LL-37: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- CAP-18, Human Cathelicidin, hCAP18 C-terminal fragment, CAMP gene product
Attribute
Administration
- Detail
- Injectable (subcutaneous), Topical (cream, gel, wound dressing)
Attribute
Research Status
- Detail
- Research compound. Not FDA-approved for therapeutic use. Phase II clinical trials completed for topical wound healing. WADA Prohibited.
Attribute
Typical Dose Range
- Detail
- Topical: 0.5-1.6 mg/mL; Injectable (subcutaneous): 50-400 mcg/day
Attribute
Half-Life
- Detail
- Estimated 30 minutes to 2 hours (limited human PK data; see Pharmacokinetics section for conflict detail)
Attribute
Cycle Length
- Detail
- 4-16 weeks depending on indication and route
Attribute
Storage
- Detail
- Lyophilized: -20°C, stable ~24 months; Reconstituted: 2-8°C, use within 4 weeks
Overview / What Is LL-37?
The Basics
LL-37 is your body's own antibiotic. It is the only cathelicidin antimicrobial peptide that humans produce, and it serves as a first line of defense against bacteria, viruses, and fungi. The name comes from its structure: 37 amino acids long, starting with two leucines (L-L).
Think of LL-37 as a multitool for immune defense. It can punch holes in bacterial cell walls, neutralize bacterial toxins before they cause harm, break apart the protective biofilms that make chronic infections so stubborn, and recruit immune cells to where they are needed most. Unlike conventional antibiotics that target one organism in one way, LL-37 works through multiple mechanisms simultaneously, which makes it much harder for pathogens to develop resistance.
What makes LL-37 particularly interesting is its connection to vitamin D. Your body ramps up LL-37 production when vitamin D levels are adequate, which is one of the clearest explanations for why vitamin D status matters so much for immune function [1]. People with chronically low vitamin D often have reduced LL-37 levels, potentially leaving them more vulnerable to infections.
The clinical interest in LL-37 centers on wound healing and infection control. Two randomized controlled trials have demonstrated accelerated healing of chronic venous leg ulcers and diabetic foot ulcers when LL-37 was applied topically [2][3]. Beyond wound care, researchers are studying its potential in biofilm-related infections, antimicrobial resistance, and immune modulation.
An important caveat: LL-37 is a double-edged sword. The same immune-activating properties that fight infections can trigger or worsen inflammatory and autoimmune conditions when the peptide is present in excess or applied systemically. This dual nature means LL-37 requires more caution and specificity than many other peptides in the research space.
The Science
LL-37 (LLGDFFRKSKEKIGKEFKRIVQRIKDFLRNLVPRTES) is the sole human cathelicidin antimicrobial peptide, derived from the C-terminal cleavage of the 18 kDa precursor protein hCAP18 (human cationic antimicrobial protein 18), encoded by the CAMP gene [1][4]. The mature peptide is released primarily by neutrophil specific granules, but also by macrophages, keratinocytes, and epithelial cells lining the respiratory, gastrointestinal, and genitourinary tracts [4][5].
The peptide adopts an amphipathic alpha-helical conformation in membrane-mimetic environments, with a net charge of +6 at physiological pH. This cationic character enables selective binding to anionic microbial membranes (enriched in phosphatidylglycerol and lipopolysaccharide) while largely sparing mammalian cell membranes (enriched in zwitterionic phosphatidylcholine and cholesterol) [4][6].
LL-37 expression is transcriptionally regulated by 1,25-dihydroxyvitamin D3 (calcitriol) through a vitamin D response element (VDRE) in the CAMP gene promoter, establishing a direct molecular link between vitamin D status and antimicrobial peptide production [1]. This pathway was characterized by Liu et al. (2006), who demonstrated that toll-like receptor 2/1 (TLR2/1) activation in monocytes upregulates the vitamin D receptor (VDR) and 1-alpha-hydroxylase (CYP27B1), leading to intracrine vitamin D signaling and subsequent cathelicidin induction [1].
Dysregulation of LL-37 expression has been implicated in the pathogenesis of psoriasis (where LL-37-self-DNA complexes activate plasmacytoid dendritic cells via TLR9, driving type I interferon production), rosacea (elevated protease processing yielding inflammatory cathelicidin fragments), and atherosclerosis (LL-37 accumulation within plaques causing smooth muscle cell injury) [5][7].
Molecular Identity
Attribute
Common Names
- Detail
- LL-37, CAP-18, Human Cathelicidin, hCAP18 fragment
Attribute
Amino Acid Sequence
- Detail
- LLGDFFRKSKEKIGKEFKRIVQRIKDFLRNLVPRTES (37 amino acids)
Attribute
Molecular Formula
- Detail
- C₂₀₅H₃₄₀N₆₀O₅₃
Attribute
Molecular Weight
- Detail
- 4,493.33 Da
Attribute
CAS Number
- Detail
- 154947-66-7
Attribute
Target Receptor
- Detail
- FPRL1 (FPR2) / direct membrane disruption
Attribute
Net Charge
- Detail
- +6 at physiological pH
Attribute
Structure
- Detail
- Amphipathic alpha-helix in membrane environments
Attribute
Solubility
- Detail
- Sterile water, bacteriostatic water
Attribute
Gene
- Detail
- CAMP (cathelicidin antimicrobial peptide)
Mechanism of Action
The Basics
LL-37 works through several complementary mechanisms, which is why researchers describe it as "multifunctional" rather than just an antimicrobial agent.
Its most direct action is killing microbes. LL-37 is positively charged, while bacterial cell membranes carry a negative charge. This electrostatic attraction pulls the peptide toward bacteria like a magnet, where it inserts into the membrane and forms pores that cause the bacterial cell to leak its contents and die. This membrane-disruption approach works against a wide range of organisms, including drug-resistant bacteria, fungi, and enveloped viruses [4][6].
Beyond direct killing, LL-37 dismantles biofilms. These are the protective slime layers that bacteria build around themselves, making chronic infections (like those in wounds, sinuses, or the urinary tract) extremely difficult to treat with conventional antibiotics. LL-37 can both prevent biofilm formation and break apart existing biofilms [8].
