GHRP-2: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Pralmorelin, Growth Hormone Releasing Peptide-2, KP-102, GPA 748
Attribute
Administration
- Detail
- Injectable (subcutaneous)
Attribute
Research Status
- Detail
- Research Compound. Never approved by the FDA. Used diagnostically in Japan for GH deficiency evaluation (Pralmorelin). WADA prohibited.
Attribute
Typical Dose Range
- Detail
- 100-300 mcg per injection, 1-3 times daily
Attribute
Half-Life
- Detail
- 25-55 minutes
Attribute
Cycle Length
- Detail
- 8-16 weeks on, 4-6 weeks off
Attribute
Storage
- Detail
- Lyophilized: -20°C long-term; Reconstituted: 2-8°C (use within 4 weeks)
Overview / What Is GHRP-2?
The Basics
GHRP-2 is a synthetic peptide that tells your pituitary gland to release more growth hormone. It belongs to a family called growth hormone releasing peptides, or GHRPs, and sits in the middle of the potency-versus-side-effect spectrum. Where Ipamorelin (the third-generation version) trades some potency for an extremely clean side effect profile, and GHRP-6 (the first generation) provides strong GH pulses but comes with intense hunger and more off-target hormonal effects, GHRP-2 lands in between: stronger than Ipamorelin, but with fewer side effects than GHRP-6.
The peptide works by mimicking ghrelin, the hormone your stomach produces to signal hunger. This is why appetite stimulation is the most commonly reported effect. For people trying to eat more (bodybuilders in a bulking phase, individuals recovering from illness), this can be helpful. For people trying to manage their weight, it can be counterproductive.
GHRP-2 has been studied as a diagnostic tool for evaluating pituitary function in growth hormone deficiency. Its strongest clinical evidence comes from combination protocols with GHRH analogs, where the two types of peptides work through different pathways to produce a synergistic growth hormone response greater than either achieves alone.
The Science
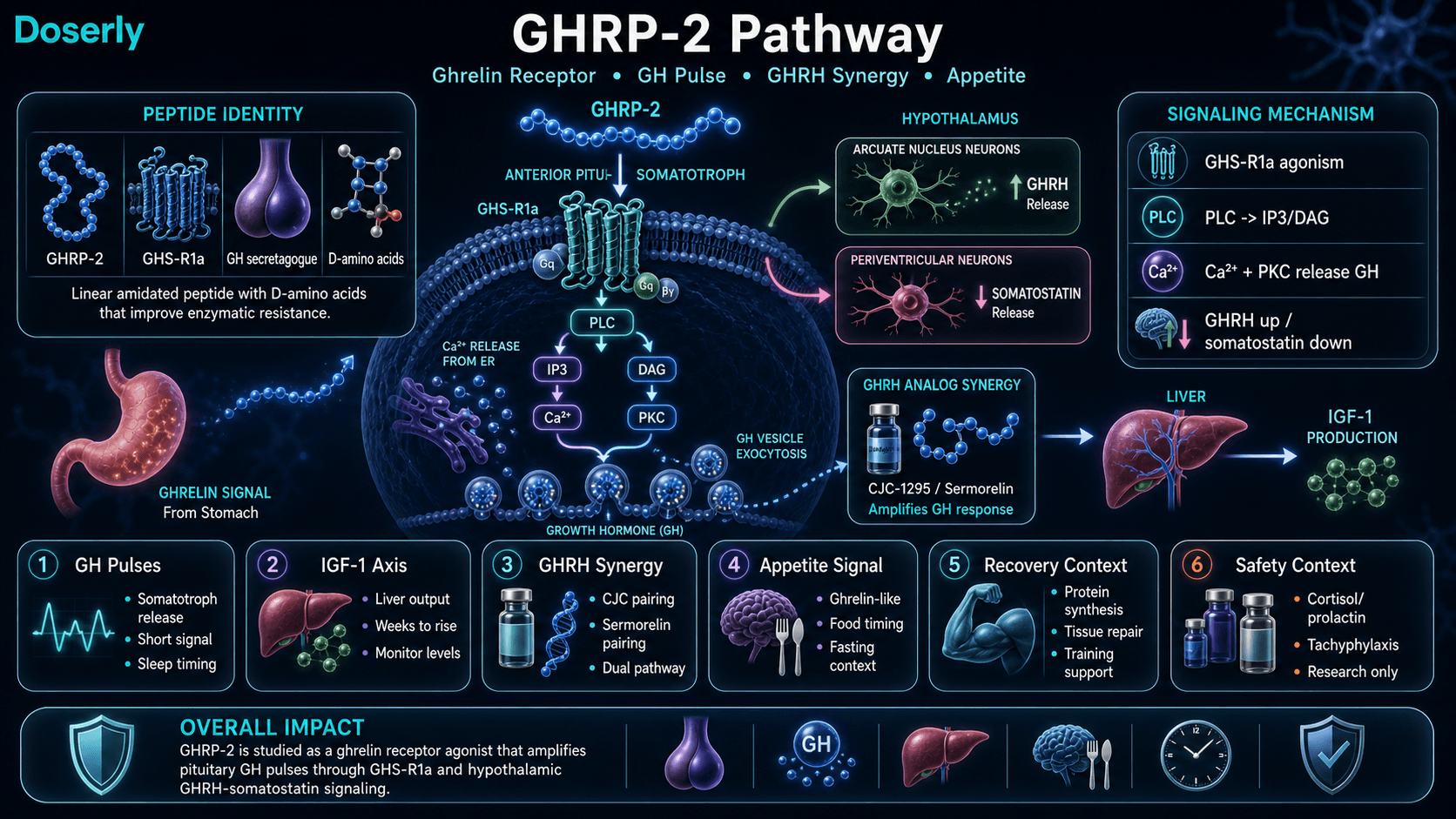
GHRP-2 (Growth Hormone Releasing Peptide-2, Pralmorelin) is a synthetic hexapeptide (molecular weight 817.98 Da) that stimulates growth hormone secretion through selective agonism of the growth hormone secretagogue receptor type 1a (GHS-R1a) [1][2]. The compound acts through a signaling pathway independent of growth hormone releasing hormone (GHRH), engaging PLC/PKC-mediated calcium mobilization in pituitary somatotrophs rather than the cAMP/PKA pathway utilized by GHRH analogs [3][4].
