Mazdutide: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- IBI362, LY3305677, Mazdutide Injection
Attribute
Administration
- Detail
- Injectable (subcutaneous, once weekly)
Attribute
Research Status
- Detail
- Approved in China (NMPA, June 2025) for chronic weight management and type 2 diabetes; investigational elsewhere; not FDA-approved
Attribute
Typical Dose Range
- Detail
- 2.5-9 mg once weekly with dose escalation
Attribute
Half-Life
- Detail
- Prolonged (engineered for once-weekly dosing)
Attribute
Cycle Length
- Detail
- 12-48 weeks based on clinical trial protocols
Attribute
Storage
- Detail
- Lyophilized: -20°C; Reconstituted: 2-8°C, use within 28 days
Overview / What Is Mazdutide?
The Basics
Mazdutide is a next-generation weight management compound that works by activating two different receptor systems in your body simultaneously. While most of the well-known weight loss medications like semaglutide (Ozempic/Wegovy) target only one receptor, mazdutide targets two: the GLP-1 receptor, which controls appetite and blood sugar, and the glucagon receptor, which tells your body to burn fat and increase energy expenditure.
Think of it like having two separate levers to pull. The first lever (GLP-1) makes you feel full sooner, slows down your digestion, and helps control blood sugar. The second lever (glucagon) tells your liver to start burning stored fat for energy and ramps up your metabolic rate. Pulling both levers at once is the idea behind mazdutide's design, and the clinical data so far suggests this dual approach may offer advantages over pulling just one.
Mazdutide was developed jointly by Eli Lilly and Innovent Biologics, a Chinese pharmaceutical company. It became the world's first approved GLP-1/glucagon dual receptor agonist when China's National Medical Products Administration (NMPA) granted approval in June 2025 for chronic weight management [1]. Phase 3 clinical trials have demonstrated meaningful weight loss, typically ranging from 11-20% of body weight over 48-60 weeks, along with improvements in blood sugar, blood pressure, cholesterol, and liver fat [1][2][3].
