GHRP-6: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Growth Hormone-Releasing Peptide-6, SKF 110679, U 75799E, Hexapeptide-2, His-D-Trp-Ala-Trp-D-Phe-Lys-NH2
Attribute
Administration
- Detail
- Injectable (subcutaneous)
Attribute
Research Status
- Detail
- Research Compound. No FDA approval. Phase I/PK studies in humans only. WADA prohibited (S2 category).
Attribute
Typical Dose Range
- Detail
- 100-300 mcg per injection, three times daily (300-900 mcg total daily)
Attribute
Half-Life
- Detail
- Approximately 20 minutes (plasma elimination)
Attribute
Cycle Length
- Detail
- 8-12 weeks on, with 1-2 week breaks between cycles
Attribute
Storage
- Detail
- Lyophilized: -20°C long-term or 2-8°C short-term; Reconstituted: 2-8°C, use within 28 days
Overview / What Is GHRP-6?
The Basics
GHRP-6 is a synthetic peptide made of six amino acids that tells your pituitary gland to release growth hormone. It does this by mimicking ghrelin, the natural hunger hormone that your stomach produces when you haven't eaten. This ghrelin mimicry is why the single most noticeable effect of GHRP-6 is a dramatic increase in appetite, typically within 15-30 minutes of administration.
Developed in the 1980s as one of the earliest growth hormone releasing peptides, GHRP-6 is considered a first-generation compound in its class. It works, but it is not selective. Along with triggering growth hormone release, it also causes transient spikes in cortisol and prolactin, two hormones that later, more refined peptides like ipamorelin were specifically designed to avoid touching.
People are drawn to GHRP-6 for a few reasons. It stimulates growth hormone release without requiring exogenous growth hormone injections, it preserves the body's natural feedback controls, and for those who struggle with low appetite (hardgainers, individuals recovering from illness, or those with eating disorders), the appetite-stimulating effect can be genuinely therapeutic. It has also attracted interest from researchers studying cardioprotection and wound healing, though this work remains largely preclinical.
The trade-off is clear: GHRP-6 offers reliable growth hormone stimulation at the cost of more side effects and a more demanding dosing schedule than newer alternatives.
The Science
GHRP-6 (Growth Hormone-Releasing Peptide-6) is a synthetic hexapeptide first characterized in the 1980s as part of Cyril Bowers' pioneering work on growth hormone secretagogues [1]. It functions as a potent agonist of the growth hormone secretagogue receptor type 1a (GHS-R1a), the endogenous receptor for ghrelin. Its amino acid sequence (His-D-Trp-Ala-Trp-D-Phe-Lys-NH2) incorporates two D-amino acid substitutions (D-tryptophan and D-phenylalanine) that confer enzymatic resistance and enhanced biological activity relative to L-amino acid configurations [2].
GHRP-6 stimulates pulsatile growth hormone secretion from anterior pituitary somatotrophs while maintaining physiological negative feedback through the somatostatin system [2]. This distinguishes it mechanistically from exogenous recombinant growth hormone, which bypasses pituitary regulation entirely.
Beyond its endocrine effects, GHRP-6 exhibits cytoprotective properties through a secondary receptor interaction with CD36, a scavenger receptor expressed on immune cells, cardiac tissue, and muscle [3]. This dual receptor activity underlies the compound's documented cardioprotective and tissue-protective effects in preclinical models. It also acts as an antagonist to the chemokine receptor CCR5, suggesting potential immunomodulatory properties that have not been fully characterized [2].
GHRP-6 is classified as a first-generation GHRP, alongside GHRP-2 and hexarelin. Third-generation compounds like ipamorelin were developed specifically to address GHRP-6's non-selective activation profile, which includes transient elevation of cortisol and prolactin [4].
Molecular Identity
Attribute
Common Names
- Detail
- GHRP-6, Growth Hormone-Releasing Peptide-6, SKF 110679, U 75799E, Hexapeptide-2
Attribute
Amino Acid Sequence
- Detail
- His-D-Trp-Ala-Trp-D-Phe-Lys-NH2 (H-D-W-A-W-D-F-K-NH2)
Attribute
Molecular Formula
- Detail
- C46H56N12O6
Attribute
Molecular Weight
- Detail
- 873.0 g/mol (free base); 1053.2 g/mol (acetate salt)
Attribute
CAS Number
- Detail
- 160320-04-3 (free base); 145177-42-0 (acetate)
Attribute
PubChem CID
- Detail
- 4345065
Attribute
Structural Type
- Detail
- Linear hexapeptide with C-terminal amidation
Attribute
D-Amino Acids
- Detail
- D-Trp (position 2), D-Phe (position 5)
Attribute
Functional Class
- Detail
- Ghrelin receptor (GHS-R1a) agonist; growth hormone secretagogue; appetite stimulant
Attribute
Salt Forms
- Detail
- Acetate salt (most common), free base
Mechanism of Action
The Basics
Your body has a built-in system for releasing growth hormone in pulses throughout the day, with the largest pulses occurring during deep sleep. GHRP-6 amplifies this system by copying the signal that ghrelin, your natural hunger hormone, sends to the pituitary gland.
Think of it like pressing the gas pedal on your growth hormone engine. GHRP-6 binds to the same receptor that ghrelin uses (the ghrelin receptor) on cells in your pituitary gland, triggering them to release a burst of growth hormone. Unlike injecting growth hormone directly, which floods your system and shuts down your own production, GHRP-6 works with your body's existing controls. When growth hormone levels get high enough, a braking system (somatostatin) kicks in to prevent overproduction.
GHRP-6 also has a second, less well-known effect. It interacts with a receptor called CD36 found on heart cells, immune cells, and muscle tissue. Through this pathway, it appears to protect cells from damage caused by oxidative stress and inflammation. This is why researchers have studied it for cardioprotection and wound healing, even though these applications remain experimental.
The appetite effect is not a side effect in the pharmacological sense. It is a direct consequence of GHRP-6 activating the ghrelin receptor, which is the body's primary hunger signal. This makes GHRP-6 unique among growth hormone peptides: it reliably stimulates both GH release and appetite simultaneously.