Unlike exogenous growth hormone administration, GHRP-2 stimulates endogenous pulsatile GH release that preserves the somatostatin negative feedback mechanism, limiting the potential for supraphysiological GH elevation [5]. The peptide also demonstrates mild stimulation of prolactin and cortisol release, distinguishing it from more selective third-generation GHS-R1a agonists such as ipamorelin [6][7].
Clinical investigation has focused on two areas: diagnostic evaluation of pituitary GH reserve (where it is used as a provocative test for GH deficiency) and therapeutic applications in growth hormone deficiency states. In children with GH deficiency, doses of 5-15 mcg/kg administered two to three times daily sustained growth velocity of approximately 6.0 cm/year over 18-24 months [5]. Research also continues into applications for muscle wasting, age-related GH decline, and wound healing.
Molecular Identity
Attribute
Common Names
- Detail
- GHRP-2, Pralmorelin, Growth Hormone Releasing Peptide-2, KP-102, GPA 748
Attribute
Amino Acid Sequence
- Detail
- D-Ala-D-2-Nal-Ala-Trp-D-Phe-Lys-NH₂
Attribute
Molecular Formula
- Detail
- C₄₅H₅₅N₉O₆
Attribute
Molecular Weight
- Detail
- 817.98 Da
Attribute
CAS Number
- Detail
- 158861-67-7
Attribute
Structure Type
- Detail
- Linear peptide with C-terminal amidation
Attribute
D-Amino Acid Content
- Detail
- D-Ala, D-2-Nal (D-2-naphthylalanine), D-Phe, conferring enzymatic resistance
Attribute
Functional Class
- Detail
- Ghrelin receptor agonist (GHS-R1a), growth hormone secretagogue
Attribute
Salt Forms
- Detail
- Free base (most common); acetate salt; HCl salt
Attribute
Purity (Research Grade)
- Detail
- ≥95% HPLC
Mechanism of Action
The Basics
Your body has two main "switches" for releasing growth hormone from the pituitary gland. One switch is activated by GHRH (growth hormone releasing hormone), a signal that comes from your hypothalamus. The other switch is activated by ghrelin, a hunger hormone produced primarily in your stomach. GHRP-2 mimics ghrelin and flips that second switch.
When GHRP-2 binds to the ghrelin receptor on your pituitary cells, those cells release a pulse of growth hormone into your bloodstream. The pulse is temporary, mimicking your body's natural pattern of releasing GH in bursts rather than at a constant level. This pulsatile pattern is important because it is how your body normally operates, and preserving it reduces the risk of the system shutting down in response.
The ghrelin-mimicking action also explains why appetite increases after an injection. Ghrelin is your body's primary hunger signal, and GHRP-2 activates the same receptor. This effect is milder than with GHRP-6 (the first-generation version) but more noticeable than with Ipamorelin (the third generation). There are also small, transient increases in cortisol and prolactin, two other hormones that the older GHRPs tend to stimulate as a side effect of their broader receptor activity.
The real power of GHRP-2 becomes apparent when it is combined with a GHRH analog like CJC-1295 or sermorelin. Because the two pathways (GHRH and ghrelin) converge on the same pituitary cells through different signaling cascades, activating both simultaneously produces a growth hormone response that is significantly greater than the sum of what either produces alone.
The Science
GHRP-2 functions as a selective agonist at GHS-R1a, a G-protein coupled receptor expressed on anterior pituitary somatotrophs and in hypothalamic neurons [1][2]. Receptor binding initiates phospholipase C (PLC) activation, generating inositol triphosphate (IP₃) and diacylglycerol (DAG). IP₃ triggers intracellular calcium release from the endoplasmic reticulum, while DAG activates protein kinase C (PKC). This convergent signaling drives GH vesicle exocytosis [3][4].
The mechanism operates through both direct pituitary action and indirect hypothalamic pathways. At the hypothalamic level, GHRP-2 stimulates arcuate nucleus neurons to release endogenous GHRH while simultaneously suppressing somatostatin release from periventricular neurons [3]. This dual hypothalamic effect amplifies the pituitary GH response beyond what direct somatotroph stimulation would produce in isolation.
The GHRH-GHRP synergy principle is quantitatively established. Veldhuis and Bowers (2009) measured a 47-fold increase in pulsatile GH secretion with GHRP-2 alone, a 20-fold increase with GHRH alone, and a 54-fold increase with the combination, demonstrating synergy rather than simple additivity [4]. However, the same study identified important modulators: synergy magnitude declines approximately 55% in older men with low testosterone, higher visceral fat, and reduced IGF-1. Abdominal visceral fat, IGF-1, and IGFBP-3 collectively explained 60% of the variability in synergy magnitude (P<0.001) [4].
A critical mechanistic constraint: ghrelin-pathway agents require intact endogenous GHRH signaling. GHRH-knockout models show markedly attenuated responses to GHRP-2, confirming that the ghrelin receptor pathway depends on baseline GHRH tone to achieve full effect [3][4]. Patients with severe hypothalamic dysfunction may not respond fully to GHRP-2 alone.
Pathway Visualization Image
Pharmacokinetics
The Basics
GHRP-2 enters your bloodstream quickly after a subcutaneous injection and peaks within minutes. It has a short working window, typically clearing from the blood within about an hour. This short half-life is why most protocols call for multiple daily injections, and why timing matters: the peptide works best on an empty stomach, with at least two hours of fasting before and 30-60 minutes after administration.