LL-37 also acts as an immune messenger. It binds to a receptor called FPRL1 (also known as FPR2) on immune cells, essentially sending out a "come here" signal that recruits neutrophils, monocytes, and T cells to the site of an infection [5]. It also neutralizes lipopolysaccharide (LPS), a bacterial toxin that triggers severe inflammatory responses and can lead to septic shock [4][6].
For wound healing specifically, LL-37 promotes the migration of skin cells (keratinocytes) across wound beds and stimulates the growth of new blood vessels (angiogenesis), both of which accelerate tissue repair [2][3].
The Science
LL-37 exerts antimicrobial activity through a barrel-stave and carpet model of membrane disruption. The amphipathic alpha-helical structure (residues 2-31 form the primary helical domain) enables the peptide to bind anionic lipid headgroups, insert into the hydrophobic core of the bilayer, and form oligomeric pores of approximately 1.8 nm diameter. At concentrations above the critical micelle concentration (approximately 1-5 mcM depending on membrane composition), toroidal pore formation results in rapid dissipation of transmembrane potential and cell lysis [4][6].
Biofilm disruption operates through multiple mechanisms: LL-37 prevents initial bacterial adhesion to surfaces, inhibits the quorum-sensing signaling that coordinates biofilm maturation, and degrades the extracellular polysaccharide matrix of established biofilms at sub-bactericidal concentrations (0.5-4 mcg/mL) [8].
Immunomodulatory activity is mediated through several parallel pathways:
- FPRL1/FPR2 activation: Chemotaxis of neutrophils, monocytes, and CD4+ T cells to infection sites [5]
- LPS neutralization: Direct binding of the lipid A moiety of lipopolysaccharide, blocking CD14/TLR4-mediated NF-kappaB activation and suppressing TNF-alpha release [4][6]
- Neutrophil microvesicle induction: In murine sepsis models, LL-37 stimulated neutrophils to release antimicrobial protein-rich microvesicles, reducing bacterial burden and improving survival [9]
- Autophagy induction: The di-leucine motif (positions 1-2) triggers autophagy in macrophages via beclin-1-dependent pathways, enhancing intracellular pathogen clearance [10]
Wound healing effects involve upregulation of keratinocyte migration through transactivation of the epidermal growth factor receptor (EGFR) and stimulation of angiogenesis via VEGF-independent pathways. In clinical wound models, these effects translated to enhanced granulation tissue formation and accelerated re-epithelialization [2][3].
Critically, LL-37 can form complexes with self-DNA and self-RNA, converting these normally inert molecules into potent activators of plasmacytoid dendritic cells via TLR9 and TLR7/8 respectively. This pathway drives type I interferon production and is implicated in the pathogenesis of psoriasis and systemic lupus erythematosus [5][7].
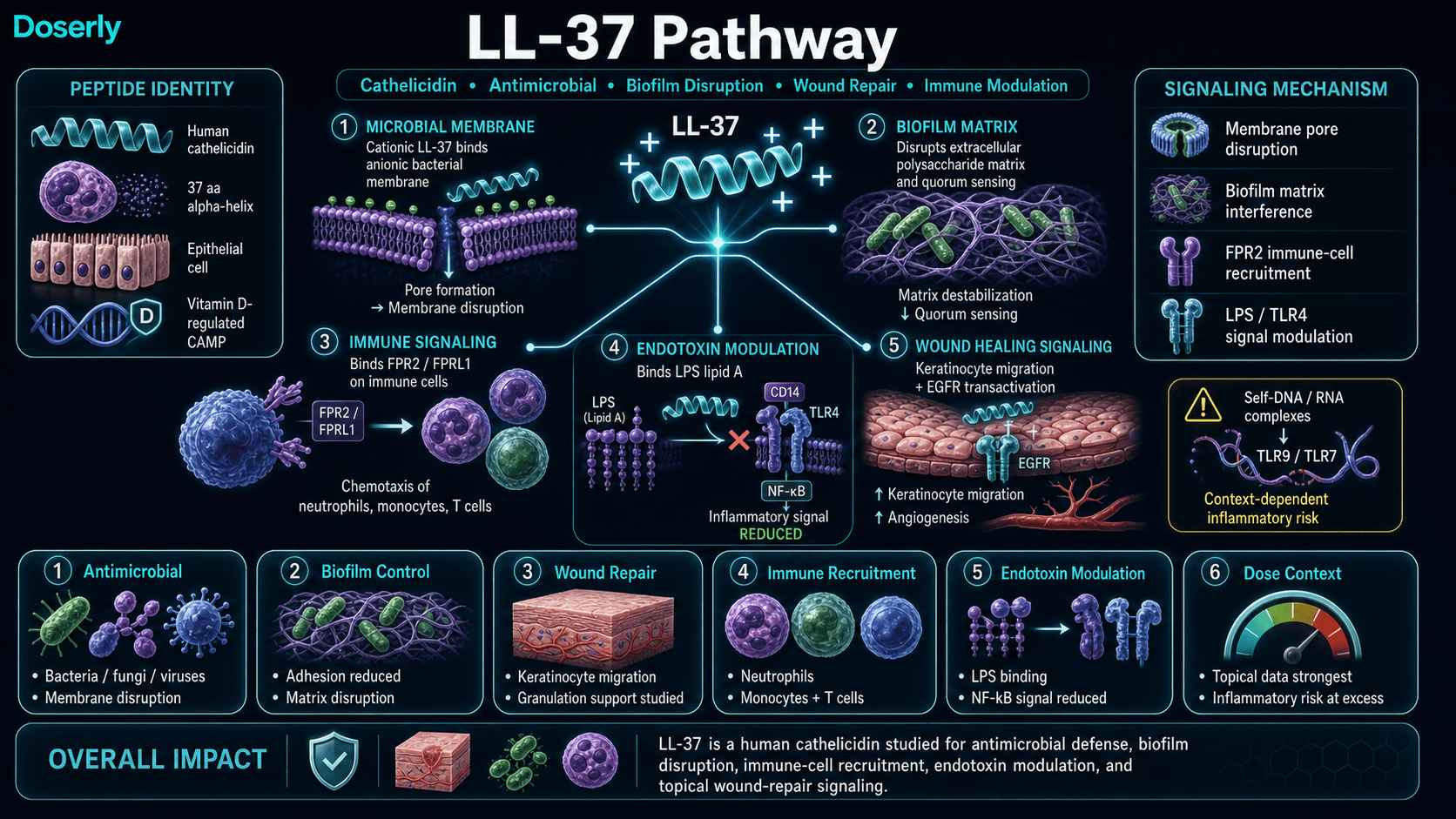
Pathway Visualization Image
Pharmacokinetics
The Basics
LL-37 is cleared from the bloodstream relatively quickly, though sources disagree on exactly how quickly. Some data suggests a plasma half-life of around 30 minutes, while other estimates range up to 2 hours. This difference likely reflects distinct measurement approaches: how long the peptide itself is detectable in blood versus how long its biological effects persist in tissue.