The Science
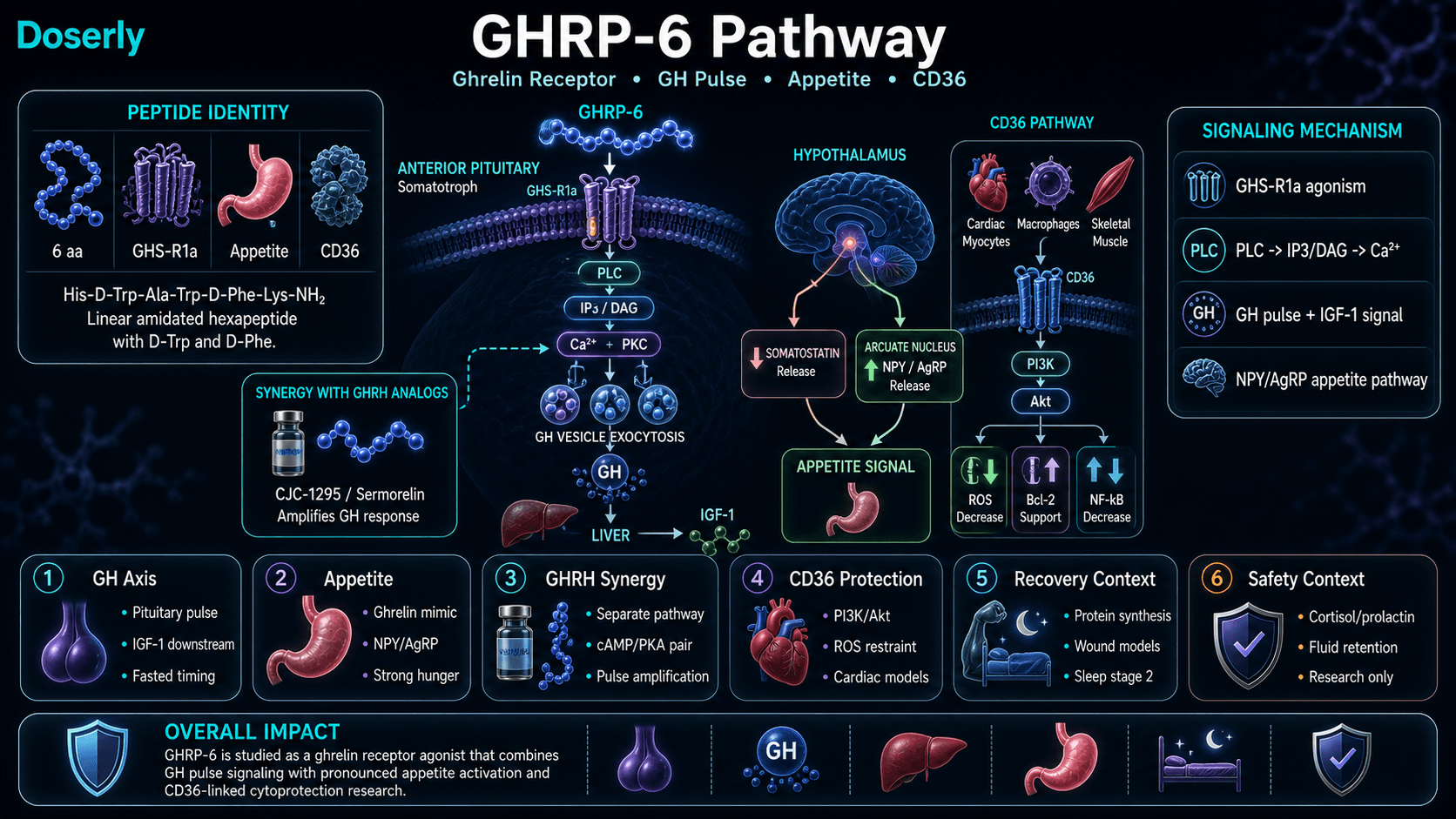
GHRP-6 exerts its primary endocrine effects through agonism of the growth hormone secretagogue receptor type 1a (GHS-R1a), a G-protein coupled receptor expressed predominantly on somatotroph cells of the anterior pituitary gland [1][2]. Receptor binding triggers phospholipase C (PLC) activation, generating inositol triphosphate (IP3) and diacylglycerol (DAG), leading to intracellular calcium mobilization and protein kinase C (PKC) activation. This signaling cascade converges on secretory granule exocytosis, producing acute pulsatile growth hormone release [2].
Simultaneously, GHRP-6 suppresses somatostatin secretion from the hypothalamus, reducing the tonic inhibitory brake on GH release and amplifying the secretory pulse amplitude [2]. This dual action (direct pituitary stimulation plus somatostatin suppression) distinguishes GHRPs from GHRH analogs, which act solely through cAMP/PKA signaling at the GHRH receptor.
The GHS-R1a pathway engaged by GHRP-6 (PLC/PKC/calcium) is mechanistically distinct from the GHRH receptor pathway (cAMP/PKA). When both pathways are activated simultaneously, the intracellular signals converge on somatotroph secretory mechanisms in a multiplicative rather than additive manner [1][5]. Bowers et al. demonstrated that submaximal doses of GHRP combined with GHRH produced synergistic GH release in healthy men, with Veldhuis and Bowers quantifying the magnitude: GHRP-2 alone produced a 47-fold increase in pulsatile GH secretion, GHRH alone a 20-fold increase, and the combination a 54-fold increase [1][5].
GHRP-6 also interacts with the CD36 receptor (cluster of differentiation 36), a scavenger receptor expressed on cardiac myocytes, macrophages, and skeletal muscle cells [3]. This secondary pathway activates PI3K/Akt cell-survival signaling cascades, conferring cytoprotective effects independent of growth hormone elevation. Documented downstream effects include suppression of reactive oxygen species (ROS) production, upregulation of Bcl-2 anti-apoptotic proteins, downregulation of NFkB-mediated inflammatory signaling, and inhibition of CTGF-driven fibrosis through PPARgamma activation [3].
The orexigenic (appetite-stimulating) effect of GHRP-6 is mediated through GHS-R1a activation in hypothalamic arcuate nucleus neurons, where it mimics endogenous ghrelin's stimulation of neuropeptide Y (NPY) and agouti-related peptide (AgRP) expression [6]. This effect is pharmacologically inseparable from GH secretion at the receptor level, which is why GHRP-6 reliably stimulates both appetite and GH release.
Pathway Visualization Image
Pharmacokinetics
The Basics
GHRP-6 works fast and clears out fast. After a subcutaneous injection, it reaches peak levels in your blood within minutes and is largely eliminated within about 20 minutes. This very short active window is why most protocols involve three injections per day, spaced several hours apart, to maintain a pattern of repeated growth hormone pulses rather than a single spike.