The short duration also means GHRP-2 produces discrete, sharp GH pulses rather than a sustained elevation. This pattern closely resembles your body's natural GH secretion, which occurs in bursts throughout the day and night. The strongest natural GH pulse typically occurs during deep sleep, which is why before-bed dosing is commonly recommended to align with and amplify that natural rhythm.
However, there is a downside to repeated daily stimulation. With continuous use, the GH response may weaken over time, a phenomenon called tachyphylaxis. Clinical data shows meaningful response attenuation within five days of continuous daily dosing [8]. This is why cycling strategies (such as 5 days on, 2 days off) and periodic breaks are often incorporated into longer protocols.
The Science
GHRP-2 demonstrates pharmacokinetic properties characteristic of small synthetic peptides. Following subcutaneous administration, the compound is rapidly absorbed with peak plasma concentrations achieved within 15-30 minutes [1][2]. The plasma elimination half-life ranges from 25 to 55 minutes, consistent with the rapid clearance typical of hexapeptides and pentapeptides of similar molecular weight [7].
The D-amino acid modifications (D-Ala, D-2-Nal, D-Phe) confer superior enzymatic resistance compared to native peptide substrates, contributing to its greater stability relative to endogenous ghrelin [9]. Despite this enhanced stability, the peptide's biological activity window remains relatively short, supporting multiple daily dosing protocols.
A single subcutaneous dose of 100 mcg can raise GH levels several-fold above baseline [10]. When administered consistently, GHRP-2 elevates IGF-1 levels over weeks to months, with one study reporting approximately 50% IGF-1 increase over a 3-month treatment period [11]. However, tachyphylaxis has been documented: Nijland et al. (1998) demonstrated significant GH response attenuation after five consecutive days of subcutaneous GHRP-2 administration in healthy young men [8].
Understanding half-life data points and clearance rates is informative, but seeing how they play out across your specific dosing schedule makes them actionable. Doserly's half-life estimator models your compound's concentration curve based on your dose, frequency, and route of administration, showing projected peaks, troughs, and steady-state levels over time.
Adjusting your dose or experimenting with timing? The estimator recalculates in real time, so you can visualize how titrating up, splitting doses, or changing frequency affects your blood levels before committing to a change. It transforms the pharmacokinetic data in this section from abstract numbers into a practical planning tool for your protocol.
See how each compound fits into the whole protocol.
Doserly organizes compounds, supplements, peptides, medications, and hormone protocols together so overlapping routines are easier to understand.
Stack view
Connected protocol
Stack views improve organization; they do not determine compatibility.
Research & Clinical Evidence
GHRP-2 and Growth Hormone Deficiency
The Basics
The most established clinical use of GHRP-2 is as a diagnostic tool. When doctors suspect a child or adult has growth hormone deficiency, they can give a dose of GHRP-2 and measure how much GH the pituitary releases in response. A blunted response confirms that the pituitary is underperforming. This diagnostic application, marketed as Pralmorelin, has been used in Japan.
Beyond diagnostics, small clinical studies have explored therapeutic use. In children with GH deficiency, treatment with GHRP-2 two to three times daily sustained growth rates of about 6 centimeters per year for up to two years. This is meaningful for children who were growing far below normal rates.
The Science
Pihoker et al. (1995) demonstrated that GHRP-2 administered intravenously and intranasally effectively evaluated pituitary GH reserve in children of short stature, establishing its utility as a diagnostic provocative agent [10]. In therapeutic applications, six children with GH deficiency treated with GHRP-2 (5-15 mcg/kg, two to three times daily) for 18-24 months sustained growth velocity of approximately 6.0 cm/year [5].
GHRP-2 has also been evaluated for diagnostic assessment of thyrotropin-producing pituitary adenomas, demonstrating utility beyond standard GH evaluation [5].
GHRP-2 and Body Composition
The Basics
The available clinical data on body composition comes primarily from a combination study using GHRP-2 with other GH secretagogues. In hypogonadal men (men with low testosterone) who were also on testosterone therapy, adding a combination of growth hormone releasing peptides produced a significant increase in IGF-1 levels and improvements in testosterone. These are markers associated with favorable body composition changes, though the study did not directly measure muscle mass or fat loss.
Community reports suggest body recomposition (simultaneous muscle gain and fat loss) is possible, particularly when the peptide is combined with resistance training and adequate protein intake. However, the appetite stimulation can complicate fat loss efforts for some users.
The Science
The primary clinical evidence comes from Sigalos et al. (2017), a retrospective study of 14 hypogonadal men on testosterone who received sermorelin (100 mcg) + GHRP-2 (100 mcg) + GHRP-6 (100 mcg) three times daily [11]. Over approximately 134 days, mean IGF-1 rose from 159.5 to 239.0 ng/mL (P<0.0001), representing a 50% increase. Testosterone and free testosterone also increased significantly after 90 days, while LH and FSH remained unchanged, indicating no suppression of the pituitary-gonadal axis [11].
Limitations of this study are significant: retrospective design, only 14 compliant patients from 105 enrolled, no body composition endpoints, and results confounded by concurrent testosterone therapy [7][11]. The triple-peptide combination also makes it impossible to isolate GHRP-2's individual contribution.
GHRP-2 and Cardioprotection
The Basics
Preclinical research has found that growth hormone releasing peptides, including GHRP-2, may have protective effects on the heart and other organs. In animal models, these peptides reduced heart damage, preserved heart function, and lowered inflammatory markers. These findings are interesting but come from animal studies, not human trials.
The Science
A comprehensive 2017 review synthesized 40+ years of GHRP research, documenting cytoprotective effects mediated through both GHS-R1a and CD36 receptor pathways [12]. In animal models of dilated cardiomyopathy, GHRP-6 and GHRP-2 in combination prevented disease progression, reduced ventricular dilation, restored ejection fraction, and extended lifespan [12]. Cardioprotection occurred via positive inotropy through calcium mobilization without increasing heart rate.