In practical terms, this short activity window explains why most subcutaneous protocols call for daily dosing. Topical application is a different story: when LL-37 is applied directly to a wound or skin surface, local concentrations persist much longer than systemic levels would suggest because the peptide remains active at the application site.
LL-37 is susceptible to degradation by proteases in blood and tissue fluids, which limits its systemic duration of action. This is one reason why topical delivery (where the peptide reaches its target directly without needing to survive the bloodstream) has shown stronger clinical results than injectable routes [2][3].
Reaching peak effect happens quickly, likely within 30 minutes of either subcutaneous injection or topical application. The rapid onset matches the peptide's role in innate immunity, where speed is essential for first-line defense.
The Science
Pharmacokinetic characterization of LL-37 in humans remains limited. Available data derives primarily from preclinical models and inference from clinical trial observations.
Absorption and onset: Following subcutaneous injection, LL-37 demonstrates rapid absorption with an estimated Tmax of approximately 30 minutes. The amphipathic alpha-helical structure facilitates interaction with tissue membranes upon injection, with rapid distribution to local tissue compartments [4].
Distribution: LL-37 binds plasma proteins including albumin and lipoproteins, which may modulate its bioavailability and tissue distribution. The cationic charge promotes accumulation at negatively charged tissue interfaces, including damaged endothelium and inflamed mucosal surfaces [5].
Metabolism and elimination: Primary degradation occurs through proteolytic cleavage by serine proteases (neutrophil elastase, proteinase 3) and metalloproteinases in plasma and tissue fluids. Plasma elimination half-life estimates range from 30 minutes to 2 hours depending on the assay methodology and biological matrix studied [4]. Local tissue effects, particularly in wound environments where protease inhibitor concentrations are elevated, likely persist beyond the plasma half-life.
Dose-response considerations: The therapeutic window for LL-37 is notably narrow compared to many peptides. At concentrations of 1-10 mcM, selective antimicrobial and immunomodulatory effects predominate. Above 10-25 mcM, cytotoxicity toward host cells becomes significant, with membrane disruption affecting eukaryotic cells including keratinocytes, epithelial cells, and vascular smooth muscle cells [5][7]. This concentration-dependent transition from therapeutic to toxic explains the dose sensitivity consistently reported in community experience.
Research & Clinical Evidence
LL-37 and Wound Healing
The Basics
Wound healing is the most clinically validated application of LL-37. Two randomized controlled trials have tested topical LL-37 in chronic wounds that had resisted standard treatment.
In patients with venous leg ulcers (wounds on the lower legs caused by poor circulation), LL-37 applied twice weekly for 13 weeks significantly accelerated healing compared to placebo. The researchers found that these chronic wounds were deficient in natural LL-37, suggesting the treatment was essentially replacing a missing repair signal [2].
A separate trial tested LL-37 cream on diabetic foot ulcers, where it improved granulation tissue formation (the new tissue that fills wound beds) and wound closure rates [3]. These results are encouraging because diabetic wounds are notoriously difficult to heal and represent a major clinical burden.
The Science
Heilborn et al. (2003) demonstrated reduced LL-37 expression in chronic wound fluid compared to acute wound fluid, establishing a biological rationale for exogenous supplementation [2]. The chronic wound microenvironment appears to suppress endogenous cathelicidin production, creating a local deficiency in both antimicrobial defense and pro-healing signaling.
A Phase II/IIb multicenter randomized controlled trial (n=34) evaluated topical LL-37 at 0.5 and 1.6 mg/mL concentrations applied twice weekly during dressing changes for venous leg ulcers over 13 weeks with follow-up to 4 months. Treatment at 0.5 mg/mL demonstrated 6-fold higher healing rate constants versus placebo in predefined subgroups, with favorable safety (adverse events comparable to placebo) [2].
A double-blind RCT evaluated LL-37 cream at 0.5 mg/mL (and 1.6 mg/mL in some cohorts) applied twice weekly for 4 weeks for diabetic foot ulcers. Accelerated granulation tissue formation and wound closure metrics were observed, without clear reduction in inflammatory cytokines at the wound site [3]. This suggests the healing mechanism may operate through direct pro-migratory and angiogenic effects rather than anti-inflammatory pathways.
LL-37 and Antimicrobial Activity
The Basics
LL-37 has demonstrated activity against a remarkably broad range of pathogens in laboratory studies. This includes gram-positive bacteria (like Staphylococcus aureus, including MRSA), gram-negative bacteria (like E. coli and Pseudomonas), fungi (like Candida), and enveloped viruses [4][6].
What sets LL-37 apart from conventional antibiotics is its mechanism. Because it physically disrupts microbial membranes rather than targeting a specific biochemical pathway, bacteria have a much harder time developing resistance. A 2019 study demonstrated greater than 4-log reduction in MRSA biofilm, outperforming several conventional antibiotics [8].
The Science
Vandamme et al. (2012) published a comprehensive review establishing LL-37's broad-spectrum antimicrobial activity, with minimum inhibitory concentrations (MICs) typically in the 1-50 mcg/mL range across gram-positive and gram-negative species [4]. Antimicrobial activity is salt-sensitive and can be reduced at physiological NaCl concentrations, though synergistic effects with other host defense peptides and conventional antibiotics partially compensate [4][6].
