NAD+: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Nicotinamide Adenine Dinucleotide, beta-NAD+, Coenzyme I, Diphosphopyridine Nucleotide (DPN), NAD
Attribute
Administration
- Detail
- Injectable (Subcutaneous, Intramuscular, Intravenous); Oral precursors (NMN, NR) available as supplements
Attribute
Research Status
- Detail
- Not a peptide. Naturally occurring coenzyme. NAD+ precursors (NMN, NR) sold as dietary supplements. Injectable NAD+ available through compounding pharmacies. No FDA-approved injectable therapeutic indication.
Attribute
Typical Dose Range
- Detail
- 50-100 mg/day subcutaneous (wellness); 100-300 mg IM (stacking protocols); 500-1,000 mg IV (clinical/addiction settings)
Attribute
Half-Life
- Detail
- Rapid plasma clearance (minutes); biological activity duration estimated at several hours; tissue-level effects persist longer
Attribute
Cycle Length
- Detail
- 8-16 weeks subcutaneous; continuous use reported in some protocols
Attribute
Storage
- Detail
- Lyophilized: -20C or below (-80C ideal); Reconstituted: 2-8C for up to 14 days; Extremely hygroscopic; protect from light
Overview / What Is NAD+?
The Basics
NAD+ stands for Nicotinamide Adenine Dinucleotide, and it is one of the most important molecules in your body. It is found in every living cell and acts as a helper molecule for hundreds of biological processes. Its two most critical jobs are helping your cells produce energy and supporting the repair of damaged DNA.
Here is the key concept: NAD+ is not a peptide. It is a coenzyme, a small molecule that enzymes need to do their work. It shows up in peptide guides and biohacking communities because injectable NAD+ has become popular alongside peptide protocols, and the people researching peptides are often the same people interested in NAD+. But it works differently from peptides, and understanding that distinction matters.
Your body makes NAD+ naturally, but levels decline as you age. By age 50, most people have roughly half the NAD+ they had at 20. This decline is one of the most consistent and well-documented features of cellular aging, which is why NAD+ has become a central focus in longevity research. The theory is straightforward: if falling NAD+ levels contribute to aging and disease, then restoring those levels might slow or partially reverse some of those processes.
There are several ways to boost NAD+ levels. Oral supplements like NMN (nicotinamide mononucleotide) and NR (nicotinamide riboside) are precursors that your body converts into NAD+. Injectable NAD+ bypasses the digestive system entirely, delivering the molecule directly into circulation. Each approach has trade-offs in terms of cost, convenience, and how quickly levels rise.
The Science
NAD+ (Nicotinamide Adenine Dinucleotide; CAS 53-84-9) is a dinucleotide coenzyme with a molecular weight of 664.43 Da, composed of two nucleotide subunits (nicotinamide mononucleotide and adenosine mononucleotide) linked by a pyrophosphate bridge. It exists in oxidized (NAD+) and reduced (NADH) forms, cycling between these states as it transfers electrons in metabolic reactions [1].
NAD+ participates in over 500 enzymatic reactions, serving as an essential cofactor in glycolysis, the tricarboxylic acid (TCA) cycle, and oxidative phosphorylation. Beyond its role as an electron carrier, NAD+ functions as a consumed substrate for three major enzyme families: sirtuins (SIRT1-7), which regulate gene expression, DNA repair, and metabolic flexibility; poly(ADP-ribose) polymerases (PARPs), which detect and repair DNA strand breaks; and CD38/CD157, ectoenzymes that hydrolyze NAD+ to produce signaling metabolites [2][3].
The age-related decline in NAD+ levels is driven by multiple factors, including increased CD38 expression on immune cells (particularly macrophages), elevated PARP activity in response to accumulated DNA damage, and reduced activity of NAMPT (nicotinamide phosphoribosyltransferase), the rate-limiting enzyme in the NAD+ salvage pathway [4]. This decline has been quantified at approximately 50% between ages 20 and 50 in human tissue studies, with faster depletion under conditions of chronic stress, inflammation, and metabolic dysfunction [5].
Molecular Identity
Attribute
Chemical Name
- Detail
- Nicotinamide Adenine Dinucleotide
Attribute
Molecular Formula
- Detail
- C21H27N7O14P2
Attribute
Molecular Weight
- Detail
- 664.43 Da
Attribute
CAS Number
- Detail
- 53-84-9 (NAD+); 58-68-4 (NADH)
Attribute
PubChem CID
- Detail
- 5892 (NAD+); 6392 (NADH)
Attribute
Structure Type
- Detail
- Dinucleotide (two nucleotide subunits linked by pyrophosphate bridge)
Attribute
Redox Forms
- Detail
- Oxidized (NAD+, yellow-white) / Reduced (NADH, white, fluorescent)
Attribute
Solubility
- Detail
- Highly soluble in water (~300 mg/mL)
Attribute
Stability
- Detail
- Stable at physiological pH; degrades above 50C; extremely hygroscopic
Mechanism of Action
The Basics
Think of NAD+ as the universal energy currency your cells use to power almost everything they do. Your mitochondria (the energy factories inside each cell) need NAD+ to convert the food you eat into usable energy called ATP. Without enough NAD+, the conversion slows down and your cells produce less energy, which you experience as fatigue, brain fog, and slower recovery.
But NAD+ does more than just fuel energy production. It also activates a family of proteins called sirtuins, which act like maintenance crews for your cells. Sirtuins repair damaged DNA, regulate inflammation, and help your metabolism stay flexible. They are the same proteins linked to the life-extending benefits of calorie restriction. The catch is that sirtuins need NAD+ to function. When NAD+ drops, sirtuin activity drops with it, and cellular maintenance falls behind.
There is a third critical role: NAD+ is consumed by PARP enzymes, which detect and fix breaks in your DNA. Every time a PARP enzyme fixes a DNA break, it uses up NAD+ in the process. Under conditions of chronic stress or inflammation, PARP activity increases and burns through NAD+ faster than your body can replace it, creating a deficit that affects both energy production and DNA repair simultaneously.
Finally, an enzyme called CD38 actively destroys NAD+. CD38 levels increase with age and inflammation, which is one reason NAD+ declines so consistently as people get older. Some researchers describe this as a "NAD+ drain" that accelerates aging from within.