In septic patients, GHRP-2 administration reduced inflammatory cytokines (TNF-alpha, IL-6) and restored organ function markers [12]. Anti-fibrotic effects were documented through PPARgamma-driven CTGF downregulation, reducing myocardial scar tissue [12].
GHRP-2 and Neuroprotection
The Basics
Early research suggests GHRP-2 may have protective effects on the brain, particularly when combined with other growth factors. In an animal model of stroke, GHRP-2 combined with epidermal growth factor showed significant neuroprotective activity. This line of research is still in its early stages.
The Science
Subiros et al. demonstrated that GHRP-2 combined with epidermal growth factor (EGF) produced significant neuroprotective activity comparable to therapeutic hypothermia in an experimental stroke model [5]. This finding suggests potential applications in acute neurological injury, though translation to human clinical settings remains uninvestigated.
Biomarker Evidence Matrix
The following table scores GHRP-2 across relevant health outcome categories. Evidence Strength reflects the quality of available research (clinical trials, animal studies, mechanistic data). Reported Effectiveness reflects community-reported real-world outcomes from the sentiment analysis.
Category
Muscle Growth
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- One clinical combo study showed significant IGF-1 elevation. Animal and in-vitro data support GH-mediated anabolic effects. Community reports body recomposition with training.
Category
Fat Loss
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- No direct fat loss clinical data for GHRP-2. Theoretical through GH/IGF-1 pathway. Community reports are mixed, confounded by appetite stimulation.
Category
Appetite & Satiety
- Evidence Strength
- 7/10
- Reported Effectiveness
- 8/10
- Summary
- Well-established ghrelin receptor agonism drives appetite. Consistently reported across all community sources. Dose-dependent effect.
Category
Sleep Quality
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- GH secretagogue class shows improved deep sleep in clinical literature (50% longer stage 4 sleep with related compounds). Community reports are generally positive.
Category
Recovery & Healing
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- GH/IGF-1 elevation supports tissue repair mechanistically. Community reports improved post-workout recovery and injury healing.
Category
Physical Performance
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Limited direct evidence. GH elevation supports performance indirectly. Community reports are inconsistent.
Category
Heart Health
- Evidence Strength
- 5/10
- Reported Effectiveness
- N/A
- Summary
- Animal studies show cardioprotective effects via inotropy and anti-fibrotic mechanisms. No human cardiovascular outcome data. Community data not yet collected.
Category
Skin Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- GH/IGF-1 pathway supports collagen synthesis theoretically. Very limited specific data. Community reports tighter, brighter skin.
Category
Hair Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- GH-mediated effect theoretically. Single community report of improved hair/nail growth over extended use.
Category
Fluid Retention
- Evidence Strength
- 6/10
- Reported Effectiveness
- 7/10
- Summary
- Known GH-class effect. Water retention widely and consistently reported in community. Typically resolves over weeks.
Category
Side Effect Burden
- Evidence Strength
- 6/10
- Reported Effectiveness
- 4/10
- Summary
- Well-documented non-selective profile: cortisol, prolactin elevation, appetite, water retention. Heavier than Ipamorelin.
Category
Heart Rate & Palpitations
- Evidence Strength
- 4/10
- Reported Effectiveness
- 3/10
- Summary
- Multiple community reports of elevated resting heart rate. Not well-characterized in clinical literature.
Category
Treatment Adherence
- Evidence Strength
- 5/10
- Reported Effectiveness
- 4/10
- Summary
- Multiple daily injections with fasting requirements create protocol burden. Community frequently cites convenience as reason for switching to alternatives.
Category
Focus & Mental Clarity
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Very limited data. One community report of improved sharpness. GH-mediated cognitive effects are theoretically plausible.
Categories scored: 14
Categories with community data: 14
Categories not scored (insufficient data): Weight Management, Food Noise, Energy Levels, Memory & Cognition, Mood & Wellbeing, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Joint Health, Inflammation, Pain Management, Gut Health, Digestive Comfort, Nausea & GI Tolerance, Blood Pressure, Hormonal Symptoms, Temperature Regulation, Body Image, Immune Function, Bone Health, Longevity & Neuroprotection, Cravings & Impulse Control, Social Connection, Withdrawal Symptoms, Daily Functioning
Benefits & Potential Effects
The Basics
The primary benefit of GHRP-2 is its ability to stimulate your body's own growth hormone production. Unlike injecting synthetic growth hormone directly, this peptide works with your body's existing system, triggering natural GH pulses that your pituitary gland produces and your body regulates through its normal feedback mechanisms. This preserves the natural rhythm and reduces the risk of pushing GH to dangerously high levels.
The downstream effects of increased GH and IGF-1 include several potential benefits. Many users report improved sleep quality, particularly deeper sleep, which in turn supports recovery from exercise and physical stress. Body recomposition (building lean tissue while reducing fat) is a commonly cited goal, though results are gradual and heavily dependent on diet and training. Faster recovery between workouts and from injuries is another frequently reported benefit.
For individuals who struggle to eat enough, the appetite-stimulating effect can be genuinely useful. Unlike most other GH secretagogues that treat appetite increase as a side effect, some GHRP-2 users actively seek this effect to support caloric intake during bulking or recovery from illness.
The compound also shows potential for strengthening the effects of GHRH analogs. When paired with a compound like CJC-1295 (no DAC) or sermorelin, the combined GH response exceeds what either peptide achieves independently.
The Science
Documented benefits of GHRP-2 span several domains supported by varying levels of evidence:
Growth Hormone Elevation: GHRP-2 produces potent, dose-dependent GH release through GHS-R1a agonism. A single 100 mcg subcutaneous dose raises GH levels several-fold above baseline [10]. Sustained administration elevates IGF-1 levels, with approximately 50% increases documented over 3-month treatment periods [11].
Diagnostic Utility: GHRP-2 (as Pralmorelin) is used clinically to evaluate pituitary GH reserve, providing a standardized provocative test for GH deficiency diagnosis [5][10].