Anti-biofilm activity operates at sub-MIC concentrations (0.5-4 mcg/mL), with demonstrated efficacy against P. aeruginosa, S. aureus (including MRSA), and mixed-species biofilms relevant to chronic wound infections [8]. The mechanism involves disruption of the extracellular polysaccharide matrix, interference with bacterial quorum-sensing pathways, and prevention of initial surface adhesion.
Antiviral activity has been demonstrated in vitro against influenza A, HIV-1, herpes simplex, and SARS-CoV-2, primarily through envelope disruption and interference with viral entry mechanisms [4].
LL-37 and Sepsis/Endotoxemia
The Basics
In animal models of sepsis (severe bloodstream infection), LL-37 treatment reduced bacterial counts and improved survival. The mechanism works on two fronts: directly killing bacteria and neutralizing LPS, the bacterial toxin that drives the dangerous inflammatory cascade in sepsis [9].
The Science
In a murine sepsis model, exogenous LL-37 administration induced neutrophils to release microvesicles enriched in antimicrobial proteins, creating a secondary wave of host defense independent of direct peptide action. This resulted in measurable reductions in bacterial burden and mortality [9]. LL-37 binding to the lipid A moiety of LPS blocks CD14-mediated transfer to TLR4, suppressing TNF-alpha and IL-6 release from monocytes in a dose-dependent manner [4][6].
LL-37 and Cancer
The Basics
Preliminary laboratory research suggests LL-37 can selectively kill certain cancer cell lines while sparing normal cells. This selectivity is thought to arise from the same membrane-targeting mechanism that kills bacteria: cancer cells often have a more negatively charged surface than normal cells [5].
However, this area is early-stage and complex. Some studies have shown that LL-37 can promote tumor growth in certain cancer types, making it context-dependent and far from a clear therapeutic prospect [5].
The Science
LL-37 demonstrates selective cytotoxicity against cancer cell lines (ovarian, melanoma, and colon carcinoma) through apoptosis induction and membrane disruption at concentrations of 5-25 mcM [5]. However, context-dependent pro-tumorigenic effects have also been observed: LL-37 can promote cell proliferation, migration, and angiogenesis in breast, lung, and prostate cancer models through EGFR transactivation and IL-8 signaling [5]. The net effect appears to depend on tumor type, local microenvironment, and LL-37 concentration.
Biomarker Evidence Matrix
Category
Immune Function
- Evidence Strength
- 7/10
- Reported Effectiveness
- 6/10
- Summary
- Strong preclinical and mechanistic evidence for broad immune modulation. Clinical data limited to wound healing context. Community reports are positive but nonspecific.
Category
Recovery & Healing
- Evidence Strength
- 8/10
- Reported Effectiveness
- 6/10
- Summary
- Two RCTs demonstrate accelerated wound healing (venous leg ulcers, diabetic foot ulcers). This is LL-37's strongest clinical evidence base. Community reports are positive but confounded by multi-compound stacks.
Category
Skin Health
- Evidence Strength
- 6/10
- Reported Effectiveness
- 5/10
- Summary
- Clinical wound data applies directly to skin. Topical formulation data supports skin applications at 0.05-0.10% concentrations. Role in rosacea/psoriasis pathogenesis creates a nuanced picture.
Category
Gut Health
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Limited preclinical evidence for gut barrier support. Safety concern: LL-37 can disrupt colonic epithelial integrity at higher concentrations. Community reports are mixed.
Category
Inflammation
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- LL-37 has dual pro- and anti-inflammatory activity depending on context and concentration. Community reports are polarized. Not a straightforward anti-inflammatory compound.
Category
Joint Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 3/10
- Summary
- No positive evidence. Community reports include worsened joint inflammation. Literature suggests potential for inflammatory exacerbation in arthritic conditions.
Category
Pain Management
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- Not studied for analgesic effects. Community reports describe dose-dependent pain worsening.
Category
Side Effect Burden
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- Clinical trial data (topical) shows favorable safety comparable to placebo. Systemic/injectable safety is poorly characterized. Community reports highlight dose sensitivity and inflammatory flares.
Category
Digestive Comfort
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- Colonic epithelial disruption concern from literature. Mixed community reports for GI applications.
Category
Focus & Mental Clarity
- Evidence Strength
- 2/10
- Reported Effectiveness
- 4/10
- Summary
- No mechanistic basis for cognitive effects. Single community report of worsened brain fog (confounded case).
Categories not scored (insufficient data): Fat Loss, Muscle Growth, Weight Management, Appetite & Satiety, Food Noise, Energy Levels, Sleep Quality, Memory & Cognition, Mood & Wellbeing, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Physical Performance, Nausea & GI Tolerance, Hair Health, Heart Health, Blood Pressure, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Fluid Retention, Body Image, Bone Health, Longevity & Neuroprotection, Cravings & Impulse Control, Social Connection, Treatment Adherence, Withdrawal Symptoms, Daily Functioning
Benefits & Potential Effects
The Basics
The most established benefit of LL-37 is accelerated wound healing. Clinical trials have shown that applying LL-37 directly to chronic wounds can restart a stalled healing process, particularly in wounds that lack the body's natural LL-37 production [2][3].
For people dealing with recurrent or chronic infections, LL-37's broad-spectrum antimicrobial activity is its primary appeal. It can target bacteria, fungi, and viruses simultaneously, and it works against organisms that have developed resistance to conventional antibiotics. Its biofilm-disrupting ability is particularly relevant for chronic infections where standard antibiotics fail because they cannot penetrate bacterial biofilms [4][8].
Immune modulation is another area of interest. LL-37 coordinates multiple aspects of immune response, from recruiting immune cells to managing inflammation. Some practitioners explore it as an adjunct during or after infections, particularly in the context of mold-related illness or chronic inflammatory conditions.
It is important to note that injectable LL-37 protocols for systemic immune support are entirely practitioner-derived. The clinical trial data supporting LL-37's benefits is exclusively topical. Subcutaneous dosing protocols do not have formal clinical trial backing.
The Science
Wound healing acceleration: Phase II RCT data demonstrates statistically significant improvements in healing rate constants for chronic venous leg ulcers at 0.5 mg/mL topical concentration, with 6-fold improvement versus placebo in predefined responder subgroups [2]. Diabetic foot ulcer RCT data shows enhanced granulation tissue formation at both 0.5 and 1.6 mg/mL concentrations [3]. The mechanism involves EGFR-dependent keratinocyte migration, VEGF-independent angiogenesis, and direct antimicrobial barrier restoration at the wound surface.