The short half-life is actually by design. Growth hormone is naturally released in pulses, not as a steady stream. GHRP-6's rapid clearance means each injection triggers a distinct GH pulse that rises and falls, mimicking your body's natural rhythm. A compound that stayed active for hours would produce a constant, non-physiological elevation that could disrupt feedback controls.
Timing matters for effectiveness. Blood sugar and insulin levels can blunt the GH response, which is why administration on an empty stomach (at least two hours after eating, with a 30-minute wait before the next meal) is commonly cited as important for maximizing the effect.
The Science
GHRP-6 demonstrates rapid pharmacokinetic characteristics consistent with its small peptide structure (873 Da) and D-amino acid modifications [2][7].
Following subcutaneous administration, GHRP-6 is absorbed rapidly with peak plasma concentrations (Tmax) occurring within 5-20 minutes [7]. The plasma elimination half-life is approximately 20 minutes, necessitating multiple daily administrations to maintain pulsatile GH stimulation [2][7]. This short half-life reflects both proteolytic degradation and renal clearance, though the D-amino acid substitutions at positions 2 and 5 confer some resistance to aminopeptidases relative to all-L-amino acid peptides.
Pharmacodynamic studies demonstrate that GHRP-6 can restore GH responsiveness in populations with blunted secretion, including obese subjects, producing GH surges approximately twice as large as GHRH alone [8]. The GH secretory response is dose-dependent across the 100-300 mcg range in healthy male volunteers, with diminishing returns at higher doses consistent with receptor saturation [7].
The compound's GH-releasing effect is significantly attenuated by concurrent food intake, particularly carbohydrates and fats, which elevate blood glucose and insulin [9]. This pharmacokinetic-pharmacodynamic interaction underlies the clinical emphasis on fasted administration.
Transient elevation of ACTH and cortisol occurs within 15-60 minutes post-injection, returning to baseline within 2-3 hours [10]. This neuroendocrine side effect distinguishes GHRP-6 from selective GHS-R1a agonists like ipamorelin, which do not produce significant cortisol elevation even at supraphysiological doses [4].
The half-life and clearance data above tells you how long the compound stays active, but what does that mean for your daily schedule? Doserly's pharmacokinetic tools let you plug in your dose and frequency to see a projected concentration timeline, helping you understand when you're at peak levels and when the compound has largely cleared.
This becomes especially useful when titrating. If you're increasing your dose gradually, the estimator shows how each step changes your projected peak and trough levels, giving you and your healthcare provider concrete data to discuss at check-ins rather than relying on subjective feel alone.
Keep multi-step protocols organized from start to finish.
Use Doserly to map compounds, timing, cycle windows, notes, and review points so complex protocols stay readable in one place.
Plan view
Protocol schedule
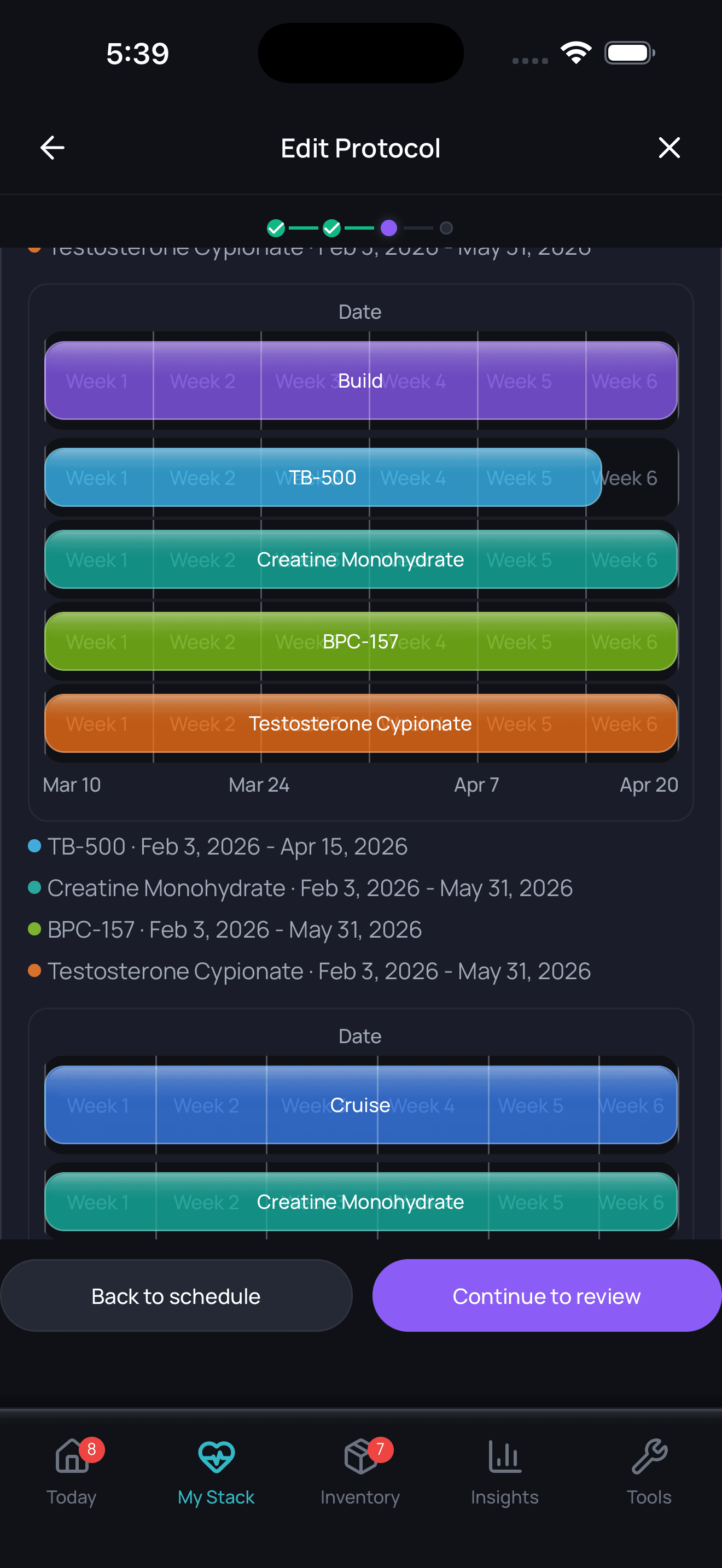
Planning views are organizational and should be aligned with professional guidance.
Research & Clinical Evidence
Growth Hormone Secretion
The Basics
The core evidence for GHRP-6 centers on its ability to make the pituitary gland release growth hormone. This is well-documented in human studies, though the body of clinical evidence is limited to early-phase pharmacokinetic and pharmacodynamic studies rather than large clinical trials. GHRP-6 has never progressed beyond Phase I studies in formal drug development.
