35.6-46.4°F) after reconstitution
- Use within 3-4 weeks (28 days) for optimal potency
- Do NOT freeze reconstituted solutions (freezing denatures peptides)
- Avoid repeated freeze-thaw cycles
- Protect from light by wrapping vials in foil or storing in opaque containers
Handling best practices:
- Swab vial stopper with alcohol before each draw
- Use sterile syringes for each draw
- Gently swirl or roll to dissolve during reconstitution; do not shake
- Inject bacteriostatic water slowly down the vial wall to avoid foaming
- Inspect reconstituted solution before each use; discard if cloudy, discolored, or contains particles
Lifestyle Factors
The lifestyle context around AOD-9604 is arguably more important than the compound itself. Because its fat-loss effect size is modest, the surrounding habits determine whether its contribution is detectable or lost in the noise.
Nutrition: Practitioners consistently emphasize that AOD-9604 is best viewed as a supportive aid within a calorie-controlled, protein-forward diet, not a replacement for nutritional discipline. A hypocaloric diet creates the metabolic demand (energy deficit) that drives oxidation of the fatty acids AOD-9604 mobilizes. Without that deficit, mobilized fat simply recirculates and is re-stored. Protein intake is important for preserving lean mass during any fat-loss phase, particularly since AOD-9604 itself provides no muscle-sparing effect.
Exercise: Both resistance training and aerobic activity complement AOD-9604's mechanism. Aerobic activity (especially fasted Zone-2 cardio performed 30-60 minutes after morning AOD-9604 injection) provides immediate oxidative demand for mobilized fatty acids. Resistance training 3-4 times per week supports muscle preservation and overall metabolic rate.
Sleep: 7-9 hours of quality sleep supports metabolic homeostasis and hormonal regulation. While AOD-9604 itself does not affect sleep, inadequate rest can impair fat metabolism through cortisol elevation and insulin sensitivity changes that work against the peptide's mechanism.
Fasting timing: The requirement for fasted-state administration adds a structural element to daily routine. Most protocols involve injection immediately upon waking, followed by 30-60 minutes before eating. This timing doubles as an opportunity for fasted cardio if applicable.
Stress management: Chronic stress elevates cortisol, which promotes visceral fat storage and can counteract lipolytic signaling. While AOD-9604 does not directly interact with the stress axis, practitioners report that stress management practices improve overall protocol outcomes.
The lifestyle factors above, nutrition, exercise, sleep, stress management, are not just nice-to-haves alongside a peptide protocol. They're force multipliers. Doserly lets you track these inputs alongside your compounds, building a complete picture of what your body is receiving and how it's responding.
When everything lives in one dashboard, patterns emerge. You can see whether training days correlate with better biomarker trends, whether your sleep scores predict next-day recovery quality, or whether stress spikes derail your progress in measurable ways. This kind of integrated tracking turns the lifestyle recommendations in this section from abstract advice into actionable, personalized insight.
Keep sensitive protocol records in a purpose-built app.
Doserly is designed for private health tracking with structured records, offline-ready workflows, and exportable history when you need it.
Privacy
Health records
Privacy controls help you manage records; keep clinical records where required.
Regulatory Status & Research Classification
United States (FDA): AOD-9604 is not approved by the FDA for any therapeutic indication. It received GRAS (Generally Recognized As Safe) status as a food ingredient in 2019. It is currently classified as a research compound and is available through research chemical suppliers and compounding pharmacies. The FDA Pharmacy Compounding Advisory Committee reviewed AOD-9604 as a bulk drug substance in 2024 [4].
Australia (TGA): AOD-9604 was originally developed in Australia by Metabolic Pharmaceuticals Ltd. It received regulatory attention during its Phase IIb clinical trial program but was not approved following trial discontinuation in 2007. The compound has been referenced under the brand name Aegerine in some regulatory contexts.
Canada (Health Canada): No DIN or NPN issued. AOD-9604 is not approved for therapeutic use.
United Kingdom (MHRA): Not approved for therapeutic use. Available as a research compound.
European Union (EMA): No marketing authorization. AOD-9604 has not been submitted for EMA review.
WADA Status: AOD-9604 is prohibited by the World Anti-Doping Agency (WADA) under category S2: Peptide Hormones, Growth Factors, Related Substances, and Mimetics [7]. Athletes subject to drug testing should avoid AOD-9604 regardless of its lack of significant performance-enhancing properties. Detection methods have been developed for anti-doping purposes [7].
Active Clinical Trials: No active registered clinical trials for AOD-9604 as of early 2026. All clinical development was discontinued in 2007.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is AOD-9604 and how is it different from growth hormone?
AOD-9604 is a synthetic fragment of human growth hormone, comprising amino acids 177-191 from the tail end of the HGH molecule. It was designed to isolate the fat-metabolizing properties of growth hormone while excluding the growth-promoting, IGF-1-elevating, and glucose-disrupting effects. Unlike full HGH, AOD-9604 does not elevate IGF-1 levels, does not affect blood sugar, and does not cause water retention or joint problems.
How effective is AOD-9604 for fat loss?
Based on available research data, AOD-9604 produced approximately 2% additional body weight reduction compared to placebo in the largest clinical trial (534 obese adults over 24 weeks). This effect was considered insufficient for pharmaceutical approval. Community reports are mixed, with many users reporting no noticeable difference beyond what diet and exercise alone would produce. Some practitioners report that the compound may be more effective for individuals who are already relatively lean and targeting stubborn fat areas, though this population has not been studied in controlled trials.