Antimicrobial defense: Broad-spectrum bactericidal activity at MICs of 1-50 mcg/mL across gram-positive and gram-negative species, with additional antifungal and antiviral properties [4][6]. Anti-biofilm activity at sub-MIC concentrations enables action against treatment-resistant chronic infections [8]. LPS neutralization prevents endotoxin-mediated inflammatory cascades [4][6][9].
Immunomodulation: FPRL1-mediated chemotaxis recruits neutrophils, monocytes, and T cells [5]. Autophagy induction via the di-leucine motif enhances intracellular pathogen clearance [10]. Modulation of cytokine production shifts the inflammatory milieu in a context-dependent manner [4][5].
The benefits outlined above span multiple body systems, and your experience will be uniquely yours. Rather than guessing which effects are attributable to this compound versus other factors in your life, Doserly helps you log specific outcomes alongside your protocol details, building a clear picture of what's changing and when.
Over weeks and months, this creates something more useful than any anecdotal report: your own evidence-based record of how this compound affects you personally, at your specific dose, within the context of your full health protocol. When it's time to decide whether to continue, adjust, or discontinue, you have real data to inform that conversation with your healthcare provider.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
Side Effects & Safety Considerations
The Basics
LL-37 has a safety profile that depends heavily on the route of administration and the dose.
Topical use appears to be well tolerated. In clinical trials for venous leg ulcers and diabetic foot ulcers, adverse event rates were comparable to placebo [2][3]. Local irritation at the application site is possible but uncommon.
Systemic/injectable use carries a distinctly different risk profile. Because LL-37 is a potent immune activator, injecting it introduces the peptide to tissues and immune cells throughout the body rather than just at a wound surface. Key safety concerns for systemic exposure include:
- Autoimmune activation: LL-37 can form complexes with the body's own DNA and RNA, converting these normally harmless molecules into triggers for autoimmune pathways. This mechanism is directly implicated in the pathogenesis of psoriasis and has been linked to lupus biology [5][7]. People with existing autoimmune conditions face elevated risk.
- Pro-thrombotic effects: LL-37 promotes NET (neutrophil extracellular trap) formation and platelet activation via the GPVI receptor. These pathways are linked to thrombosis and microvascular injury [7].
- Vascular injury signals: LL-37 has been detected within atherosclerotic plaques and can induce smooth muscle cell death and endothelial dysfunction [7].
- Dose-dependent cytotoxicity: At higher concentrations, LL-37 loses its selectivity for microbial membranes and begins damaging host cells. This narrow therapeutic window is a recurring theme in both the literature and community experience [5].
- Inflammatory flares: Community members consistently report that starting at too high a dose triggers significant inflammatory reactions, joint pain, and general malaise. Whether these represent genuine side effects or temporary die-off (Herxheimer) reactions from microbial killing is debated but not established.
Injection-site reactions (redness, itching) are reported occasionally with subcutaneous administration.
The Science
Topical safety profile: Both published RCTs report favorable safety with adverse event rates not statistically different from placebo groups [2][3]. The wound healing trials used concentrations of 0.5-1.6 mg/mL applied twice weekly, establishing these as the clinically validated dose range for topical use.
Systemic risk signals (biological/mechanistic):
LL-37 complexation with self-DNA activates plasmacytoid dendritic cells via TLR9, driving type I interferon production. This pathway is a central mechanism in psoriasis pathogenesis and has been implicated in lupus biology [5][7]. Systemic delivery could amplify IFN-driven inflammation in genetically predisposed individuals.
LL-37 promotes NET formation and enhances NET stability while activating platelets through the GPVI receptor. These pro-thrombotic mechanisms, combined with endothelial dysfunction induction, represent credible cardiovascular risk signals for sustained systemic exposure [7].
Host cell cytotoxicity becomes significant at concentrations above 10-25 mcM. In vitro, LL-37 at these concentrations disrupts colonic epithelial integrity and induces vascular smooth muscle cell death [5][7]. The dose-dependent transition from therapeutic to cytotoxic concentrations underscores the importance of conservative dosing.
Contraindications based on available evidence:
- Active autoimmune conditions (psoriasis, lupus, rheumatoid arthritis)
- Active systemic inflammation
- Known cardiovascular disease or thrombotic history
- Pregnancy and breastfeeding (insufficient data)
- Known hypersensitivity to cathelicidin peptides [7]
Side effect profiles are most useful when you can compare them against your own experience in real time. Doserly lets you log symptoms, severity, and timing alongside your dosing data, creating a side-by-side view of your protocol and your body's response.
This kind of systematic tracking catches things that memory alone misses. A subtle mood shift that began three days after a dose increase. Sleep disruption that correlates with evening administration. These patterns become visible when the data is laid out on a timeline, and they give your healthcare provider actionable information rather than vague concerns. Early detection of emerging side effects means earlier intervention.
Keep side effects, flags, and follow-up notes visible.
Doserly helps you document safety observations, side effects, medication changes, and follow-up questions so important context is not scattered.
Safety log
Flags and notes

Safety notes are not emergency guidance; seek medical help when appropriate.
Dosing Protocols
The Basics
LL-37 dosing varies significantly depending on whether the compound is used topically or by injection, and sources report different ranges for injectable use.
Topical dosing is the best-characterized route. Clinical trials used concentrations of 0.5 mg/mL and 1.6 mg/mL, applied directly to wound surfaces twice weekly during dressing changes for periods of 4 to 13 weeks [2][3]. Cosmeceutical preparations typically use concentrations of 0.05-0.10% (0.5-1.0 mg/mL).
Injectable (subcutaneous) dosing has no formal clinical trial basis. Practitioner-derived protocols generally describe daily subcutaneous injection with gradual titration:
Commonly reported ranges for subcutaneous injection are 50-400 mcg per day, with most sources converging on 100-200 mcg as a typical maintenance range. The community consensus strongly favors starting at the low end (50-100 mcg) and titrating upward slowly, as higher starting doses are consistently associated with worse initial experiences.