The Science
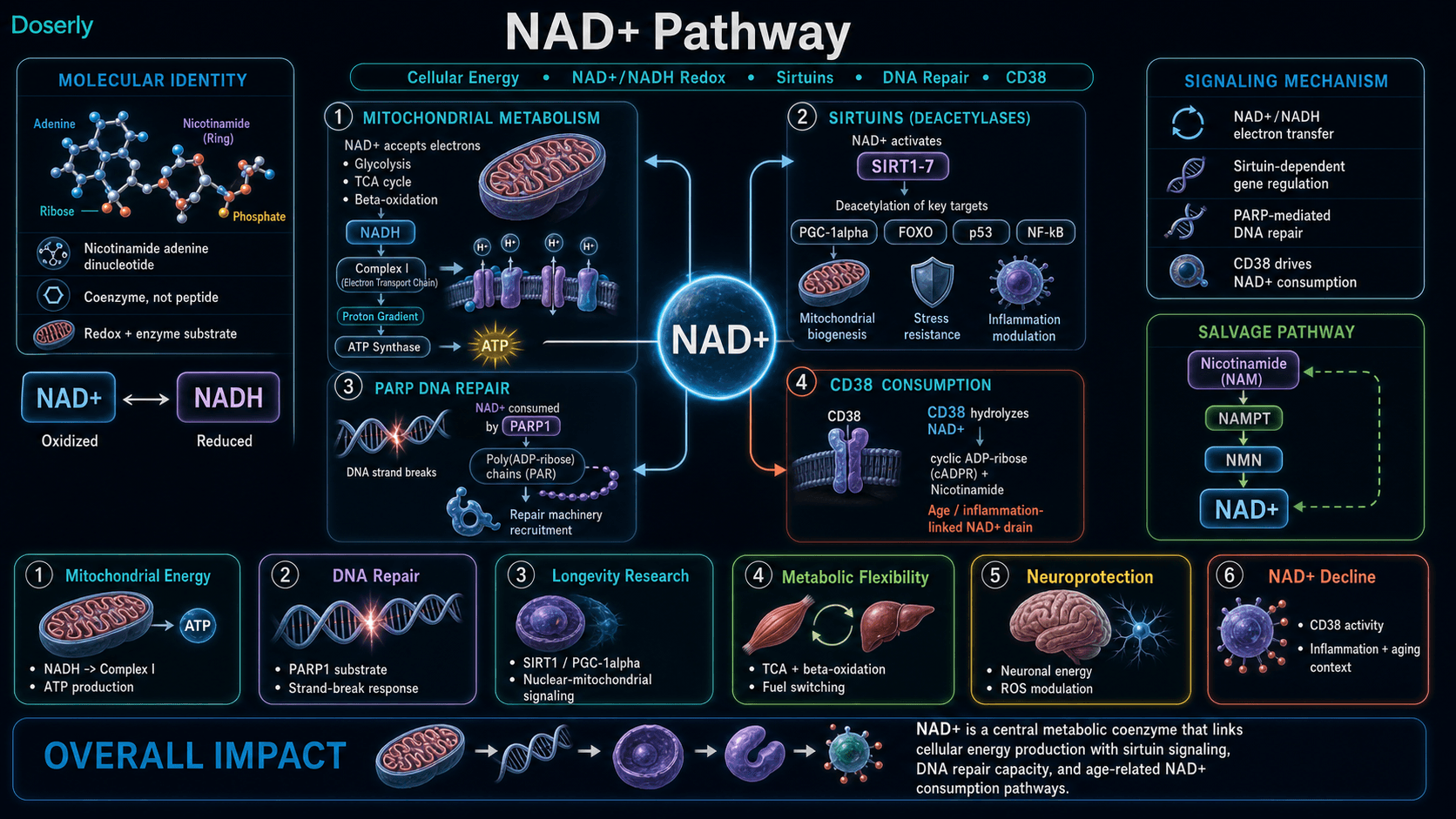
NAD+ exerts its biological effects through four primary functional roles:
1. Electron Carrier in Oxidative Metabolism
NAD+ accepts electrons from substrates during glycolysis, fatty acid beta-oxidation, and the TCA cycle, forming NADH. NADH then donates these electrons to Complex I (NADH dehydrogenase) of the mitochondrial electron transport chain, driving the proton gradient that powers ATP synthase. The NAD+/NADH ratio is a critical determinant of metabolic flux, with a high ratio favoring oxidative/catabolic pathways [1][6].
2. Sirtuin Activation
Sirtuins (SIRT1-7) are NAD+-dependent deacetylases and ADP-ribosyltransferases that regulate gene expression, DNA repair, mitochondrial biogenesis, and inflammatory responses. SIRT1, the most studied family member, deacetylates key transcription factors including PGC-1alpha (mitochondrial biogenesis), p53 (apoptosis), NF-kB (inflammation), and FOXO proteins (stress resistance). Sirtuin activity is directly limited by NAD+ availability, establishing a mechanistic link between NAD+ decline and age-related metabolic dysfunction [2][3].
3. DNA Repair via PARPs
Poly(ADP-ribose) polymerases (PARPs), particularly PARP1, consume NAD+ to synthesize poly(ADP-ribose) chains at sites of DNA strand breaks, recruiting repair machinery. Under conditions of chronic DNA damage (aging, oxidative stress, inflammation), PARP hyperactivation can deplete cellular NAD+ pools, creating competition between DNA repair and sirtuin-mediated metabolic regulation. This PARP-sirtuin competition for NAD+ is a proposed mechanism linking DNA damage to metabolic decline in aging [7].
4. CD38-Mediated NAD+ Consumption
CD38 is an ectoenzyme expressed on immune cells (particularly macrophages) that catalyzes the hydrolysis of NAD+ to produce cyclic ADP-ribose and nicotinamide. CD38 expression increases with age and inflammation, and has been identified as a primary driver of age-related NAD+ decline. Inhibition of CD38 (pharmacologically or through compounds like apigenin) has been shown to restore NAD+ levels in aged mouse models [4][8].
The interplay between these four pathways creates a reinforcing cycle: age-related inflammation increases CD38 activity, which depletes NAD+, which reduces sirtuin-mediated anti-inflammatory signaling, which further increases inflammation. Breaking this cycle through NAD+ repletion is the theoretical basis for therapeutic intervention [5].
Pathway Visualization Image
Pharmacokinetics
The Basics
NAD+ behaves differently from most compounds discussed in peptide guides. When administered intravenously, it is cleared from the bloodstream very quickly, within minutes. However, its biological effects last considerably longer because NAD+ is rapidly taken up by cells and metabolized into downstream products that continue working for hours.
This rapid clearance is why IV infusions are given slowly (often over several hours) and why subcutaneous injections create a slower, more sustained release compared to IV. Subcutaneous injection deposits NAD+ into fatty tissue, where it absorbs gradually into the bloodstream rather than arriving all at once.
One important detail: a significant portion of administered NAD+ is excreted through the kidneys. A pilot study found that much of a 750 mg IV dose appeared as metabolites in the urine, suggesting the body processes exogenous NAD+ extensively rather than simply storing it. This rapid metabolism is why repeated dosing (daily or several times per week) is the norm in most protocols rather than single large doses.