What is the typical dosing protocol that sources describe?
Commonly reported ranges in the literature and practitioner communities are 200-500 mcg per day via subcutaneous injection, with 300 mcg being the most frequently cited starting dose. Most sources emphasize fasted-state administration in the morning, at least 30-60 minutes before eating. Typical cycle lengths range from 8-16 weeks followed by a 4-6 week break. Readers should consult a qualified healthcare professional for any dosing decisions.
Does AOD-9604 have side effects?
Clinical trial data across approximately 900 subjects in six randomized, controlled trials showed a side effect profile indistinguishable from placebo. No IGF-1 elevation, glucose disruption, antibody formation, or treatment-related serious adverse events were reported. Mild injection site reactions and occasional headache have been reported but at rates comparable to placebo.
Can AOD-9604 be taken orally?
AOD-9604 was tested orally in clinical trials at doses of 0.25-30 mg/day. Oral bioavailability is substantially lower than subcutaneous injection, which is why clinical trial oral doses were orders of magnitude higher than the subcutaneous doses commonly reported by practitioners (200-500 mcg). Some oral and sublingual formulations are commercially available, but their bioavailability compared to injection is significantly reduced.
Is AOD-9604 banned in sports?
Yes. AOD-9604 is prohibited by WADA under category S2 (Peptide Hormones, Growth Factors, Related Substances, and Mimetics). Athletes subject to drug testing should avoid it entirely.
Can AOD-9604 be combined with GLP-1 medications?
Based on available data, AOD-9604 works through beta-3 adrenergic receptors on fat cells, while GLP-1 agonists work through GIP/GLP-1 receptors in the gut and brain. These are entirely different mechanisms with no known pharmacological interaction. Some practitioners describe using AOD-9604 as an adjunct to GLP-1 therapy for targeting stubborn fat areas. Readers should discuss any compound combination with their healthcare provider.
How long until results are noticeable?
Community reports suggest that if AOD-9604 is going to produce detectable results, they typically emerge around weeks 4-8 of consistent use, paired with a caloric deficit and regular activity. Results are generally described as subtle and gradual. Many practitioners suggest that if no measurable change is apparent by week 4-6, the issue may lie elsewhere in the overall protocol.
Sources & References
- Ng FM, Sun J, Sharma L, Libinaka R, Jiang WJ, Gianello R. Metabolic studies of a synthetic lipolytic domain (AOD9604) of human growth hormone. Hormone Research. 2000;53(6):274-278. PubMed: 11146367
- Wilding J. AOD-9604 Metabolic. Current Opinion in Investigational Drugs. 2004;5(4):431-437. PubMed: 15134286
- Stier H, Vos E, Kenley D. Safety and Tolerability of the Hexadecapeptide AOD9604 in Humans. Journal of Endocrinology and Metabolism. 2013;3(1-2):7-15. PubMed: 24078711
- FDA GRAS Notice GRN 000775. AOD-9604. U.S. Food and Drug Administration. 2019.
- Heffernan MA, Thorburn AW, Fam B, et al. Increase of fat oxidation and weight loss in obese mice caused by chronic treatment with human growth hormone or a modified C-terminal fragment. International Journal of Obesity. 2001;25(10):1442-1449. PubMed: 11673763
- Heffernan M, Summers RJ, Thorburn A, et al. The effects of human GH and its lipolytic fragment (AOD9604) on lipid metabolism following chronic treatment in obese mice and beta(3)-AR knock-out mice. Endocrinology. 2001;142(12):5182-5189. PubMed: 11713213
- Cox HD, Rampton J, Eichner D. Detection and in vitro metabolism of AOD9604. Drug Testing and Analysis. 2015;7(1):31-38. PubMed: 25208511
- Kwon DR, Park GY. Effect of Intra-articular Injection of AOD9604 with or without Hyaluronic Acid in Rabbit Osteoarthritis Model. Annals of Clinical and Laboratory Science. 2015;45(4):426-432. PubMed: 26275694
- Valentino MA, Lin JE, Snook AE, et al. Central and Peripheral Molecular Targets for Anti-Obesity Pharmacotherapy. Clinical Pharmacology and Therapeutics. 2010;87(6):652-662. PMC: PMC3136748
Related Peptide Guides
- Tesamorelin — GHRH analog for visceral fat reduction and GH-axis support; complementary to AOD-9604 for body composition optimization
- MOTS-C — Mitochondrial-derived peptide for metabolic support and fat oxidation; pairs with AOD-9604 in the morning partition stack
- Semaglutide — GLP-1 agonist for primary fat loss and appetite suppression; higher-leverage compound compared to AOD-9604
- Tirzepatide — Dual GIP/GLP-1 agonist with strongest clinical weight loss data; AOD-9604 used as adjunct
- Retatrutide — Triple agonist (GLP-1/GIP/glucagon) in clinical trials; primary fat-loss driver
- 5-Amino-1MQ — NNMT inhibitor targeting fat metabolism through NAD+ pathway; different mechanism, complementary
- Ipamorelin — GH secretagogue for pulsatile growth hormone release and body composition
- CJC-1295 — GHRH analog often combined with ipamorelin for GH optimization
- MK-677 — Oral GH secretagogue; alternative approach to GH-axis modulation
- BPC-157 — Healing peptide sometimes combined in broader wellness protocols
Need the reconstitution math for AOD-9604: Complete Research Guide?
Open the calculator with AOD-9604: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.