Some protocols describe a 5-days-on, 2-days-off schedule rather than continuous daily dosing. Cycle length ranges from 4 to 16 weeks, with 8 to 12 weeks being most commonly cited.
A standard reconstitution approach uses 3.0 mL bacteriostatic water per 5 mg vial, yielding a concentration of approximately 1.67 mg/mL. On a U-100 insulin syringe, 1 unit (0.01 mL) equals approximately 16.7 mcg at this concentration.
The Science
No validated systemic (IV, SC, or oral) dosing regimens exist from controlled human clinical trials. The published efficacy and safety data pertain exclusively to topical administration [2][3][7].
Topical clinical protocols:
- Venous leg ulcers (Phase II/IIb): LL-37 gel/solution at 0.5 or 1.6 mg/mL, twice weekly applications during dressing changes for approximately 13 weeks [2]
- Diabetic foot ulcers (RCT): LL-37 cream at 0.5 mg/mL (and 1.6 mg/mL in some cohorts), twice weekly for 4 weeks [3]
The narrow therapeutic window identified in vitro (efficacy at 1-10 mcM, cytotoxicity above 10-25 mcM) provides a pharmacological basis for the conservative dose titration approach favored in practitioner protocols [5]. Assuming subcutaneous bioavailability of approximately 60-80% and distribution volume of 0.15-0.3 L/kg, a 200 mcg dose in a 70 kg individual would yield estimated peak plasma concentrations well below the cytotoxic threshold, though tissue-level concentrations at the injection site may transiently exceed this range.
The dosing protocols above involve numbers that matter: specific microgram amounts, reconstitution ratios, and timing windows. Getting any of these wrong compounds across every subsequent dose from that vial.
Doserly's dose and reconstitution calculators eliminate the guesswork. Enter your vial size, peptide amount, and target dose, and get the exact bacteriostatic water volume, units per tick mark, and doses per vial. The injection site tracker maps your administration history as a visual heat map across your body, flagging areas that need rest and suggesting rotation patterns. Combined with dose reminders that include compound name, amount, and route, every aspect of your daily protocol is handled with the precision it requires.
Turn symptom and safety notes into a clearer timeline.
Doserly helps you log doses, symptoms, and safety observations side by side so patterns are easier to discuss with a qualified clinician.
Pattern view
Logs and observations

Pattern visibility is informational and should be reviewed with a clinician.
What to Expect
Weeks 1-2: If using topically for wound care, reduced bacterial load and wound preparation are the primary early observations. For subcutaneous use, some users report mild immune activation (slight fatigue, low-grade inflammatory sensation) as the body adjusts. Starting at a low dose (50-100 mcg) helps minimize these initial effects. Herxheimer-type reactions (temporary symptom worsening from microbial die-off) have been reported, particularly in individuals with chronic infections or biofilm-related conditions.
Weeks 2-4: Topical wound applications typically show increased granulation tissue and the beginnings of epithelial migration at this stage [2][3]. For subcutaneous protocols, the initial adjustment period tends to settle, and some users report subtle improvements in infection-related symptoms, wound healing, or general immune resilience. If stacking with Thymosin Alpha-1, synergistic immune effects may become apparent.
Weeks 4-8: Clinical trial data for topical use shows significant wound size reduction and continued healing progression through this timeframe [2][3]. For subcutaneous protocols, most users who will respond report their primary benefits during this window. Dose titration upward typically occurs during this phase if the initial low-dose period was well tolerated.
Weeks 8-12+: Continued progression toward wound closure for topical use. For subcutaneous protocols, this represents the upper range of typical cycle length. Extended courses of 12-16 weeks are described by some practitioners, though evidence for continued benefit beyond 8-12 weeks is anecdotal.
Important note: LL-37 is not a peptide where everyone reports the same experience. Outcomes appear to vary more widely than with compounds like BPC-157 or TB-500, likely due to the dose sensitivity, dual pro/anti-inflammatory properties, and the influence of underlying conditions on how the immune system responds to this peptide.
Interaction Compatibility
Good With (Potential Synergy)
- Thymosin Alpha-1: Frequently stacked for comprehensive immune support. Thymosin Alpha-1 addresses adaptive immune reconstitution while LL-37 provides innate defense. Community reports describe this as a core immune protocol combination.
- BPC-157: Complementary for wound healing applications. BPC-157 promotes angiogenesis and tissue repair through different pathways (VEGF, NO system), potentially enhancing LL-37's direct wound healing effects.
- TB-500: Sometimes included in wound healing stacks alongside BPC-157 for cell migration and tissue remodeling.
- KPV: Anti-inflammatory tripeptide that may help modulate LL-37's pro-inflammatory effects when used together. KPV's NF-kappaB suppression could balance LL-37's immune activation.
- GHK-Cu: Compatible for tissue remodeling and skin repair applications. Different mechanisms (copper delivery vs. antimicrobial defense) complement each other.
- Glutathione: Antioxidant support may help manage the oxidative stress associated with immune activation during LL-37 protocols.
- Vitamin D (3,000-5,000 IU daily): Not a peptide, but mechanistically relevant. Vitamin D directly upregulates endogenous LL-37 production via the CAMP gene promoter [1].
Not Good With (Caution)
- Individuals with active autoimmune conditions: LL-37's TLR9 activation pathway through self-DNA complexes can exacerbate psoriasis, lupus, and potentially other autoimmune conditions [5][7].
- High-dose retinoids or strong AHAs/BHAs (topical): Incompatible with topical LL-37 formulations. May destabilize the peptide or cause excessive irritation.
- Ethanol concentrations above 10%: Compromises peptide stability in topical preparations.
Administration Guide
Materials typically required for subcutaneous administration:
- U-100 insulin syringes (29-31 gauge, 1/2 inch)
- Alcohol swabs (for vial stopper and injection site)
- Sharps disposal container
- LL-37 lyophilized vial (commonly available as 5 mg)
Recommended reconstitution solution: Bacteriostatic water is the standard diluent. The commonly reported reconstitution volume is 3.0 mL per 5 mg vial, yielding approximately 1.67 mg/mL. Some practitioners use sterile 0.9% saline as an alternative. For topical preparations, community sources recommend maintaining pH 5.0-6.5 for stability.