The distinction between plasma half-life and biological effect duration matters for dosing decisions. NAD+ disappears from the blood quickly, but the downstream effects on sirtuin activation, DNA repair, and mitochondrial function persist well beyond the point when the molecule itself is no longer detectable.
The Science
Pharmacokinetic data for exogenous NAD+ in humans remains limited, with most evidence derived from a single pilot metabolic study and extrapolation from precursor (NMN, NR) pharmacokinetics.
A pilot study administering 750 mg NAD+ as a continuous IV infusion over 6 hours in healthy volunteers demonstrated rapid metabolic handling with significant urinary excretion of NAD+-related metabolites. Plasma appearance of downstream metabolites was delayed relative to infusion timing, suggesting tissue uptake and processing precede systemic recirculation [9].
Subcutaneous administration creates depot-like absorption with more inter-subject variability influenced by temperature and adiposity. Intramuscular injection provides faster, less variable uptake than subcutaneous due to greater muscle perfusion. IM generally tolerates larger volumes (1-3 mL) compared to SC (0.3-1 mL) and may cause more injection soreness, while SC may cause more local irritation and erythema [10].
NAD+ is not a conventional drug with a simple plasma half-life. It functions as a metabolic substrate that is rapidly consumed by enzymatic pathways (sirtuins, PARPs, CD38) upon cellular uptake. The relevant pharmacokinetic parameter is not how long NAD+ persists in plasma, but how long its replenishment of intracellular NAD+ pools sustains elevated enzymatic activity.
Research & Clinical Evidence
NAD+ and Aging / Longevity
The Basics
The connection between NAD+ and aging is one of the most actively researched areas in longevity science. The basic finding is consistent across many studies: NAD+ levels drop with age, and restoring those levels in animal models reverses some markers of aging. Mice given NAD+ or its precursors show improved mitochondrial function, better muscle performance, healthier blood vessels, and markers of cellular rejuvenation.
The Harvard researcher David Sinclair brought this concept to mainstream attention in 2013 when his lab demonstrated that NAD+ supplementation could restore mitochondrial function in aged mouse muscle to a more youthful state. The key insight was that declining NAD+ creates a communication breakdown between the cell's nucleus and its mitochondria, and that this breakdown is reversible with intervention.
However, translating these results to humans has been slower. Multiple human trials with NAD+ precursors (NMN and NR) confirm that supplementation does increase NAD+ levels in blood and tissue. Whether those increased levels translate to the dramatic rejuvenation seen in mice remains an open question. Early human data is encouraging but preliminary.
The Science
Gomes et al. (2013) demonstrated that declining NAD+ induces a pseudohypoxic state in aged mouse cells, disrupting nuclear-mitochondrial communication through reduced SIRT1 activity and consequent loss of PGC-1alpha-mediated mitochondrial gene expression. This dysfunction was reversible with NAD+ repletion within one week of treatment [11].
Subsequent studies established a two-phase model of age-related muscle decline: Phase 1 involves reduced oxidative phosphorylation from decreased mitochondrial gene expression (reversible with NAD+); Phase 2 involves malfunctioning genes in both mitochondria and nucleus (refractory to NAD+ intervention). This suggests a critical window for intervention before irreversible dysfunction develops [12].
A systematic review of NAD+ precursor supplementation in humans (2023) across multiple randomized trials found consistent increases in blood NAD+ levels, with evidence of improved exercise performance, enhanced insulin sensitivity, and reduced inflammatory markers in middle-aged and older adults [13]. A meta-analysis of glucose and lipid metabolism outcomes found significant reductions in triglycerides and increases in HDL cholesterol with niacin-based NAD+ enhancement [14].
NAD+ and Neuroprotection
The Basics
Research into NAD+ and brain health is growing, particularly around neurodegenerative conditions like Parkinson's and Alzheimer's diseases. The brain is one of the most energy-demanding organs, and neurons are especially vulnerable when cellular energy production falters. NAD+ supports brain health in two ways: by keeping mitochondria running efficiently in neurons, and by reducing the buildup of damaging free radicals.
Some researchers are exploring whether NAD+ supplementation could work alongside PARP inhibitors (a class of cancer drugs) to protect neurons. The rationale is that overactive PARP enzymes consume too much NAD+, potentially contributing to the death of dopamine-producing neurons in Parkinson's disease. Early animal studies suggest NAD+ supplementation may help preserve these neurons.
The Science
NAD+ demonstrates neuroprotective effects in multiple preclinical models. Shan et al. (2019) showed that beta-nicotinamide adenine dinucleotide protected against motor deficits and dopaminergic neuronal damage in a mouse model of Parkinson's disease [15]. The mechanism involves improved mitochondrial function, decreased reactive oxygen species production, and modulation of the kynurenine pathway (KP), which links tryptophan metabolism to neuroinflammation [16].
KP dysregulation has been implicated in Parkinson's, Alzheimer's, and Huntington's diseases, as well as psychiatric disorders including schizophrenia and bipolar disorder. Because NAD+ de novo synthesis via the KP consumes tryptophan (a neurotransmitter precursor), exogenous NAD+ supplementation may spare tryptophan for serotonin and other neurotransmitter synthesis [16][17].
A 2021 review of both basic research and clinical trials of NAD+ in Parkinson's disease found consistent neuroprotective signals in animal models, with two registered human clinical trials underway but no definitive human efficacy data published at that time [18].
NAD+ and Metabolic Health
The Basics
NAD+ plays a direct role in how your body processes sugar and fat. When NAD+ levels are adequate, cells can efficiently convert both glucose and fatty acids into energy. When levels drop, this conversion becomes less efficient, contributing to insulin resistance, weight gain, and metabolic dysfunction.
Research in mice has shown that NAD+ supplementation improves insulin sensitivity, increases metabolic rate, and promotes lean body mass. In humans, NAD+ precursor supplementation has shown improvements in glucose and lipid metabolism, though the effects are more modest than what is seen in animal models.
The Science
Adipose tissue NAD+ biology plays a central role in obesity-driven insulin resistance. Obesity leads to inflammation and NAMPT suppression, reducing NAD+ availability in fat tissue. This triggers a cascade: reduced adiponectin signaling, increased hepatic gluconeogenesis, and impaired insulin-mediated glucose uptake in skeletal muscle [19]. NAD+ repletion in animal models reverses fatty liver disease through activation of the mitochondrial unfolded protein response [20].
A systematic review with meta-analysis examining NAD+ precursor supplementation effects on glucose and lipid metabolism found significant reductions in triglycerides and increases in HDL cholesterol, particularly with niacin-based interventions. Blood glucose showed a slight increase in some studies, warranting monitoring in metabolically susceptible individuals [14].
NAD+ and Addiction Recovery
The Basics
NAD+ therapy for addiction recovery dates back to the 1960s, making it one of the oldest applications of the compound. The theory is that substance abuse depletes NAD+ levels, contributing to the mood disturbances, cravings, and cognitive impairment that characterize withdrawal. Restoring NAD+ may help reset neurotransmitter balance and reduce cravings.