The most cited human combination study followed 14 men with low testosterone who received GHRP-6, GHRP-2, and sermorelin together, each at 100 mcg three times daily. Over approximately 134 days, their IGF-1 levels rose by about 50% (from 159.5 to 239.0 ng/mL), and their testosterone levels also increased. Notably, their LH and FSH levels did not change, meaning the peptides did not suppress the body's own testosterone-producing signals [11].
The Science
GHRP-6's growth hormone secretory effects have been characterized in multiple human pharmacokinetic studies [7][10]. Dose-response relationships demonstrate significant GH elevation at doses of 100-300 mcg administered subcutaneously [7].
The only published clinical combination study (Sigalos et al., 2017) evaluated sermorelin (100 mcg) + GHRP-2 (100 mcg) + GHRP-6 (100 mcg) administered three times daily in 14 hypogonadal men on concurrent testosterone therapy [11]. Mean IGF-1 increased from 159.5 to 239.0 ng/mL (P<0.0001) over approximately 134 days. Free testosterone also increased significantly after 90 days. LH and FSH levels remained unchanged, indicating preservation of pituitary gonadotropin function. The study was retrospective with significant attrition (14 compliant patients from 105 initially enrolled), and results were confounded by concurrent testosterone therapy [11].
Cardioprotection
The Basics
One of the more surprising findings about GHRP-6 comes from animal studies on heart protection. In multiple preclinical models, GHRP-6 demonstrated the ability to protect heart tissue from damage caused by chemotherapy drugs, reduced blood flow, and other stressors. In one model using doxorubicin (a chemotherapy drug known to damage the heart), animals treated with GHRP-6 had an 84% survival rate compared to 42% for the control group [3].
These effects appear to work through a separate pathway from the growth hormone mechanism, involving a receptor called CD36 found on heart cells. This means the cardioprotective benefit may be independent of GH elevation. However, none of this work has been confirmed in human clinical trials.
The Science
GHRP-6's cardioprotective properties are mediated primarily through CD36 receptor interactions rather than GHS-R1a-dependent GH release [3]. In preclinical models of doxorubicin-induced cardiomyopathy, GHRP-6 administration achieved 84% survival versus 42% in placebo groups through activation of prosurvival PI3K/Akt signaling cascades [3][12].
In hamster models of dilated cardiomyopathy (TO-2 strain), combined GHRP-6 and GHRP-2 treatment prevented ventricular dilation, restored ejection fraction, and extended lifespan [3]. The cardioprotective mechanism involves positive inotropic effects (increased cardiac contractility) through calcium mobilization without associated chronotropic effects (no heart rate increase), a pharmacologically favorable profile [3].
Anti-fibrotic effects have been demonstrated through PPARgamma-mediated downregulation of connective tissue growth factor (CTGF), reducing myocardial scar formation post-infarction [3].
Wound Healing and Anti-Scarring
The Basics
Research has also examined GHRP-6 for wound healing, with studies suggesting it may help prevent excessive scarring. One study found that GHRP-6 reduced hypertrophic (raised, thickened) scar formation in a skin wound model, potentially by reducing the inflammation and fibrosis that drive abnormal scar tissue growth [13].
The Science
GHRP-6 has demonstrated anti-hypertrophic scarring properties in preclinical cutaneous wound models. Proteomic analysis revealed that treated wounds showed downregulated fibrotic markers (including CTGF and TGF-beta signaling intermediaries) and upregulated tissue remodeling factors, consistent with its established anti-fibrotic mechanism via CD36/PPARgamma activation [13].
Sleep Effects
The Basics
Human studies have shown that GHRP-6 can influence sleep architecture. Specifically, it appears to increase the duration of stage 2 sleep (light sleep) without significantly disrupting REM sleep. Some users report that sleep feels somewhat deeper, though this is not a primary reason people use GHRP-6.
The Science
In a study of normal male subjects, GHRP-6 administration stimulated increases in GH, ACTH, and cortisol alongside measurable changes in sleep architecture, specifically increased stage 2 NREM sleep duration without major disruption of REM sleep patterns [10].
Biomarker Evidence Matrix
Category
Appetite & Satiety
- Evidence Strength
- 7/10
- Reported Effectiveness
- 9/10
- Summary
- Mechanistically established ghrelin mimicry; universally reported by users. The most consistent signal for this compound.
Category
Muscle Growth
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Indirect via GH/IGF-1 elevation; no direct muscle-specific human trials. Community reports modest gains with confounding factors.
Category
Fat Loss
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- GH elevation theoretically supports lipolysis, but appetite stimulation counteracts fat loss goals. Most users report it is not suitable for cutting.
Category
Sleep Quality
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- One human study demonstrates stage 2 sleep effects [10]. Some community reports of modestly deeper sleep.
Category
Recovery & Healing
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- GH/IGF-1 elevation supports tissue repair; preclinical wound healing data. Community reports are sparse and confounded.
Category
Physical Performance
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- No direct human performance studies. Community attributes improvements primarily to appetite-enabled caloric surplus.
Category
Heart Health
- Evidence Strength
- 6/10
- Reported Effectiveness
- 5/10
- Summary
- Strong preclinical evidence for cardioprotection via CD36 pathway [3]. No human cardiac studies. Community awareness is low.
Category
Fluid Retention
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Consistently reported side effect. Generally manageable but present in most users. Direction: negative.
Category
Side Effect Burden
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- Well-characterized non-selective profile (cortisol, prolactin elevation). More side effects than ipamorelin but generally tolerable.
Category
Hormonal Symptoms
- Evidence Strength
- 5/10
- Reported Effectiveness
- 4/10
- Summary
- Transient cortisol and prolactin elevation documented in human PK studies [10]. Confirmed by community blood work reports. Direction: negative.
Category
Treatment Adherence
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- TID fasting protocol is widely reported as burdensome. Higher dropout than simpler protocols. Direction: negative.
Category
Nausea & GI Tolerance
- Evidence Strength
- 3/10
- Reported Effectiveness
- 6/10
- Summary
- Limited reports; occasional nausea mentioned. Generally well-tolerated GI-wise.
Category
Mood & Wellbeing
- Evidence Strength
- 2/10
- Reported Effectiveness
- 5/10
- Summary
- Mechanistic argument for acute neuroprotective/mood effects via pulsatile GHSR activation. No experiential community data.