Synergistic GH Amplification: When combined with GHRH analogs, GHRP-2 produces synergistic GH release. Bowers et al. (1990) demonstrated that submaximal doses of GHRP combined with GHRH produced supraadditive GH release in healthy men [3]. The combination approach is the basis for most clinical protocols utilizing GHRP-2.
Cytoprotection: Preclinical data demonstrates cardioprotective, neuroprotective, and anti-inflammatory properties through both GHS-R1a and CD36 receptor pathways [12]. GHRP-2 administration in septic patients reduced inflammatory cytokines and restored organ function markers [12].
Sleep Enhancement: The GH secretagogue class broadly demonstrates sleep-enhancing effects. MK-677 studies showed 50% longer stage 4 (deep) sleep and greater than 20% longer REM sleep duration in young men [5][13]. GHRP-2 is expected to share this effect through the common GHS-R1a pathway, though direct GHRP-2 sleep data is limited.
Side Effects & Safety Considerations
The Basics
GHRP-2 carries a heavier side effect burden than Ipamorelin, the more selective peptide in the same family. The most common effects are appetite stimulation (which can be intense shortly after injection), water retention (noticeable puffiness, especially in the first weeks), and transient flushing or warmth at the injection site.
Some users report elevated heart rate after injection, with resting heart rate increasing from typical levels around 70 BPM to around 100 BPM. This effect appears to be dose-related and temporary, but it has led some users to discontinue use or switch to alternatives.
There are also mild hormonal side effects. Unlike Ipamorelin, which releases GH without touching other hormonal axes, GHRP-2 causes small, transient increases in cortisol and prolactin. These elevations are typically described as clinically insignificant at standard doses, but they distinguish GHRP-2 from cleaner alternatives.
With continued daily use, the body's GH response can weaken. This tachyphylaxis is well-documented in clinical literature and is why cycling protocols and periodic breaks are commonly incorporated.
Blood sugar effects are another consideration. Some users report hypoglycemia-like symptoms (weakness, faintness, shakiness) shortly after injection, even when actual blood glucose levels are normal or mildly elevated. This paradoxical response may be related to the ghrelin receptor's role in glucose metabolism.
The Science
The safety profile of GHRP-2 reflects its non-selective GHS-R1a agonism [5][6][7]:
Hormonal Side Effects: Administration of GHRP-2 at standard doses produces transient cortisol elevation and modest prolactin increases, contrasting with ipamorelin which produces no significant elevation of either hormone at equipotent GH-stimulating doses [6][7]. Comparative clinical data demonstrates that GHRP-6 at doses sufficient to stimulate GH release consistently elevates plasma cortisol by 30-50%, while GHRP-2 produces a milder but measurable increase [6].
Appetite Stimulation: As a ghrelin receptor agonist, GHRP-2 activates the same hunger signaling pathway as endogenous ghrelin. This effect is dose-dependent and peaks shortly after administration [1][2].
Water Retention: GH-mediated fluid retention is a class effect of all GH secretagogues. GHRP-2 users commonly report peripheral edema, facial puffiness, and weight gain from water, particularly during initial weeks of use [5].
Tachyphylaxis: Nijland et al. (1998) documented significant GH response attenuation after five consecutive days of subcutaneous GHRP-2 in healthy young men [8]. This finding supports the rationale for cycling protocols and periodic breaks.
Cardiovascular Effects: Heart rate elevation has been reported in community settings but is not well-characterized in published clinical literature. The mechanism may involve GHS-R1a expression in cardiovascular tissue or sympathetic activation secondary to ghrelin-pathway stimulation.
Glycemic Effects: GHRP-2 can produce transient alterations in glucose homeostasis. GH elevation itself has counter-regulatory effects on insulin sensitivity, and ghrelin-pathway activation influences glucose metabolism through hypothalamic circuits [5].
The side effects and contraindications above give you a map of what to watch for. Doserly turns that map into a daily practice. Log the specific biomarkers and symptoms associated with this compound's known risk profile, and the app builds a timeline of how your body is responding across your cycle.
Trending in the wrong direction on a key marker? Noticing a pattern that started two weeks into your protocol? Doserly connects the dots between your protocol timeline and your logged data, making it easier to spot emerging issues early and have informed, data-backed conversations with your healthcare provider about what's working and what needs attention.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
Dosing Protocols
The Basics
Commonly reported GHRP-2 doses range from 100 to 300 mcg per injection. Most sources describe a gradual approach: starting at the lower end (100 mcg once daily) and increasing over several weeks based on tolerance. The target dose for most users appears to be around 200 mcg per injection.
Dosing frequency varies. Conservative protocols use once-daily injection, typically before bed. More aggressive protocols call for two or three injections per day, spaced to take advantage of natural GH pulse windows (morning fasted, pre-workout, and bedtime). The trade-off with more frequent dosing is increased side effects and greater risk of response attenuation.
Timing is important. The peptide should be administered on an empty stomach, with most sources recommending at least two hours of fasting before injection and 30-60 minutes of continued fasting afterward. Insulin spikes from food can significantly blunt the GH response.
Cycle lengths of 8 to 16 weeks are most commonly cited, followed by a 4-6 week break. Some users employ a 5-days-on, 2-days-off pattern within their cycle to help maintain receptor sensitivity.
The Science
Clinical dosing data derives from diagnostic and therapeutic studies:
Diagnostic Use: Pihoker et al. (1995) utilized GHRP-2 at doses ranging from 0.3 to 3.0 mcg/kg administered intravenously and intranasally for GH deficiency evaluation in children [10].
Therapeutic Pediatric Use: GHRP-2 at 5-15 mcg/kg administered two to three times daily sustained growth velocity of approximately 6.0 cm/year over 18-24 months in GH-deficient children [5].
Adult Combination Protocols: Sigalos et al. (2017) used 100 mcg each of sermorelin, GHRP-2, and GHRP-6 administered three times daily subcutaneously in hypogonadal men [11].