High-dose IV NAD+ infusions (500-1,500 mg daily for up to 10 days) have been used in open-label studies for substance use disorders, with participants reporting reduced cravings and improved mood. However, these studies lack the rigorous controls (randomization, blinding, placebo groups) needed to confirm efficacy. The clinical interest remains active but the evidence base is still preliminary.
The Science
Open-label studies using high-dose intravenous NAD+ (500-1,500 mg daily for approximately 10 days) in substance use disorder patients have reported reductions in cravings and improvements in mood during follow-up periods [21]. A pilot study of 50 cases combining NAD+ with enkephalinase infusions reported attenuated burden of substance use disorder symptoms [22]. However, no adequately powered randomized controlled trials have been published, and the mechanistic basis remains theoretical, centered on NAD+-dependent restoration of disrupted neurotransmitter metabolism and mitochondrial function in the reward circuitry [10].
Biomarker Evidence Matrix
Category
Energy Levels
- Evidence Strength
- 6/10
- Reported Effectiveness
- 7/10
- Summary
- Multiple preclinical studies demonstrate improved mitochondrial ATP production. Human precursor trials show improved exercise capacity. Community reports strongly positive for energy with proper titration.
Category
Focus & Mental Clarity
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Mechanistic support through sirtuin activation and PGC-1alpha neuroprotection. Limited direct human cognitive data. Community reports positive but often confounded with energy improvement.
Category
Mood & Wellbeing
- Evidence Strength
- 4/10
- Reported Effectiveness
- 6/10
- Summary
- MAO pathway modulation and addiction recovery literature suggest mood effects. No dedicated mood RCTs. Community reports positive but bidirectional (some experience anxiety).
Category
Longevity & Neuroprotection
- Evidence Strength
- 7/10
- Reported Effectiveness
- 5/10
- Summary
- Strong preclinical evidence across multiple models. Human clinical trials underway. Community reports mostly theoretical enthusiasm with limited experiential data.
Category
Recovery & Healing
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- Supported by DNA repair mechanism (PARP activation). Limited direct clinical evidence for recovery. Community reports sparse.
Category
Physical Performance
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Human precursor trials show improved exercise capacity and muscle function. Community reports limited but positive.
Category
Sleep Quality
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Limited direct evidence. Circadian NAD+ cycling is well-documented but therapeutic implications unclear. Community reports mixed, with insomnia a common side effect.
Category
Pain Management
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Minimal direct evidence. One fibromyalgia report positive. Biotin synergy mentioned in community sources.
Category
Skin Health
- Evidence Strength
- 4/10
- Reported Effectiveness
- 4/10
- Summary
- Nicotinamide RCT (500mg BID, n=386) showed 23% reduction in non-melanoma skin cancer. Community reports for injectable NAD+ skin benefits are sparse.
Category
Heart Health
- Evidence Strength
- 5/10
- Reported Effectiveness
- N/A
- Summary
- Preclinical evidence of vascular protection and reversal of age-related aortic dysfunction. No community effectiveness data specific to cardiovascular outcomes.
Category
Anxiety
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- No direct evidence for anxiolytic effect. Community reports bidirectional: some improvement, some worsening. Methylation depletion mechanism proposed for anxiety induction.
Category
Nausea & GI Tolerance
- Evidence Strength
- N/A
- Reported Effectiveness
- 3/10
- Summary
- Not a benefit category. Nausea is a consistently reported side effect, particularly with IV and high-dose protocols.
Category
Heart Rate & Palpitations
- Evidence Strength
- N/A
- Reported Effectiveness
- 3/10
- Summary
- Not a benefit category. Elevated heart rate and palpitations reported as dose-dependent adverse effects.
Category
Side Effect Burden
- Evidence Strength
- N/A
- Reported Effectiveness
- 4/10
- Summary
- Overall burden moderate. Manageable with proper titration. Dose-dependent.
Benefits & Potential Effects
The Basics
The potential benefits of NAD+ supplementation cluster around a few core themes, all flowing from the same underlying mechanism: restoring the cellular energy and repair capacity that declines with age.
The most commonly reported benefit is improved energy. This makes sense mechanistically because NAD+ is literally the molecule your mitochondria need to produce ATP. Many users report that the afternoon energy crashes they had grown accustomed to simply disappear, and that their overall stamina and daily functioning improve.
Cognitive benefits are the second most discussed area. Users frequently describe reduced brain fog, improved mental clarity, and better ability to focus and multitask. Whether this is a direct effect on brain chemistry or an indirect result of having more cellular energy is still debated, but the outcome is consistent enough to be noteworthy.
Beyond energy and cognition, NAD+ research suggests potential benefits for cardiovascular health (protecting blood vessels from age-related stiffening), metabolic function (improving insulin sensitivity and fat metabolism), immune regulation, and DNA repair. These are longer-term, less immediately noticeable effects that are better supported by research data than by subjective community reports.
The Science
Evidence-supported potential benefits of NAD+ repletion include:
Mitochondrial Function Enhancement: NAD+ is required for electron transport chain activity. Preclinical studies demonstrate 30-40% improvement in mitochondrial function with NAD+ precursor supplementation. Human trials confirm increased NAD+ levels and improved exercise capacity in aged populations [13].
Sirtuin-Mediated Gene Regulation: Restored NAD+ levels reactivate SIRT1-dependent deacetylation of PGC-1alpha (mitochondrial biogenesis), FOXO proteins (stress resistance), and NF-kB (inflammation suppression) [2][3].
DNA Repair Support: Adequate NAD+ pools sustain PARP-mediated DNA strand break repair, potentially reducing mutation accumulation and genomic instability associated with aging and cancer risk [7].
Vascular Protection: In mouse models, NAD+ supplementation protects blood vessels against age-related arterial stiffening and atherosclerotic plaque deposition, with some studies showing reversal of existing age-related aortic dysfunction [12].
Metabolic Flexibility: NAD+ is required at every step of beta-oxidation (fatty acid metabolism). Adequate NAD+ pools support efficient fuel switching between glucose and fat oxidation, a capacity that declines with age and metabolic disease [20].
Neuroprotection: NAD+ supports neuronal survival through enhanced mitochondrial function, reduced ROS production, and modulation of the kynurenine pathway [15][16][17][18].
Side Effects & Safety Considerations
The Basics
NAD+ has a notable side effect profile that is highly dose-dependent. The experience of someone who starts at a low dose and gradually increases is often dramatically different from someone who begins with a high dose or receives a rapid IV infusion.
The most common side effects at standard subcutaneous doses (50-100 mg/day) include injection site reactions (redness, itching, soreness), mild nausea, and transient flushing. These typically resolve within the first week or two as the body adjusts.