Category
Longevity & Neuroprotection
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Theoretical neuroprotective benefit from pulsatile (vs. chronic) ghrelin receptor activation. Preclinical only.
Categories not scored (insufficient data): Weight Management, Food Noise, Energy Levels, Focus & Mental Clarity, Memory & Cognition, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Joint Health, Inflammation, Pain Management, Gut Health, Digestive Comfort, Skin Health, Hair Health, Blood Pressure, Heart Rate & Palpitations, Temperature Regulation, Body Image, Immune Function, Bone Health, Cravings & Impulse Control, Social Connection, Withdrawal Symptoms, Daily Functioning
Benefits & Potential Effects
The Basics
GHRP-6's benefits fall into two main categories: what the growth hormone elevation does for your body, and what the appetite stimulation does for people who need it.
On the growth hormone side, the elevated GH and IGF-1 levels can support muscle maintenance and modest growth, improved recovery from training or injury, potential fat metabolism benefits (though the hunger effect often works against this), and the general anti-aging associations that come with healthy growth hormone levels.
The appetite effect is the standout feature. For people who genuinely struggle to eat enough, whether due to medical conditions, treatment side effects, or simply being a "hardgainer" who can't consume enough calories to grow, GHRP-6 provides powerful, reliable appetite stimulation within minutes of each dose. This is not subtle. Users consistently describe it as intense, overwhelming hunger.
There is also preliminary evidence from animal studies for cardioprotective effects, wound healing support, and anti-fibrotic properties, though none of these have been validated in human clinical trials.
The Science
The therapeutic profile of GHRP-6 encompasses several documented and potential effects:
Growth Hormone Axis Activation: Consistent elevation of circulating GH and downstream IGF-1, supporting anabolic processes including nitrogen retention, protein synthesis, and body composition optimization [2][7][11]. The pulsatile release pattern preserves physiological feedback, distinguishing it from exogenous GH administration.
Orexigenic Effect: Pronounced appetite stimulation via hypothalamic GHS-R1a activation, mimicking endogenous ghrelin signaling through NPY/AgRP neuronal pathways [6]. Onset typically occurs within 15-30 minutes post-injection. This property has clinical relevance for cachexia, anorexia, and conditions involving involuntary weight loss.
Cytoprotection: CD36-mediated activation of PI3K/Akt survival signaling, with documented cardioprotective, neuroprotective, and tissue-protective effects in preclinical models [3][12]. Anti-fibrotic effects via PPARgamma-dependent CTGF suppression are relevant to post-injury tissue remodeling.
Sleep Modulation: Documented increases in stage 2 NREM sleep duration in human subjects, with potential implications for recovery quality [10].
Side Effects & Safety Considerations
The Basics
GHRP-6 has a broader side effect profile than newer growth hormone peptides, and understanding these effects is important for anyone considering it.
The most prominent effect is appetite stimulation. While some users welcome this, others find it disruptive, especially those using GHRP-6 for body composition goals. The hunger kicks in within 15-30 minutes and can be intense enough to derail dietary plans if not anticipated.
Water retention is commonly reported. Users describe looking "fuller" but sometimes "puffy," particularly in the face and extremities. This is generally manageable with adequate hydration and electrolyte balance but can be cosmetically noticeable.
GHRP-6 causes transient increases in cortisol and prolactin, hormones that newer peptides like ipamorelin were specifically designed to avoid elevating. These increases are temporary (returning to baseline within a few hours) and generally clinically insignificant at standard doses, but they represent a meaningful disadvantage compared to more selective alternatives.
Injection site irritation is occasionally reported, and some users describe mild nausea, particularly early in use. No serious adverse events have been reported in human studies at standard doses.
The Science
GHRP-6's non-selective GHS-R1a agonism produces several documented off-target effects:
Cortisol Elevation: Administration at growth hormone-stimulating doses consistently elevates plasma cortisol concentrations by 30-50%, with levels returning to baseline within 2-3 hours [4][10]. While transiently insignificant in most individuals, chronic cortisol cycling three times daily warrants monitoring in populations susceptible to HPA axis dysregulation.
Prolactin Elevation: Modest prolactin increases have been documented, raising theoretical concerns about gynecomastia or libido changes with chronic use, though clinical significance at standard doses has not been established [2][4]. One community report confirmed elevated prolactin on blood work during GHRP-6 use.
Fluid Retention: Water retention is consistently reported and likely reflects growth hormone-mediated sodium reabsorption in the renal tubules. The effect is dose-dependent and generally resolves with electrolyte management.
Appetite Stimulation: The orexigenic effect is pharmacologically inseparable from GH release at the receptor level. It is a direct agonist action, not an off-target side effect, though it is unwanted for some use cases [6].
Glucose Metabolism: Growth hormone secretagogues can transiently affect insulin sensitivity. Monitoring HbA1c and fasting glucose is warranted during extended protocols [2].
Comparative Safety Profile: In head-to-head pharmacological comparisons, ipamorelin at equipotent GH-stimulating doses produces no significant cortisol, prolactin, or appetite elevation, establishing it as the preferred first-line GHS-R1a agonist for most applications [4].
Side effect profiles are most useful when you can compare them against your own experience in real time. Doserly lets you log symptoms, severity, and timing alongside your dosing data, creating a side-by-side view of your protocol and your body's response.
This kind of systematic tracking catches things that memory alone misses. A subtle mood shift that began three days after a dose increase. Sleep disruption that correlates with evening administration. These patterns become visible when the data is laid out on a timeline, and they give your healthcare provider actionable information rather than vague concerns. Early detection of emerging side effects means earlier intervention.
Connect protocol changes to labs and health markers.
Doserly can keep lab results, biomarkers, symptoms, and dose history close together so follow-up conversations have better context.
Insights
Labs and trends

Doserly organizes data; it does not diagnose or interpret labs for you.
Dosing Protocols
The Basics
GHRP-6 protocols typically involve subcutaneous injections three times per day, spaced at least 3-4 hours apart. The most commonly cited dose is 100 mcg per injection (300 mcg total daily), with some sources noting doses up to 300 mcg per injection (900 mcg total daily) as an upper practical limit.
The three-times-daily schedule is driven by the peptide's very short half-life of about 20 minutes. Each injection triggers a distinct growth hormone pulse, and spacing them throughout the day creates a pattern of repeated pulses that more closely mimics natural GH secretion.
Timing relative to food is important. Sources consistently recommend administration on an empty stomach, at least two hours after the last meal, with a 30-minute wait before eating afterward. Elevated blood sugar and insulin can significantly reduce the growth hormone response.