Titration Rationale: Gradual titration from 100 mcg upward is supported by the dose-dependent nature of both GH response and side effects. Higher per-injection doses (above 300 mcg) have been studied but may offer diminishing GH returns while increasing tachyphylaxis risk [8].
Standard Gradual Protocol:
Weeks
Weeks 1-2
- Per-Injection Dose
- 100 mcg
- Frequency
- 1-2x daily
Weeks
Weeks 3-4
- Per-Injection Dose
- 150 mcg
- Frequency
- 1-2x daily
Weeks
Weeks 5-8
- Per-Injection Dose
- 200 mcg
- Frequency
- 1-2x daily
Weeks
Weeks 9-12+
- Per-Injection Dose
- 200-300 mcg
- Frequency
- 1-2x daily
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Turn symptom and safety notes into a clearer timeline.
Doserly helps you log doses, symptoms, and safety observations side by side so patterns are easier to discuss with a qualified clinician.
Pattern view
Logs and observations

Pattern visibility is informational and should be reviewed with a clinician.
What to Expect
A general timeline based on available research and community reports. Individual responses vary significantly based on dose, frequency, body composition, age, and whether GHRP-2 is used alone or in combination with a GHRH analog.
Weeks 1-2: The most immediate effects are appetite stimulation after injection, which many users notice from the very first dose. Transient flushing, warmth, or tingling at the injection site may occur. Water retention and mild puffiness often begin within the first week. Sleep quality may improve for some users, though others report initial disruption that resolves over time.
Weeks 3-4: Body composition changes may begin to become noticeable. Users who combine GHRP-2 with resistance training commonly report muscles feeling fuller and more "pumped" throughout the day. Some report improvements in skin quality. The initial water retention typically stabilizes.
Weeks 5-8: This is where the more substantive effects are generally reported. Body recomposition becomes more visible, with users noting reduced fat around the midsection, face, and extremities even when eating at maintenance or surplus. Recovery between training sessions improves. Sleep quality improvements become more consistent for most users.
Weeks 9-16: Extended use may produce further body composition improvements, but the risk of tachyphylaxis increases with continuous daily dosing. Users who incorporate cycling strategies (5 on/2 off, or periodic breaks) tend to report more sustained effects. IGF-1 elevation continues to build with consistent administration.
Post-Cycle: When discontinuing GHRP-2, the most commonly noted immediate change is loss of the appetite stimulation effect. Some water weight loss occurs as fluid retention resolves. GH and IGF-1 levels gradually return toward baseline values over days to weeks.
Interaction Compatibility
Good With (Synergistic Compounds)
- CJC-1295 (no DAC) — GHRH analog that activates the complementary cAMP/PKA pathway. Produces synergistic GH release when combined with GHRP-2. The most studied combination approach.
- Sermorelin — Another GHRH analog with prior FDA approval. The Sigalos 2017 study used sermorelin + GHRP-2 + GHRP-6 in combination [11].
- Tesamorelin — The strongest evidence-backed GHRH analog (FDA-approved). Can be paired with GHRP-2 for GHRH/GHRP synergy.
- BPC-157 — Tissue repair peptide. Community protocols combine it for enhanced recovery support.
- TB-500 — Complementary tissue repair compound frequently stacked for injury recovery protocols.
Not Good With (Contraindicated or Cautionary)
- Hexarelin — Another potent GHS-R1a agonist. Stacking with GHRP-2 would likely produce overlapping receptor activation with amplified side effects (cortisol, prolactin) and increased tachyphylaxis risk.
- GHRP-6 — While used together in the Sigalos 2017 study, stacking two GHRPs simultaneously may compound side effects, particularly appetite and cortisol elevation. The combination is a clinical research protocol, not a standard user approach.
- MK-677 — Oral GHS-R1a agonist with a 24-hour half-life. Combining with GHRP-2 would produce overlapping ghrelin-pathway stimulation with potentially compounded appetite, water retention, and glucose effects.
- Insulin — GH elevation from GHRP-2 has counter-regulatory effects on insulin sensitivity. Combining requires careful glucose monitoring and clinical supervision.
Administration Guide
Materials required: Insulin syringes (U-100, 30- or 50-unit preferred for precision), alcohol swabs, bacteriostatic water for reconstitution, sharps container.
Recommended reconstitution solution: Bacteriostatic water (0.9% benzyl alcohol) is the standard choice, enabling multi-dose vial use over approximately 4 weeks. For a 10 mg vial, adding 3.0 mL of bacteriostatic water produces a concentration of approximately 3.33 mg/mL, where each unit on a U-100 insulin syringe equals approximately 33.3 mcg.
Timing considerations: GHRP-2 is most commonly administered on an empty stomach. Most sources recommend at least two hours without food before administration and 30-60 minutes of continued fasting afterward. Insulin spikes from food intake can significantly blunt the GH response. Bedtime dosing aligns with the body's natural nocturnal GH pulse. When using multiple daily doses, common timing windows include morning fasted, pre-workout (if training fasted), and bedtime.
Post-administration care: Mild flushing, warmth, or tingling at the injection site are normal and transient. Increased appetite typically occurs within 15-30 minutes and subsides within an hour. Users with concerns about blood sugar effects should monitor glucose levels during the initial adjustment period.
Supplies & Planning
The following materials are generally associated with GHRP-2 protocols. Specific quantities depend on your prescribed dose, frequency, and cycle length. Consult your healthcare provider and use the reconstitution calculator for precise planning.
Peptide Vials: GHRP-2 is commonly available in 5 mg and 10 mg lyophilized vial sizes.
Reconstitution Solution: Bacteriostatic water (0.9% benzyl alcohol) in 10 mL bottles. Standard usage is approximately 3.0 mL per vial.
Insulin Syringes: U-100 insulin syringes. For the small volumes typical of GHRP-2 dosing, 30-unit or 50-unit syringes are preferred for improved measurement accuracy over standard 100-unit syringes.