The more concerning side effects tend to appear with higher doses or rapid administration. These include insomnia (NAD+ is stimulatory, and dosing late in the day can disrupt sleep), anxiety (potentially related to methylation depletion, see below), elevated heart rate and palpitations, chest pressure, and headache. IV infusions carry additional risks including rate-related reactions where pushing the infusion too fast triggers nausea, body aches, and cardiovascular symptoms.
One pattern worth understanding: NAD+ metabolism consumes methyl groups. If you have genetic variants affecting methylation (such as MTHFR mutations) or do not supplement with methyl donors, NAD+ can deplete your methyl reserves. This is proposed as the mechanism behind the anxiety and "wired but tired" feeling some users report. Supplementing with TMG (trimethylglycine) and methylated B-vitamins is widely recommended in community protocols to prevent this issue.
The Science
Rate-Dependent Reactions (IV): Flushing, warmth, nausea, chest pressure, dyspnea, and headache are more likely with rapid infusion rates. A 750 mg IV infusion delivered over 6 hours was well-tolerated, while faster rates produce more symptoms [9][10].
Cardiovascular Effects: Dose-dependent elevation of heart rate has been reported in community settings, including tachycardia episodes exceeding 170 bpm in isolated cases following injection. These events appear related to dose magnitude and individual sensitivity rather than an inherent property of NAD+ at standard doses [10].
Methylation Depletion: NAD+ metabolism via the salvage pathway produces nicotinamide, which is methylated by nicotinamide N-methyltransferase (NNMT) using S-adenosylmethionine (SAM) as a methyl donor. High-dose NAD+ supplementation may increase demand on methylation pathways, potentially depleting methyl donors in individuals with compromised methylation capacity (MTHFR variants, inadequate folate/B12 status). Clinical manifestation may include anxiety, irritability, and mood disturbance [23].
Renal Considerations: Biochemical handling suggests significant renal excretion of NAD+ metabolites. Long-term parenteral safety data are limited. Monitoring renal function (SCr/eGFR) is recommended for frequent dosing protocols [10].
Drug/Condition Interactions: Use caution in unstable cardiovascular disease, arrhythmias, severe pulmonary disease, and pregnancy/lactation (insufficient safety data) [10].
No severe adverse events have been reported in published NAD+/NADH clinical trials. The overall safety profile appears favorable when dosed appropriately with gradual titration [24].
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders

Reminder tracking supports consistency; it does not select a protocol for you.
Dosing Protocols
The Basics
NAD+ dosing is one of the areas where sources differ the most, and the single most important principle is to start low and increase gradually. Many negative experiences with NAD+ trace back to starting at too high a dose. The body needs time to adjust, and rushing the process often produces the very side effects (insomnia, anxiety, nausea, elevated heart rate) that give people a bad experience.
For subcutaneous self-injection, the most commonly reported starting point across sources is 50 mg per day for the first week, increasing to 75 mg in week two, and reaching 100 mg per day by week three if well-tolerated. This gradual titration protocol runs for 8 to 16 weeks. Some community sources suggest lower starting doses of 25 mg two to three times per week, particularly for people who are sensitive or new to injectables.
For intramuscular injection in the context of stacking protocols (combining NAD+ with other compounds), higher doses of 100 to 300 mg given three to five times per week are reported in practitioner-derived protocols. These doses are notably higher than standalone subcutaneous protocols.
IV infusion protocols, typically administered in clinical settings, use much higher doses: 500 to 1,000 mg infused slowly over several hours. These are primarily associated with addiction treatment and acute metabolic support applications.
The Science
Subcutaneous Protocol (Standalone, Wellness):
Phase
Titration Week 1
- Dose
- 50 mg SC
- Frequency
- Once daily
- Duration
- 7 days
Phase
Titration Week 2
- Dose
- 75 mg SC
- Frequency
- Once daily
- Duration
- 7 days
Phase
Maintenance Weeks 3-16
- Dose
- 100 mg SC
- Frequency
- Once daily
- Duration
- 6-14 weeks
IM/Stacking Protocol:
Context
Mito Stack (SS-31 + MOTS-c + NAD+)
- Dose
- 100-300 mg IM
- Frequency
- 3-5x/week
- Duration
- 4-12 weeks
Context
Retatrutide + NAD+
- Dose
- 100-200 mg IM/SC
- Frequency
- 5x/week
- Duration
- 12 weeks
Context
Immune Protocol
- Dose
- 50-250 mg IM
- Frequency
- 1-3x/week
- Duration
- 4+ weeks
IV Protocol (Clinical Setting Only):
Application
Addiction/Acute Support
- Dose
- 500-1,000 mg IV
- Frequency
- Daily (slow infusion over 4-6 hours)
- Duration
- 5-10 days
Application
Metabolic Support
- Dose
- 750 mg IV
- Frequency
- Single session or weekly
- Duration
- Variable
Reconstitution (500 mg vial): Add 3.0 mL bacteriostatic water for a concentration of 166.7 mg/mL. At this concentration, 1 unit on a U-100 insulin syringe equals approximately 1.67 mg. Example conversions: 50 mg = 30 units; 75 mg = 45 units; 100 mg = 60 units [25].
Oral Precursor Alternatives:
- Nicotinamide Riboside (NR): 300-500 mg daily
- Nicotinamide Mononucleotide (NMN): 250-500 mg daily
- These raise NAD+ levels more gradually but reliably, and do not match injectable NAD+ for acute repletion [26].
The side effects and contraindications above give you a map of what to watch for. Doserly turns that map into a daily practice. Log the specific biomarkers and symptoms associated with this compound's known risk profile, and the app builds a timeline of how your body is responding across your cycle.
Trending in the wrong direction on a key marker? Noticing a pattern that started two weeks into your protocol? Doserly connects the dots between your protocol timeline and your logged data, making it easier to spot emerging issues early and have informed, data-backed conversations with your healthcare provider about what's working and what needs attention.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
What to Expect
Week 1 (Titration at 50 mg/day SC):
The first few days may be uneventful, or you may notice mild injection site soreness and possibly slight nausea. Some users report a subtle energy shift within the first few days; others notice nothing. The initial titration period is about assessing tolerance, not expecting dramatic results. If you experience insomnia, ensure you are dosing in the morning.
Weeks 2-3 (Increasing to 75-100 mg/day):
This is where most users begin to notice changes if they are going to respond. The most commonly reported early benefit is reduced afternoon energy crashes and improved sustained energy throughout the day. Some users report clearer thinking and reduced brain fog. Mild side effects from the initial days typically resolve during this period as the body adjusts.