Common timing patterns include morning (upon waking), midday, and bedtime. The bedtime dose aligns with the body's largest natural GH pulse during deep sleep.
Most protocols suggest an 8-12 week cycle, with some sources recommending a 1-2 week break before repeating.
The Science
Published dosing data derives from Phase I pharmacokinetic studies in healthy male volunteers [7]. Dose-response relationships are well-characterized across the 100-300 mcg subcutaneous range:
Protocol Level
Standard
- Dose per Injection
- 100 mcg
- Frequency
- 3x daily
- Total Daily
- 300 mcg/day
Protocol Level
Moderate
- Dose per Injection
- 150-200 mcg
- Frequency
- 3x daily
- Total Daily
- 450-600 mcg/day
Protocol Level
Advanced
- Dose per Injection
- 200-300 mcg
- Frequency
- 3x daily
- Total Daily
- 600-900 mcg/day
The three-times-daily frequency reflects the compound's approximately 20-minute plasma half-life [7]. Multiple daily administrations are more effective than single daily dosing for sustained pulsatile GH elevation [2].
Fasting requirement: Elevated blood glucose attenuates GHRP-6-induced GH release. Administration should occur on an empty stomach (minimum 2-3 hours postprandial), with food intake delayed at least 30 minutes post-injection to allow peak GH response [9].
Combination protocols: When administered with a GHRH analog (such as sermorelin or modified GRF 1-29), synergistic GH release has been documented at doses of 100 mcg each per injection [1][5][11]. The only published human combination study used 100 mcg each of sermorelin, GHRP-6, and GHRP-2 administered three times daily [11].
Cycle duration: Most sources suggest 8-12 weeks of continuous use, followed by a 1-2 week washout period. Desensitization has not been clearly demonstrated for GHRP-6 at standard doses when administered in divided daily doses, though the evidence base for long-term continuous use is limited [2].
The dosing protocols above involve numbers that matter: specific microgram amounts, reconstitution ratios, and timing windows. Getting any of these wrong compounds across every subsequent dose from that vial.
Doserly's dose and reconstitution calculators eliminate the guesswork. Enter your vial size, peptide amount, and target dose, and get the exact bacteriostatic water volume, units per tick mark, and doses per vial. The injection site tracker maps your administration history as a visual heat map across your body, flagging areas that need rest and suggesting rotation patterns. Combined with dose reminders that include compound name, amount, and route, every aspect of your daily protocol is handled with the precision it requires.
Track injection timing, draw notes, and site rotation.
Doserly helps keep syringe-related notes, injection site history, reminders, and reconstitution context together for easier review.
Injection log
Site rotation
Injection logs support record-keeping; follow clinician instructions for administration.
What to Expect
The following timeline reflects commonly reported experiences and is not a guarantee of individual results. Response varies based on dose, individual physiology, diet, training, and concurrent compounds.
Week 1-2:
The appetite effect is typically the first thing noticed, often from the very first dose. Intense hunger within 15-30 minutes of injection is the hallmark early response. Some users report mild injection site irritation and slight water retention during this period. Sleep may feel marginally deeper.
Week 3-4:
Appetite stimulation remains strong. Some users report early body composition changes, particularly if the increased caloric intake is paired with structured training. Water retention stabilizes. The three-times-daily injection schedule either becomes routine or is identified as a long-term adherence challenge.
Week 5-8:
If GH/IGF-1 elevation is occurring (confirmable via blood work), downstream effects on recovery, body composition, and training capacity may become noticeable. Strength and muscle fullness improvements are reported by some users, though these are difficult to attribute solely to GHRP-6 when stacking with other compounds or optimizing diet.
Week 8-12:
Continued use at standard doses. Most sources suggest evaluating results and considering a washout period. The appetite effect typically does not diminish with continued use. Users report that the compound "does what it says" but is not transformative on its own; results are proportional to diet, training, and overall protocol quality.
Interaction Compatibility
Good With (Synergistic)
- Sermorelin — GHRH analog; activates the complementary cAMP/PKA pathway for synergistic GH release when combined with GHRP-6's PLC/PKC pathway. This is the most well-supported combination in published research [1][5][11].
- CJC-1295 — Modified GHRH analog (both DAC and no-DAC variants). Provides sustained GHRH stimulus to complement GHRP-6's pulsatile action. Widely used in clinical practice though the specific CJC-1295 no-DAC + GHRP-6 combination lacks published human trial data.
- GHRP-2 — Fellow GHS-R1a agonist with slightly different receptor activation profile. Used alongside GHRP-6 in the Sigalos et al. triple combination study [11].
- Ipamorelin — Selective third-generation GHRP. Some practitioners combine with GHRP-6 as part of GHRP rotation strategies, though using both simultaneously offers limited theoretical advantage over either alone.
Not Good With (Caution Advised)
- MK-677 — Oral ghrelin mimetic with 24-hour half-life. Combining with GHRP-6 would produce redundant GHS-R1a activation with compounding side effects (appetite, cortisol, prolactin, water retention) without proportional additional benefit.
- Hexarelin — Strongest acute GH secretagogue but develops tachyphylaxis (rapid desensitization) and has the worst selectivity profile. Combining with GHRP-6 amplifies cortisol and prolactin elevation.
- Insulin — GHRP-6 effects are attenuated by insulin. Concurrent insulin administration may blunt the GH response and creates hypoglycemia risk.
- Somatostatin analogs — Directly antagonize GHRP-6's mechanism by suppressing GH release.
Administration Guide
Materials required:
- U-100 insulin syringes (29-31 gauge, 0.5 mL or 1.0 mL)
- Alcohol swabs (70% isopropyl)
- Bacteriostatic water for reconstitution
- Sharps disposal container
Recommended reconstitution solution: Bacteriostatic water (0.9% benzyl alcohol preserved) is the standard reconstitution solution for GHRP-6. Common reconstitution volumes for a 5 mg vial include 2.5 mL (yielding 2.0 mg/mL, where 1 unit on a U-100 syringe equals 20 mcg). For readers who need help with reconstitution calculations, Doserly's reconstitution calculator can determine the exact volumes for any vial size and target concentration.
Timing considerations:
- Administer on an empty stomach (minimum 2-3 hours after the last meal)
- Wait at least 30 minutes after administration before eating
- Space injections at least 3-4 hours apart (morning, midday, bedtime is the most common schedule)
- Evening doses align with the body's natural nocturnal GH pulse
- Anticipate strong appetite within 15-30 minutes; have appropriate food prepared in advance
Post-administration care:
- Appetite onset is rapid and intense. Having a planned, portion-controlled meal ready for the 30-minute post-administration window can prevent unstructured eating.