Alcohol Swabs: For cleaning the vial stopper and injection site before each administration. Plan for two per administration session.
Sharps Container: For safe disposal of used syringes. A 1-quart container accommodates approximately 100 syringes.
Storage & Handling
Lyophilized (powder) form:
- Long-term storage: -20°C (-4°F) in dry, dark conditions. Stable for 1+ years.
- Short-term storage: 2-8°C (35.6-46.4°F) for weeks to months.
- Room temperature (~25°C) is acceptable for 3-4 weeks when lyophilized but not recommended for extended periods.
- Allow vials to reach room temperature before opening to prevent condensation from compromising the powder.
- Store in original sealed packaging with desiccant to minimize moisture exposure.
Reconstituted (liquid) form:
- Refrigerate at 2-8°C (35.6-46.4°F) immediately after reconstitution.
- Use within approximately 4 weeks (28 days) for optimal potency.
- Do not freeze reconstituted solution. Freezing causes irreversible peptide degradation.
- Avoid freeze-thaw cycles.
- Inspect before each use for cloudiness, discoloration, or particulate matter. Discard if any abnormalities are observed.
D-amino acid stability advantage: GHRP-2's D-amino acid modifications (D-Ala, D-2-Nal, D-Phe) provide superior enzymatic stability compared to sermorelin and other peptides with exclusively L-amino acid residues. This translates to better shelf stability in both lyophilized and reconstituted forms.
Lifestyle Factors
Getting the most from any GH secretagogue protocol requires attention to the factors that naturally influence your body's growth hormone production and utilization.
Diet: Administer GHRP-2 on an empty stomach (minimum 2 hours fasted) and avoid eating for 30-60 minutes after injection. Insulin spikes from carbohydrate-rich meals blunt the GH response. A protein-forward diet supports the anabolic effects of elevated GH and IGF-1. If appetite stimulation is a concern during cutting phases, planning the dosing window carefully to align with meal timing can help manage intake.
Exercise: Resistance training and aerobic exercise independently stimulate GH release and support the IGF-1 axis. Combining a structured training program with GHRP-2 may produce additive benefits for body composition and recovery. Some users time a dose before training to combine the exercise-induced and peptide-induced GH pulses.
Sleep: Prioritize 7-9 hours of quality sleep. The body's largest natural GH pulse occurs during deep sleep. Bedtime dosing of GHRP-2 is commonly recommended to amplify this natural rhythm. Poor sleep undermines the hormonal benefits of any secretagogue protocol.
Stress Management: Elevated cortisol can blunt the GH response. Since GHRP-2 already produces mild cortisol elevation, managing baseline stress levels through lifestyle modifications may help optimize the net hormonal effect.
Monitoring: Baseline and periodic blood work is advisable when using any GH secretagogue. Key markers include IGF-1, fasting glucose, HbA1c, prolactin, and cortisol. Tracking these values over your cycle provides objective data on how your body is responding.
Regulatory Status & Research Classification
United States (FDA): GHRP-2 has never been approved by the FDA for any indication. It was investigated in Phase I/pharmacokinetic studies but did not advance through the clinical development pipeline. GHRP-2 is classified as a research compound and is not on the FDA's 503A Bulks List for compounding. Its regulatory status for compounding remains in a gray area similar to other GH secretagogues.
Japan: Pralmorelin (the pharmaceutical name for GHRP-2) has been used as a diagnostic agent for evaluating growth hormone deficiency, representing the most established clinical application of this compound.
Canada (Health Canada): No DIN or NPN listing. Not approved for therapeutic use.
United Kingdom (MHRA): Not approved for therapeutic use. Available as a research chemical.
Australia (TGA): Not listed in the Australian Register of Therapeutic Goods. Classification would likely fall under Schedule 4 (prescription only) or higher.
European Union (EMA): No marketing authorization. Research use only.
WADA Status: GHRP-2 is prohibited at all times under the World Anti-Doping Agency's Prohibited List as a growth hormone secretagogue. GHRP-2 metabolites have been identified in doping control analyses, and glycine-modified growth hormone secretagogues (including GHRP-2 analogs) have been identified in seized doping materials [5][14].
Active Clinical Trials: No currently active clinical trials registered on ClinicalTrials.gov specifically for GHRP-2 therapeutic applications as of 2026.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is the difference between GHRP-2, GHRP-6, and Ipamorelin?
All three are growth hormone releasing peptides that work through the ghrelin receptor (GHS-R1a), but they differ in selectivity and side effect profiles. Based on available data, GHRP-6 (first generation) produces the strongest appetite stimulation and the most off-target hormonal effects. GHRP-2 (second generation) is more potent for GH release with milder side effects than GHRP-6. Ipamorelin (third generation) offers the cleanest profile, releasing GH without measurable effects on cortisol, prolactin, or appetite, but some sources describe it as slightly less potent. A healthcare professional can help determine which compound best matches specific goals and risk tolerance.
Does GHRP-2 need to be combined with a GHRH analog?
GHRP-2 works on its own, but research consistently demonstrates synergistic GH release when combined with a GHRH analog such as CJC-1295 (no DAC) or sermorelin. The combination activates two complementary pathways simultaneously. This synergistic principle, established by Bowers (1990) and quantified by Veldhuis and Bowers (2009), forms the basis for most clinical protocols using GH secretagogues. Whether to use GHRP-2 alone or in combination is a decision to discuss with a healthcare provider.
How long does it take to see results from GHRP-2?
Based on available community data and research, some effects are felt immediately (appetite stimulation, sometimes flushing). Sleep quality changes and improved recovery are commonly reported within the first 1-2 weeks. Visible body composition changes typically require 4-8 weeks of consistent use combined with appropriate diet and exercise. IGF-1 elevation builds progressively, with significant increases documented over 3+ months of regular administration.
Will GHRP-2 show up on a drug test?