Weeks 4-8 (Steady State):
Benefits tend to consolidate and become the new baseline rather than a novelty. Users report consistent energy levels, improved workout recovery, and better mental clarity becoming their normal state. Some users report improved sleep quality (despite insomnia being a side effect for others, typically resolved by morning dosing). This is the period where the cumulative effects of sustained NAD+ repletion on sirtuin activity and DNA repair are theoretically building.
Weeks 8-16 (Extended Protocol):
Long-term users describe the benefits as becoming less dramatic and more integrated into their daily experience. The contrast is most noticeable if they stop the protocol and experience a return of pre-supplementation fatigue and fog. Some practitioners recommend cycling (8-12 weeks on, 4-8 weeks off) while others support continuous use. The optimal long-term protocol has not been established.
Important Note: Response is highly individual. A meaningful minority of users report minimal or no noticeable benefits, particularly younger users (under 40) who may have higher baseline NAD+ levels. Others report dramatic, life-changing improvements, particularly those with chronic fatigue or age-related energy decline.
Interaction Compatibility
Good With (Synergistic Compounds)
- SS-31 — Stabilizes mitochondrial membranes while NAD+ provides the redox fuel. Together they address mitochondrial structure and energy currency simultaneously. Core component of the Mito Stack.
- MOTS-C — Signals the nucleus to build new mitochondria (biogenesis) and shift metabolism toward fat oxidation. Complements NAD+'s role as energy fuel with metabolic reprogramming.
- BPC-157 — Vascular restoration compound paired with NAD+ for injury recovery protocols.
- TB-500 — Tissue repair compound; NAD+ supports the energy demands of healing processes.
- GHK-Cu — Copper peptide for collagen and tissue quality; paired with NAD+ in comprehensive recovery stacks.
- 5-Amino-1MQ — NNMT inhibitor that reduces NAD+ consumption, effectively conserving NAD+ pools. Complementary mechanism.
- Thymosin Alpha-1 — Immune reconstitution compound; NAD+ provides the metabolic foundation for immune cell function.
- Selank — Anxiolytic peptide; addresses the stress/cortisol component that depletes NAD+ through PARP activation.
- TMG (Trimethylglycine) — Methyl donor that prevents methylation depletion during NAD+ supplementation. Widely recommended as an essential co-supplement.
- CoQ10 — Fellow mitochondrial cofactor; may work synergistically to improve electron transport chain efficiency and neurological function.
- Resveratrol — Sirtuin activator; works synergistically with NAD+ to enhance sirtuin-mediated benefits including reduced oxidative damage and inflammation.
- B-Vitamins (methylated complex) — Support NAD+ salvage pathway and prevent methylation-related side effects.
- Apigenin — CD38 inhibitor that reduces NAD+ degradation, helping exogenous NAD+ last longer.
Not Good With (Caution)
- High-dose serotonergic medications — While NAD+ is not a direct serotonin modulator, its effects on neurotransmitter metabolism warrant caution with SSRIs, SNRIs, and MAOIs.
- Compounds with significant cardiovascular effects — Given NAD+'s potential for heart rate elevation, caution when stacking with compounds that also affect cardiovascular parameters.
- Alcohol — Alcohol metabolism directly consumes NAD+, counteracting supplementation and increasing side effect risk.
Administration Guide
Materials Required:
- NAD+ lyophilized vial (typically 500 mg or 1000 mg)
- Bacteriostatic water (0.9% benzyl alcohol)
- U-100 insulin syringes (29-31 gauge, 5/16 to 1/2 inch needle)
- Alcohol swabs
- Sharps container
Recommended Reconstitution Solution: Bacteriostatic water (0.9% benzyl alcohol). Add 3.0 mL to a 500 mg vial for a concentration of 166.7 mg/mL. The solution should be clear and colorless. Discard if any discoloration or precipitate appears. NAD+ powder is extremely hygroscopic, so allow the vial to reach room temperature before opening to minimize moisture condensation.
Timing Considerations:
- Morning administration is strongly recommended. NAD+ is stimulatory, and afternoon or evening dosing frequently causes insomnia.
- Some practitioners suggest early afternoon timing to align with circadian NAD+ troughs, but community experience favors morning dosing for most users.
- Administer at a consistent time each day for optimal protocol adherence.
Post-Administration Care:
- Inject slowly over 5-10 seconds to minimize tissue irritation.
- Mild injection site redness and soreness are common and typically resolve within 24 hours.
- Monitor for systemic reactions during the first week of a new protocol: elevated heart rate, flushing, nausea, or anxiety.
- If persistent redness or lumps develop, apply over-the-counter hydrocortisone cream and rotate to a different site.
- Document dose, injection site, and any observed effects daily to track tolerance patterns.
Supplies & Planning
NAD+ Vials: Available in 500 mg and 1000 mg lyophilized formats from compounding pharmacies.
Bacteriostatic Water: 10 mL bottles. Each 500 mg vial uses 3.0 mL for reconstitution.
Insulin Syringes: U-100, 1 mL capacity, 29-31 gauge, 5/16 to 1/2 inch needle length. One syringe per injection.
Alcohol Swabs: Two per injection (one for vial stopper, one for injection site).
Sharps Container: For safe disposal of used needles and syringes.
Storage Requirements: Lyophilized vials require freezer storage (-20C minimum, -80C ideal). Reconstituted solution must be refrigerated (2-8C) and used within 14 days. NAD+ is extremely sensitive to moisture, light, and heat. Wrap vials in foil or store in opaque containers.
For specific quantity calculations based on your protocol parameters, consult with your healthcare provider and use the reconstitution calculator for preparation math.
Storage & Handling
Lyophilized (Powder):
- Store at -20C (-4F) or below. Ideal long-term storage at -80C for up to 2-3 years.
- Short-term refrigeration at 2-8C (35.6-46.4F) is acceptable for weeks to months.
- NAD+ powder is extremely hygroscopic (absorbs moisture from the air). Always keep in original sealed packaging with desiccant.
- Allow vials to reach room temperature (10-30 minutes) before opening to prevent condensation inside the vial.
- Store in a dry, dark environment away from direct sunlight.
Reconstituted (Liquid):
- Refrigerate immediately at 2-8C (35.6-46.4F) after reconstitution.
- Use within 14 days maximum.
- Protect from light (UV exposure degrades NAD+).
- Do NOT freeze reconstituted solution. Freezing denatures the compound.
- Avoid repeated freeze-thaw cycles.
- Inspect before each use: solution should be clear and colorless. Discard if cloudiness, discoloration, or precipitate appears.
Lifestyle Factors
NAD+ supplementation does not operate in isolation. Several lifestyle factors directly influence NAD+ levels and can either amplify or counteract the effects of supplementation.