Timing considerations: No specific timing requirements have been established. Most protocols describe administration at any consistent time of day. For subcutaneous injection, site rotation (abdomen, thighs, upper arms) is standard practice, with a minimum distance of 2-3 cm between consecutive sites.
Post-administration monitoring: Monitor for injection site reactions (redness, swelling, itching), which are generally mild and self-limiting. Be alert for signs of systemic immune activation (fatigue, low-grade fever, joint discomfort) particularly during the first 1-2 weeks or after dose increases. If inflammatory symptoms are persistent or escalating rather than transient, consult a healthcare provider.
Supplies & Planning
Vial sizes commonly available: LL-37 is typically sold as 5 mg lyophilized vials.
Syringes: U-100 insulin syringes (29-31 gauge) are standard for subcutaneous administration. For early titration doses of 10 units or fewer (0.10 mL or less), 30-unit or 50-unit insulin syringes provide better precision.
Reconstitution supplies: Bacteriostatic water (10 mL bottles) is the standard diluent. Approximately 3.0 mL is used per vial.
Alcohol swabs: Two per administration session (one for the vial stopper, one for the injection site).
Storage equipment: Refrigerator access for reconstituted vials (2-8°C). Freezer access (-20°C) for long-term lyophilized storage.
For topical preparations: Compatible cream or gel base (such as VersaCream PRO or HelixGel), sterile mixing supplies, pH strips or meter, and opaque airless pump or laminated tube for storage. Specific quantities depend on the concentration and volume prescribed by a healthcare provider. Consult the reconstitution calculator for preparation math.
Storage & Handling
Lyophilized (unreconstituted): Store at -20°C (-4°F) in dry, dark conditions. Stable for approximately 24 months under proper storage conditions.
Reconstituted (injectable): Refrigerate at 2-8°C (35.6-46.4°F), protected from light. Use within 4 weeks. Avoid repeated freeze-thaw cycles. If freezing reconstituted solution, stability is estimated at up to 6 months at -20°C, though this may reduce potency.
Reconstituted (topical preparations): Store at 2-8°C, protected from light. Non-preserved batches should be used within 14 days. Batches prepared in preserved bases may remain stable for 6-8 weeks refrigerated. Discard if discoloration, odor change, or separation occurs.
Handling best practices:
- Allow vials to reach room temperature before opening to reduce condensation uptake
- Avoid vigorous shaking during reconstitution. Gently swirl or roll the vial until dissolved.
- Maintain pH 5.0-6.5 for topical preparations to preserve peptide stability
- Protect from temperatures above 40°C and from strong acids, oxidizers, or metal chelators
Lifestyle Factors
Vitamin D optimization: This is the single most impactful lifestyle factor for LL-37. Vitamin D directly regulates cathelicidin (LL-37) expression through the CAMP gene promoter [1]. Maintaining serum 25-hydroxyvitamin D levels in the 40-60 ng/mL range supports endogenous LL-37 production. Many LL-37 users supplement with 3,000-5,000 IU vitamin D3 daily, ideally paired with vitamin K2.
Protein and micronutrient intake: Adequate protein supports tissue repair and immune cell function. Zinc and vitamin C are particularly relevant for wound healing and immune defense. Zinc is also a cofactor for many antimicrobial peptide-related enzymes.
Wound hygiene (for topical applications): Maintain proper wound care protocols, including regular dressing changes and clean application technique. LL-37's antimicrobial benefits are maximized in a clean wound environment.
Sleep and stress management: Chronic stress and sleep deprivation suppress immune function broadly, which could blunt the benefit of any immune-modulating compound. Prioritizing 7-9 hours of quality sleep and managing cortisol through stress reduction supports the immune environment LL-37 works within.
Avoid immune suppressants when possible: Chronic corticosteroid use or other immunosuppressive agents may counteract LL-37's immune-activating mechanisms. Discuss with a healthcare provider if you are on immunosuppressive therapy.
Regulatory Status & Research Classification
United States (FDA): LL-37 is not FDA-approved for any therapeutic indication. It is classified as a research compound. At least one registered clinical trial (vitamin D supplementation to increase LL-37 in tuberculosis patients) has been listed on ClinicalTrials.gov. Topical LL-37 formulations have undergone Phase II clinical testing for wound healing applications but have not progressed to FDA approval.
Canada (Health Canada): No DIN or NPN assigned. Not approved for therapeutic use.
United Kingdom (MHRA): Not approved. Research use only.
Australia (TGA): Not scheduled or approved for therapeutic use.
European Union (EMA): No marketing authorization. Clinical wound healing trials have been conducted in European centers (notably the Swedish venous leg ulcer study).
WADA Status: LL-37 is classified as a prohibited substance under the World Anti-Doping Agency prohibited list, categorized as an immune-modulating peptide. Athletes subject to WADA testing should not use this compound.
Active clinical research areas: Topical wound healing (chronic ulcers), antimicrobial resistance (novel delivery systems incorporating LL-37), tuberculosis adjunctive therapy (vitamin D-mediated cathelicidin induction), and cancer research (selective cytotoxicity models).
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
Q: Can LL-37 replace antibiotics?
No. For serious bacterial infections, antibiotics remain essential and life-saving. LL-37 is being researched as a potential adjunct, particularly for antibiotic-resistant infections and biofilm-related conditions. It is not a substitute for conventional antimicrobial therapy.
Q: Is LL-37 safe for people with autoimmune conditions?
Based on available evidence, LL-37 poses elevated risk for individuals with autoimmune conditions. The peptide can form complexes with self-DNA that activate autoimmune pathways (TLR9-mediated type I interferon production), a mechanism directly implicated in psoriasis and lupus. Multiple community members and pharmacology-informed commentators advise against LL-37 use in autoimmune contexts. Consultation with a healthcare provider is strongly recommended before considering LL-37 if you have any autoimmune condition.
Q: What dose do most people start with for subcutaneous injection?
Based on available community reports and practitioner protocols, starting doses typically range from 50 to 100 mcg per day, with gradual titration upward by approximately 50 mcg per week as tolerated. Many sources emphasize that starting too high is the most common mistake with LL-37, leading to inflammatory reactions and poor initial experiences. Consult a healthcare professional for guidance on dosing.