Standard employment drug panels do not test for peptides. However, WADA prohibits all growth hormone secretagogues in competitive sport. Specialized anti-doping tests can detect GH peptide metabolites, and GHRP-2 has specifically been identified in doping control analyses. Anyone subject to athletic anti-doping testing should assume GHRP-2 is both banned and detectable.
Why do some users switch from GHRP-2 to Ipamorelin?
The most commonly cited reasons in community discussions are side effects. GHRP-2's appetite stimulation, water retention, and occasional cortisol/prolactin elevation lead some users to prefer Ipamorelin's cleaner profile, particularly those focused on cutting or body composition goals where increased appetite is counterproductive. Users who value GHRP-2's appetite stimulation for bulking or who want maximum GH potency tend to stay with it.
Can GHRP-2 affect blood sugar levels?
Based on available data, GHRP-2 can transiently affect glucose homeostasis. GH elevation has counter-regulatory effects on insulin sensitivity, and ghrelin-pathway activation influences glucose metabolism. Some community members report hypoglycemia-like symptoms (weakness, faintness) shortly after injection, though measured blood glucose may be normal or mildly elevated. Individuals with diabetes or glucose sensitivity should discuss this with their healthcare provider before considering any GH secretagogue.
Sources & References
[1] Pralmorelin (GHRP-2). Wikipedia entry covering mechanism of action, ghrelin receptor agonism, and physiological effects. https://en.wikipedia.org/wiki/Pralmorelin
[2] Growth hormone response to GHRP-2. PubMed Central (PMC3297037). Pituitary and hypothalamic mechanisms of GH release stimulation. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3297037/
[3] Bowers CY et al. "On the in vitro and in vivo activity of a new synthetic hexapeptide that acts on the pituitary to specifically release growth hormone." Journal of Clinical Endocrinology & Metabolism. 1990;70(4):975-982. PubMed 2108187. https://pubmed.ncbi.nlm.nih.gov/2108187/
[4] Veldhuis JD, Bowers CY. "Determinants of joint GH-releasing hormone and GH-releasing peptide synergy in man." American Journal of Physiology -- Endocrinology and Metabolism. 2009;296(5):E1085-E1092. PubMed 19240251. https://pubmed.ncbi.nlm.nih.gov/19240251/
[5] Sigalos JT, Pastuszak AW. "The Safety and Efficacy of Growth Hormone Secretagogues." Sexual Medicine Reviews. 2018;6(1):45-53. PubMed 28400207 / PMC5632578. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5632578/
[6] Arvat E et al. "Endocrine activities of ghrelin, a natural growth hormone secretagogue, in humans: comparison and interactions with hexarelin, a nonnatural peptidyl GH secretagogue, and GH-releasing hormone." Journal of Clinical Endocrinology & Metabolism. 2001;86(3):1169-1174. PubMed 9285939. https://pubmed.ncbi.nlm.nih.gov/9285939/
[7] Sinha DK et al. "Beyond the androgen receptor: the role of growth hormone secretagogues in the modern management of body composition in hypogonadal males." Translational Andrology and Urology. 2020;9(Suppl 2):S149-S159. PMC7108996. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7108996/
[8] Nijland EA et al. "Five-day treatment with daily subcutaneous GHRP-2: Response attenuation and IGF-I effects in healthy young men." European Journal of Endocrinology. 1998. https://pubmed.ncbi.nlm.nih.gov/
[9] Kim KS et al. "Twice-daily GHRP-2 effects on IGF-1 and tachyphylaxis patterns." Asian-Australasian Journal of Animal Sciences. 2003.
[10] Pihoker C et al. "Diagnostic studies with intravenous and intranasal growth hormone-releasing peptide-2 in children of short stature." Journal of Clinical Endocrinology & Metabolism. 1995;80(10):2987-2992. https://pubmed.ncbi.nlm.nih.gov/7559884/
[11] Sigalos JT et al. "Growth Hormone Secretagogue Treatment in Hypogonadal Men Raises Serum Insulin-Like Growth Factor-1 Levels." American Journal of Men's Health. 2017;11(6):1752-1757. PubMed 28830317 / PMC5675260. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5675260/
[12] Berlanga-Acosta J et al. "Synthetic Growth Hormone-Releasing Peptides (GHRPs): A Historical Appraisal of the Evidences Supporting Their Cytoprotective Effects." Clinical Medicine Insights: Cardiology. 2017;11:1179546817694558. PMC5392015. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5392015/
[13] Nass R et al. "Effects of an Oral Ghrelin Mimetic on Body Composition and Clinical Outcomes in Healthy Older Adults: A Randomized Trial." Annals of Internal Medicine. 2008;149(9):601-611. PMC2757071. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2757071/
[14] Seki Y, Ichihara A. "Association between overweight and growth hormone secretion in patients with non-functioning pituitary tumors." 2022. https://pubmed.ncbi.nlm.nih.gov/
Related Peptide Guides
- Ipamorelin — Third-generation GHRP with the cleanest selectivity profile. The most common alternative to GHRP-2.
- GHRP-6 — First-generation GHRP with stronger appetite stimulation and broader hormonal effects.
- CJC-1295 — GHRH analog frequently combined with GHRP-2 for synergistic GH release.
- Sermorelin — GHRH analog with prior FDA approval, used in the Sigalos 2017 combination study.
- Tesamorelin — FDA-approved GHRH analog with the strongest clinical evidence for visceral fat reduction.
- MK-677 — Oral GHS-R1a agonist with 24-hour half-life. Alternative for those who prefer oral dosing.
- Hexarelin — Most potent acute GH secretagogue but limited by rapid tachyphylaxis.
- BPC-157 — Tissue repair peptide commonly stacked with GH secretagogues for recovery.
- TB-500 — Complementary healing peptide often combined in recovery-focused protocols.
Need the reconstitution math for GHRP-2: Complete Research Guide?
Open the calculator with GHRP-2: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.