Nutrition: A diet rich in NAD+ precursors supports the salvage pathway that recycles NAD+. Key dietary sources include tryptophan (found in turkey, chicken, eggs, cheese), niacin/vitamin B3 (tuna, chicken, mushrooms, peanuts), and nicotinamide (beef, pork, nuts, seeds). B-vitamins and magnesium support the enzymatic pathways that process NAD+. TMG (trimethylglycine) at 500-1,000 mg daily is widely recommended to protect methylation capacity during NAD+ supplementation.
Exercise: Regular physical activity is one of the most potent natural stimulators of NAD+ biosynthesis. Both resistance training and aerobic exercise upregulate NAMPT (the rate-limiting enzyme in the NAD+ salvage pathway) and enhance mitochondrial adaptations. Exercise and NAD+ supplementation appear to have synergistic effects.
Sleep: NAD+ metabolism follows circadian patterns, and cellular repair processes that consume NAD+ are most active during sleep. Prioritizing 7-9 hours of quality sleep supports the DNA repair and metabolic restoration that NAD+ enables. Conversely, NAD+ supplementation can disrupt sleep if dosed too late in the day.
Alcohol: Alcohol metabolism directly consumes NAD+ through the alcohol dehydrogenase and aldehyde dehydrogenase pathways. Even moderate alcohol consumption during an NAD+ protocol counteracts supplementation and may increase side effect risk. Reducing or eliminating alcohol intake during NAD+ protocols is one of the most impactful lifestyle modifications.
Stress Management: Chronic stress activates PARP enzymes (through stress-induced DNA damage) and increases CD38 expression (through inflammatory signaling), both of which consume NAD+. Stress reduction practices including meditation, breathwork, and adequate recovery time support NAD+ conservation.
Peptide protocols don't exist in a vacuum. Your nutrition, exercise, sleep, stress, and the rest of your health stack all influence outcomes. Doserly tracks your entire health picture in one place: peptides, supplements, medications, TRT/HRT, and the lifestyle factors that determine whether your protocol reaches its potential.
This holistic view reveals correlations that compartmentalized tracking misses. You might discover that your recovery improvements stall during weeks with poor sleep, or that adding a specific supplement amplified a benefit you were already seeing. Doserly's cross-category visibility helps you understand which lifestyle factors are pulling the most weight in your results, turning health optimization from guesswork into a data-informed practice.
See how each compound fits into the whole protocol.
Doserly organizes compounds, supplements, peptides, medications, and hormone protocols together so overlapping routines are easier to understand.
Stack view
Connected protocol
Stack views improve organization; they do not determine compatibility.
Regulatory Status & Research Classification
United States (FDA): NAD+ is not approved as a pharmaceutical product. It is classified as a naturally occurring metabolite. NAD+ precursors NMN and NR are available as over-the-counter dietary supplements (NMN's supplement status was contested by the FDA in 2022-2023 due to its prior investigation as a drug candidate, but NMN supplements remain widely available). Injectable NAD+ is obtained through compounding pharmacies and is not FDA-approved for any specific therapeutic indication.
Canada (Health Canada): NAD+ precursors (NR, niacin) are available as natural health products. Injectable NAD+ regulatory status follows compounding pharmacy regulations.
United Kingdom (MHRA): NAD+ IV therapy is offered through private wellness clinics. NAD+ precursors are available as supplements. Not a licensed medicine.
Australia (TGA): NAD+ precursors are available as supplements. Injectable NAD+ is available through compounding pharmacies under practitioner supervision.
European Union (EMA): No marketing authorization for NAD+ as a pharmaceutical product. NAD+ precursors available as food supplements under EU regulations.
WADA Status: NAD+ and its precursors are not currently on the World Anti-Doping Agency prohibited list.
Active Clinical Trials: Multiple registered trials examining NAD+-boosting interventions for aging, metabolic disease, neurodegeneration, and cardiovascular health. Clinicaltrials.gov lists active trials for NMN and NR supplementation across various conditions.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is the difference between NAD+, NMN, and NR?
NAD+ is the active coenzyme itself. NMN (nicotinamide mononucleotide) and NR (nicotinamide riboside) are precursors that your body converts into NAD+. Oral NMN and NR supplements are widely available and raise NAD+ levels gradually over days to weeks. Injectable NAD+ delivers the molecule directly into circulation for faster repletion but requires injection. Based on available data, no definitive head-to-head human study exists between injectable NAD+ and oral precursors for most outcomes.
Is NAD+ actually a peptide?
No. NAD+ is a dinucleotide coenzyme, not a peptide. It appears in peptide guides because it is commonly used alongside peptides in biohacking and longevity protocols, and the community that researches peptides frequently researches NAD+ as well. It works through entirely different mechanisms than peptide compounds.
Why do some people feel terrible on NAD+ while others love it?
Community reports suggest that response is highly dose-dependent and individually variable. Users who start at low doses (25-50 mg) and titrate gradually tend to report positive experiences. Users who begin at higher doses or receive rapid IV infusions are more likely to report adverse reactions. Methylation status may also play a role: individuals with compromised methylation capacity may experience anxiety and mood disturbances, which can be mitigated with TMG and methylated B-vitamin supplementation.
What time of day is best for NAD+ administration?
Based on community experience and practitioner recommendations, morning administration is strongly favored. NAD+ is stimulatory, and afternoon or evening dosing frequently causes insomnia and sleep disruption.
How long does it take to notice effects?
Based on community reports, some users notice energy improvements within the first week of titration, while others require 2-4 weeks at maintenance doses. A meaningful minority report no noticeable subjective effects. Longer-term cellular benefits (DNA repair, sirtuin activation) are not subjectively perceptible and operate over weeks to months.
Can I take oral NMN/NR instead of injecting NAD+?
Based on available data, oral precursors (NMN at 250-500 mg daily or NR at 300-500 mg daily) reliably raise NAD+ levels and have a growing evidence base from human clinical trials. They do not provide the same acute peak levels as injection but offer convenience, lower cost, and avoiding injection-related side effects. Many practitioners use oral precursors as a maintenance layer and injectable NAD+ for acute repletion.