- Rotate injection sites systematically to prevent lipohypertrophy
- Monitor for injection site irritation, which is occasionally reported
- Use new sterile syringes for each administration
Supplies & Planning
The following materials are generally associated with GHRP-6 protocols. Specific quantities depend on the dose, frequency, and cycle length determined in consultation with a healthcare provider.
Peptide vials: GHRP-6 is commonly available in 2 mg, 5 mg, and 10 mg lyophilized vials. Vial size selection affects reconstitution concentration and doses available per vial. Use the Doserly reconstitution calculator to determine the optimal setup for your protocol.
Reconstitution supplies:
- Bacteriostatic water (10 mL bottles)
- Sterile syringes for drawing bacteriostatic water
Injection supplies:
- U-100 insulin syringes (29-31 gauge). For small volumes (under 10 units), 30-unit or 50-unit syringes provide better measurement precision.
- Alcohol swabs (two per injection: one for vial stopper, one for injection site)
- Sharps disposal container
Storage:
- Freezer access for long-term lyophilized storage
- Refrigerator space for reconstituted vials
Storage & Handling
Lyophilized (powder) form:
- Long-term: Store at -20°C (-4°F) or colder for maximum stability (up to 2-3 years)
- Short-term: 2-8°C (35.6-46.4°F) is acceptable for weeks to months
- Room temperature (~25°C) is acceptable for 3-4 weeks when the powder remains sealed
- Keep in a dry, dark environment; GHRP-6 is hygroscopic and light-sensitive
- Allow vials to reach room temperature before opening to prevent condensation
Reconstituted (liquid) form:
- Refrigerate at 2-8°C (35.6-46.4°F) immediately after reconstitution
- Use within 28 days when reconstituted with bacteriostatic water
- Do not freeze reconstituted solutions
- Avoid repeated freeze-thaw cycles
- Inspect for clarity before each use; discard if cloudy, discolored, or if particles are visible
Stability notes:
GHRP-6 demonstrates superior stability compared to larger peptides like sermorelin due to its D-amino acid modifications (D-Trp and D-Phe), which confer resistance to enzymatic degradation. The acetate salt form is the most common commercially available preparation.
Lifestyle Factors
Getting the most from GHRP-6 requires attention to several lifestyle factors that directly influence how the compound performs:
Diet: The appetite-stimulating effect is the dominant lifestyle consideration. If body composition improvement is a goal, having structured meals prepared before each dose prevents the intense post-injection hunger from leading to unplanned, low-quality food choices. For individuals using GHRP-6 specifically for weight gain, the appetite effect is the primary therapeutic feature. A protein-forward diet supports the anabolic effects of elevated GH/IGF-1.
Fasting discipline: The 2-3 hour pre-injection fast and 30-minute post-injection wait are not optional recommendations. Blood glucose and insulin levels meaningfully attenuate the GH response. Integrating these windows into a daily routine is essential for consistent results.
Training: Resistance training and aerobic activity complement the anabolic and metabolic adaptations supported by GH elevation. GHRP-6 is not a substitute for training stimulus; it amplifies the body's response to the stimulus you provide.
Sleep: Growth hormone is naturally released in its largest pulses during deep sleep. Prioritizing 7-9 hours of quality sleep, with the final GHRP-6 dose timed before bed, may optimize the compounding effect of endogenous and peptide-stimulated GH release.
Monitoring: Blood work to track IGF-1, fasting glucose, HbA1c, and prolactin levels is warranted during extended use. This provides objective data on whether the compound is producing the intended endocrine effects and helps identify any emerging issues early.
Regulatory Status & Research Classification
United States (FDA):
GHRP-6 has never been approved by the FDA for any therapeutic indication. It has not progressed beyond Phase I/pharmacokinetic studies in formal drug development. It is not currently on the FDA's Category 2 Bulks List (which would prohibit compounding), but it also lacks a positive nomination for the 503A Bulks List. Its compounding status exists in regulatory uncertainty.
Canada (Health Canada):
GHRP-6 does not hold a Drug Identification Number (DIN) or Natural Health Product classification. It is available through some compounding pharmacies under prescriber authority.
United Kingdom (MHRA):
Not approved for therapeutic use. Available through some peptide suppliers as a research compound.
Australia (TGA):
Not approved for therapeutic use. Would likely fall under Schedule 4 (prescription only) classification if formally reviewed.
European Union (EMA):
No marketing authorization has been sought or granted for GHRP-6.
WADA Status:
GHRP-6 is prohibited at all times under WADA Section S2 (Peptide Hormones, Growth Factors, Related Substances, and Mimetics). Glycine-modified growth hormone secretagogues, including analogues of GHRP-6, have been identified in seized doping material [14]. Specialized anti-doping tests can detect GHRP-6 metabolites.
Active Clinical Trials:
No clinical trials specifically evaluating GHRP-6 as a therapeutic agent are currently registered on ClinicalTrials.gov. The compound has been used in published pharmacokinetic and pharmacodynamic studies but has not entered efficacy-focused clinical development.
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is GHRP-6 and how does it differ from other growth hormone peptides?
GHRP-6 is a synthetic hexapeptide that stimulates growth hormone release by activating the ghrelin receptor (GHS-R1a) on pituitary cells. It is considered a first-generation growth hormone releasing peptide. Compared to newer compounds like ipamorelin, GHRP-6 produces broader hormonal effects including transient cortisol and prolactin elevation, along with pronounced appetite stimulation. These off-target effects are the primary reason many practitioners prefer ipamorelin for general growth hormone optimization.
How intense is the appetite increase?
Based on community reports, the appetite effect is consistently described as powerful and rapid, typically onset within 15-30 minutes of administration. Users frequently characterize it as intense, overwhelming hunger that is meaningfully stronger than normal hunger signals. The effect does not appear to diminish with continued use. For individuals specifically seeking appetite stimulation (such as those recovering from illness or struggling with low appetite), this is the primary therapeutic feature. For those focused on fat loss, it represents a significant practical challenge.
Can GHRP-6 be used for fat loss?
Based on available data, GHRP-6 is generally not considered an ideal choice for fat loss protocols. While GH elevation theoretically supports lipolysis, the pronounced appetite-stimulating effect makes caloric restriction substantially more difficult. Most sources and community reports suggest compounds like ipamorelin, AOD-9604, or tesamorelin for fat-loss-oriented GH optimization. A healthcare professional can help determine the most appropriate option.