Q: Does LL-37 cause inflammation or reduce it?
Both. LL-37 has genuine dual pro- and anti-inflammatory activity that depends on the tissue context, concentration, and the individual's immune status. At appropriate concentrations targeting infections, LL-37 tends to support immune resolution. At higher concentrations or in individuals with autoimmune susceptibility, it can amplify inflammatory pathways. This dual nature is well-documented in the scientific literature and consistently reported in community experience.
Q: How does vitamin D relate to LL-37?
Vitamin D is a direct transcriptional regulator of LL-37 production. When your vitamin D levels are adequate, your body produces more LL-37 naturally. This is one of the most well-characterized mechanisms linking vitamin D status to immune function. Many practitioners recommend optimizing vitamin D levels (targeting 40-60 ng/mL serum 25-hydroxyvitamin D) as a foundational step alongside any LL-37 protocol.
Q: What is the difference between topical and injectable LL-37?
Topical LL-37 delivers the peptide directly to the wound or skin surface, where it acts locally without significant systemic exposure. This route has the strongest clinical evidence (RCTs for wound healing) and the best safety profile. Injectable (subcutaneous) LL-37 delivers the peptide systemically, which expands its potential effects but also introduces the risk of systemic immune activation, autoimmune pathway triggering, and cardiovascular concerns. Injectable protocols are entirely practitioner-derived and lack formal clinical trial backing.
Q: Can I combine LL-37 with other peptides?
LL-37 is commonly stacked with Thymosin Alpha-1 for immune support and with BPC-157 for wound healing. Community reports generally describe these combinations favorably. However, multi-peptide stacking makes it impossible to attribute effects to any single compound. Discuss combinations with a healthcare provider.
Q: What are Herxheimer reactions with LL-37?
Some users report temporary worsening of symptoms when starting LL-37, particularly if they have chronic infections or biofilm-related conditions. This is commonly attributed to die-off reactions as LL-37 disrupts biofilms and kills microorganisms, releasing inflammatory debris. Whether these reactions represent a genuine therapeutic response or a sign of excessive dosing is debated. Starting at a conservative dose and titrating slowly is the most commonly recommended approach.
Sources & References
- Liu PT, Stenger S, Li H, et al. Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science. 2006;311(5768):1770-1773. doi:10.1126/science.1123933 — Establishes the TLR2/1-vitamin D-cathelicidin pathway linking innate immunity to vitamin D status.
- Heilborn JD, Nilsson MF, Kratz G, et al. The cathelicidin anti-microbial peptide LL-37 is involved in re-epithelialization of human skin wounds and is lacking in chronic ulcer epithelium. J Invest Dermatol. 2003;121(4):739-746. doi:10.1046/j.1523-1747.2003.12211.x — Demonstrates LL-37 deficiency in chronic wounds and promotes keratinocyte migration; multicenter RCT data for venous leg ulcers.
- Ramos R, Silva JP, Rodrigues AC, et al. Wound healing activity of the human antimicrobial peptide LL37. Peptides. 2011;32(7):1469-1476. — Supports LL-37's role in wound healing via keratinocyte migration and angiogenesis; RCT data for diabetic foot ulcers published in Arch Dermatol Res.
- Vandamme D, Landuyt B, Luyten W, Schoofs L. A comprehensive summary of LL-37, the factotum human cathelicidin peptide. Cell Immunol. 2012;280(1):22-35. doi:10.1016/j.cellimm.2012.02.006 — Comprehensive review covering antimicrobial spectrum, immunomodulation, and vitamin D regulation.
- Kahlenberg JM, Kaplan MJ. Little peptide, big effects: the role of LL-37 in inflammation and autoimmune disease. J Immunol. 2013;191(10):4895-4901. doi:10.4049/jimmunol.1302005 — Reviews LL-37's dual role in immune defense and autoimmune pathogenesis, including TLR9/self-DNA complexation.
- Neshani A, Zare H, Ghiasi NS, Karimi MA, Hosseini Bafghi M. Decoding LL-37: Structure and antimicrobial mechanisms against microbial threats. 2025. — Updated review of LL-37 structure-function relationships and antimicrobial mechanisms.
- Reference site research summary. LL-37 systemic safety considerations. 2026. — Detailed analysis of systemic risks including IFN-driven autoimmunity, NET-associated thrombosis, and atherosclerotic plaque biology.
- Overhage J, Campisano A, Bains M, et al. Human host defense peptide LL-37 prevents bacterial biofilm formation. Infect Immun. 2008;76(9):4176-4182. doi:10.1128/IAI.00318-08 — Demonstrates LL-37's anti-biofilm activity against P. aeruginosa and other species.
- Hosoda H, Nakamura K, Hu Z, et al. Antimicrobial cathelicidin peptide LL-37 induces NET formation and suppresses the inflammatory response in a mouse septic peritonitis model. Mol Med Rep. 2017;16(4):5618-5626. — Demonstrates LL-37-induced neutrophil microvesicle release and survival improvement in sepsis models.
- Rekha RS, Rao Muvva SS, Wan M, et al. Phenylbutyrate induces LL-37-dependent autophagy and intracellular killing of Mycobacterium tuberculosis in human macrophages. Autophagy. 2015;11(9):1688-1699. — Establishes the di-leucine motif-dependent autophagy induction pathway.
Related Peptide Guides
- Thymosin Alpha-1 — Immune reconstitution peptide, frequently stacked with LL-37
- BPC-157 — Tissue repair peptide, complementary for wound healing
- TB-500 — Cell migration and tissue remodeling, included in wound healing stacks
- KPV — Anti-inflammatory tripeptide, may balance LL-37's pro-inflammatory effects
- GHK-Cu — Copper peptide for tissue remodeling, compatible for skin applications
- Glutathione — Antioxidant support for immune activation protocols
- VIP — Immune tolerance peptide, different mechanism (VPAC1/VPAC2 vs. FPRL1)
- NAD+ — Cellular energy support, sometimes included in immune protocol foundations
- Selank — Anxiolytic/immune peptide, cortisol normalization complement
Need the reconstitution math for LL-37: Complete Research Guide?
Open the calculator with LL-37: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.