Sources & References
Reviews and Meta-Analyses
[1] Xie N, et al. NAD+ metabolism: pathophysiologic mechanisms and therapeutic potential. Signal Transduction and Targeted Therapy. 2020;5:227. https://pubmed.ncbi.nlm.nih.gov/33028824/
[2] Imai S, Guarente L. NAD+ and sirtuins in aging and disease. Trends Cell Biol. 2014;24(8):464-471. https://pubmed.ncbi.nlm.nih.gov/24786309/
[3] Rajman L, Chwalek K, Sinclair DA. Therapeutic potential of NAD-boosting molecules: the in vivo evidence. Cell Metab. 2018;27(3):529-547. https://pubmed.ncbi.nlm.nih.gov/29514064/
[4] Covarrubias AJ, et al. NAD+ metabolism and its roles in cellular processes during ageing. Nature Reviews Molecular Cell Biology. 2021;22:119-141. https://pubmed.ncbi.nlm.nih.gov/33353981/
[5] Massudi H, et al. Age-associated changes in oxidative stress and NAD+ metabolism in human tissue. PLoS One. 2012;7(7):e42357. https://pubmed.ncbi.nlm.nih.gov/22848760/
Mechanism and Pharmacology
[6] Ying W. NAD+/NADH and NADP+/NADPH in cellular functions and cell death: regulation and biological consequences. Antioxid Redox Signal. 2008;10(2):179-206. https://pubmed.ncbi.nlm.nih.gov/18020963/
[7] Lloret A, Beal MF. PGC-1alpha, Sirtuins and PARPs in Huntington's Disease and Other Neurodegenerative Conditions: NAD+ to Rule Them All. Neurochem Res. 2019;44(10):2423-2434. https://pubmed.ncbi.nlm.nih.gov/31054010/
[8] Chini EN, et al. CD38 as a regulator of cellular NAD: a novel potential pharmacological target for metabolic conditions. Curr Pharm Des. 2009;15(1):57-63. https://pubmed.ncbi.nlm.nih.gov/19149603/
Human Studies
[9] Grant R, et al. A pilot study investigating changes in the human plasma and urine NAD+ metabolome during a 6 hour intravenous infusion of NAD+. Front Aging Neurosci. 2019;11:257. https://pubmed.ncbi.nlm.nih.gov/31572159/
[10] Braidy N, et al. Role of Nicotinamide Adenine Dinucleotide and Related Precursors as Therapeutic Targets for Age-Related Degenerative Diseases. Antioxid Redox Signal. 2019;30(2):251-294. https://pubmed.ncbi.nlm.nih.gov/29634344/
Preclinical Evidence
[11] Gomes AP, et al. Declining NAD+ Induces a Pseudohypoxic State Disrupting Nuclear-Mitochondrial Communication during Aging. Cell. 2013;155(7):1624-1638. https://pubmed.ncbi.nlm.nih.gov/24360282/
[12] Mendelsohn AR, Larrick JW. Partial reversal of skeletal muscle aging by restoration of normal NAD+ levels. Rejuvenation Res. 2014;17(1):62-69. https://pubmed.ncbi.nlm.nih.gov/24410488/
Clinical Trial Data
[13] Alegre GFS, et al. Dietary Supplementation With NAD+-Boosting Compounds in Humans: Current Knowledge and Future Directions. J Nutr. 2023;153(12):3483-3502. https://pubmed.ncbi.nlm.nih.gov/37068054/
[14] Zhong O, et al. Effects of NAD+ precursor supplementation on glucose and lipid metabolism in humans: a meta-analysis. Nutr Metab. 2022;19:20. https://pubmed.ncbi.nlm.nih.gov/35303905/
Neuroprotection
[15] Shan C, et al. Protective effects of beta-nicotinamide adenine dinucleotide against motor deficits and dopaminergic neuronal damage in a mouse model of Parkinson's disease. Prog Neuropsychopharmacol Biol Psychiatry. 2019;94:109670. https://pubmed.ncbi.nlm.nih.gov/31132411/
[16] Maddison DC, Giorgini F. The kynurenine pathway and neurodegenerative disease. Semin Cell Dev Biol. 2015;40:134-141. https://pubmed.ncbi.nlm.nih.gov/25773161/
[17] Lautrup S, et al. NAD+ in Brain Aging and Neurodegenerative Disorders. Cell Metab. 2019;30(4):630-655. https://pubmed.ncbi.nlm.nih.gov/31577933/
[18] Chong R, et al. Progresses in both basic research and clinical trials of NAD+ in Parkinson's disease. Neural Regen Res. 2022;17(8):1680-1683. https://pubmed.ncbi.nlm.nih.gov/33989633/
Metabolic Health
[19] Yamaguchi S, Yoshino J. Adipose Tissue NAD+ Biology in Obesity and Insulin Resistance: From Mechanism to Therapy. BioEssays. 2017;39(5):1600227. https://pubmed.ncbi.nlm.nih.gov/28417465/
[20] Gariani K, et al. Eliciting the mitochondrial unfolded protein response by nicotinamide adenine dinucleotide repletion reverses fatty liver disease in mice. Hepatology. 2016;63(4):1190-1204. https://pubmed.ncbi.nlm.nih.gov/26404765/
Addiction and Clinical Applications
[21] Braidy N, et al. Preclinical and clinical evidence of NAD+ precursors in health, disease, and ageing. Curr Nutr Rep. 2021;10(3):292-317. https://pubmed.ncbi.nlm.nih.gov/34517020/
[22] Zucker M, et al. NAD+ and enkephalinase infusions attenuate burden in substance use disorder: a pilot study. Curr Psychiatry Res Rev. 2020;16(1):53-60.
Safety and Pharmacokinetics
[23] Garten A, et al. Physiological and pathophysiological roles of NAMPT and NAD metabolism. Nat Rev Endocrinol. 2015;11(9):535-546. https://pubmed.ncbi.nlm.nih.gov/26215259/
[24] American Journal of Physiology. Evaluation of safety and effectiveness of NAD+ in different clinical conditions: a systematic review.
[25] Reference site protocol reconstitution guide. Educational resource.
[26] Yoshino J, et al. NAD+ Intermediates: The Biology and Therapeutic Potential. Cell Metab. 2018;27(3):513-528. https://pubmed.ncbi.nlm.nih.gov/29249689/
Related Peptide Guides
- SS-31 — Mitochondrial membrane stabilizer; core component of Mito Stack with NAD+
- MOTS-C — Mitochondrial-derived peptide for metabolic programming; pairs with NAD+ in energy protocols
- 5-Amino-1MQ — NNMT inhibitor that conserves NAD+ pools
- BPC-157 — Tissue repair peptide; paired with NAD+ in recovery protocols
- TB-500 — Thymosin Beta-4 fragment for healing; complementary to NAD+ in injury recovery
- GHK-Cu — Copper peptide for collagen and tissue quality
- Thymosin Alpha-1 — Immune modulator; NAD+ provides metabolic foundation for immune function
- Selank — Anxiolytic peptide; addresses stress that depletes NAD+
- Methylene Blue — Alternative mitochondrial electron carrier with complementary mechanism
- BAM15 — Mitochondrial uncoupler for metabolic flexibility
- Glutathione — Antioxidant frequently co-administered with NAD+ in wellness protocols
- Semaglutide — GLP-1 agonist; NAD+ supports fat oxidation during caloric restriction
- Retatrutide — Triple agonist; NAD+ prevents energy crash during aggressive fat loss
- Tirzepatide — GLP-1/GIP agonist; NAD+ commonly added for fatigue management
Need the reconstitution math for NAD+: Complete Research Guide?
Open the calculator with NAD+: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.