Does GHRP-6 need to be taken on an empty stomach?
Available research indicates that food intake, particularly carbohydrates and fats, significantly attenuates GHRP-6's growth hormone releasing effect by elevating blood glucose and insulin levels. Most sources recommend a minimum 2-3 hour fast before administration and a 30-minute wait before eating afterward. This timing requirement, repeated three times daily, is one of the practical challenges of GHRP-6 protocols.
Is GHRP-6 safe?
In published human pharmacokinetic studies, no serious adverse events have been reported at standard doses. However, the safety database is limited to small, short-term Phase I studies. Long-term safety data from controlled trials does not exist. Known effects include transient cortisol and prolactin elevation, water retention, and appetite changes. Individuals with diabetes, active malignancies, or pituitary disorders should discuss specific contraindications with a healthcare professional.
How does GHRP-6 compare to MK-677?
MK-677 (ibutamoren) is an oral, non-peptide ghrelin receptor agonist with a 24-hour half-life, contrasting with GHRP-6's approximately 20-minute half-life. MK-677 provides continuous GHS-R1a activation from a once-daily oral dose, while GHRP-6 produces pulsatile activation from three daily injections. Some researchers have raised concerns that chronic (continuous) ghrelin receptor activation from MK-677 may have different neurological implications than the pulsatile pattern produced by short-acting GHRPs, though this remains theoretical. MK-677 also has a more substantial clinical evidence base, including a 2-year RCT.
Is GHRP-6 detectable on drug tests?
GHRP-6 is prohibited by WADA and can be detected by specialized anti-doping tests. GHRP-6 metabolites and analogues have been identified in seized doping material. Anyone subject to athletic anti-doping testing should assume GHRP-6 and all growth hormone secretagogues are banned and detectable.
Sources & References
[1] Bowers CY et al. "On the in vitro and in vivo activity of a new synthetic hexapeptide that acts on the pituitary to specifically release growth hormone." Journal of Clinical Endocrinology & Metabolism. 1990;70(4):975-982. https://pubmed.ncbi.nlm.nih.gov/2108187/
[2] Sigalos JT, Pastuszak AW. "The Safety and Efficacy of Growth Hormone Secretagogues." Sexual Medicine Reviews. 2018;6(1):45-53. https://pmc.ncbi.nlm.nih.gov/articles/PMC5632578/
[3] Berlanga-Acosta J et al. "Synthetic Growth Hormone-Releasing Peptides (GHRPs): A Historical Appraisal of the Evidences Supporting Their Cytoprotective Effects." Clinical Medicine Insights: Cardiology. 2017;11:1179546817694558. https://pmc.ncbi.nlm.nih.gov/articles/PMC5392015/
[4] Raun K et al. "Ipamorelin, the first selective growth hormone secretagogue." European Journal of Endocrinology. 1998;139(5):552-561. https://pubmed.ncbi.nlm.nih.gov/9849822/
[5] Veldhuis JD, Bowers CY. "Determinants of joint GH-releasing hormone and GH-releasing peptide synergy in man." American Journal of Physiology - Endocrinology and Metabolism. 2009;296(5):E1085-E1092. https://pubmed.ncbi.nlm.nih.gov/19240251/
[6] Asakawa A et al. "Ghrelin is an appetite-stimulatory signal from stomach with structural resemblance to motilin." Gastroenterology. 2001;120(2):337-345. https://pubmed.ncbi.nlm.nih.gov/11159873/
[7] Garcia JM, Polvino WJ. "Pharmacokinetic study of growth hormone-releasing peptide 6 (GHRP-6) in healthy male volunteers." European Journal of Pharmaceutical Sciences. 2013;48(1-2):40-46. https://pubmed.ncbi.nlm.nih.gov/23085206/
[8] Cordido F et al. "Massive growth hormone (GH) discharge in obese subjects after the combined administration of GH-releasing hormone and GHRP-6: evidence for a marked somatotroph secretory capability in obesity." Journal of Clinical Endocrinology & Metabolism. 1993;76(4):819-823. https://pubmed.ncbi.nlm.nih.gov/8473390/
[9] Penalva A et al. "Effect of nutrient intake on the growth hormone-releasing effect of GH-releasing peptide-6." Clinical Medicine Insights: Cardiology. 2017.
[10] Frieboes RM et al. "Growth hormone-releasing peptide-6 stimulates sleep, growth hormone, ACTH, and cortisol release in normal man." Neuroendocrinology. 1995;61(5):584-589. https://pubmed.ncbi.nlm.nih.gov/7617137/
[11] Sigalos JT et al. "Growth Hormone Secretagogue Treatment in Hypogonadal Men Raises Serum Insulin-Like Growth Factor-1 Levels." American Journal of Men's Health. 2017;11(6):1752-1757. https://pmc.ncbi.nlm.nih.gov/articles/PMC5675260/
[12] Berlanga-Acosta J et al. "GHRP-6 prevents doxorubicin-induced myocardial and extra-myocardial damage." Peptides. 2017.
[13] Mendoza-Mari Y et al. "GHRP-6 prevents cutaneous hypertrophic scarring: a proteome study." International Wound Journal. 2018;15(3):416-425.
[14] Arvat E et al. "Endocrine activities of ghrelin, a natural growth hormone secretagogue, in humans: comparison and interactions with hexarelin, a nonnatural peptidyl GH secretagogue, and GH-releasing hormone." Journal of Clinical Endocrinology & Metabolism. 2001;86(3):1169-1174. https://pubmed.ncbi.nlm.nih.gov/9285939/
Related Peptide Guides
- GHRP-2 — Second-generation GHRP with improved selectivity over GHRP-6
- Ipamorelin — Third-generation selective GHS-R1a agonist; no cortisol/prolactin elevation
- Sermorelin — GHRH analog; complementary pathway for synergistic GH release
- CJC-1295 — Modified GHRH analog (with and without DAC variants)
- Hexarelin — Strongest acute GH secretagogue; rapid tachyphylaxis
- MK-677 — Oral non-peptide ghrelin mimetic; 24-hour half-life
- Tesamorelin — FDA-approved GHRH analog; strongest clinical evidence for visceral fat reduction
- AOD-9604 — HGH fragment for lipolysis without IGF-1 elevation
- IGF-1 LR3 — Direct IGF-1 analog; downstream effector of GH signaling
- PEG-MGF — Mechano growth factor for muscle repair
Need the reconstitution math for GHRP-6: Complete Research Guide?
Open the calculator with GHRP-6: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.