The compound is sometimes described as an analogue of oxyntomodulin, a naturally occurring gut hormone that activates both GLP-1 and glucagon receptors. Mazdutide essentially mimics what your body already does after a meal, but with a longer-lasting and more potent effect.
The Science
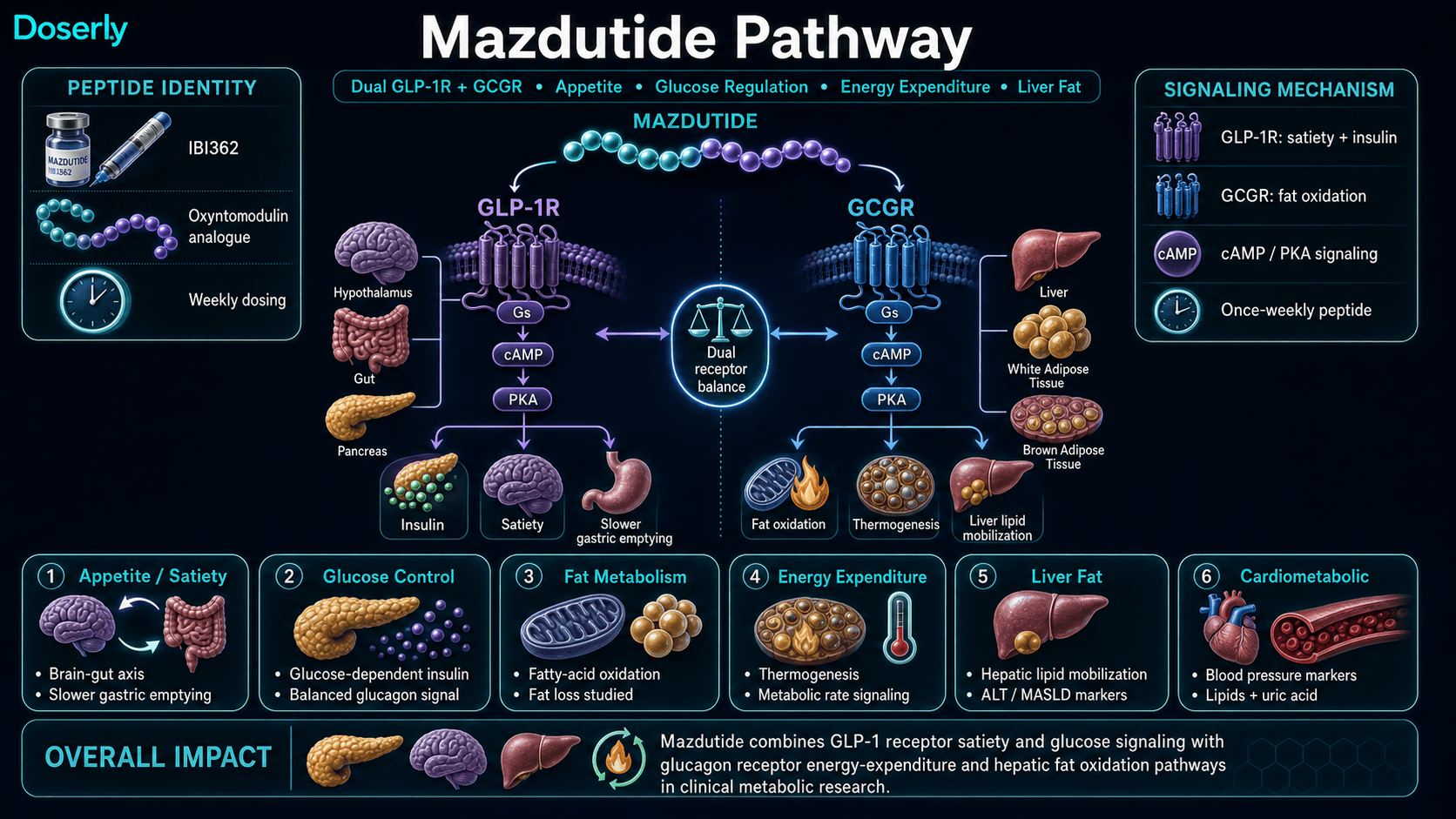
Mazdutide (IBI362/LY3305677) is a synthetic, long-acting unimolecular dual agonist of the glucagon-like peptide-1 receptor (GLP-1R) and the glucagon receptor (GCGR). The compound is engineered as a mammalian oxyntomodulin analogue with structural modifications that extend its circulating half-life to support once-weekly subcutaneous administration [1][4].
The dual receptor engagement produces complementary metabolic effects. GLP-1R activation on pancreatic beta cells enhances glucose-dependent insulin secretion, suppresses inappropriate glucagon release, delays gastric emptying, and activates central satiety pathways in the hypothalamus to reduce appetite and caloric intake [4]. GCGR activation increases hepatic fat oxidation, promotes thermogenesis and energy expenditure, and mobilizes lipids from the liver, addressing metabolic dysfunction-associated steatotic liver disease (MASLD) pathology [1][4].
This dual mechanism distinguishes mazdutide from single-target GLP-1 receptor agonists (semaglutide, liraglutide), GLP-1/GIP dual agonists (tirzepatide), and GLP-1/GIP/glucagon triple agonists (retatrutide). The compound is developed by Innovent Biologics in partnership with Eli Lilly, with advanced clinical development in China and regulatory submissions planned for additional markets [1].
Molecular Identity
Attribute
Common Names
- Detail
- Mazdutide, IBI362, LY3305677
Attribute
Molecular Formula
- Detail
- C207H317N45O65
Attribute
Molecular Weight
- Detail
- ~4,500 g/mol (4.5 kDa)
Attribute
Structural Type
- Detail
- Long-acting dual receptor agonist peptide; oxyntomodulin analogue
Attribute
Classification
- Detail
- Anti-diabetic drug / anti-obesity agent
Mechanism of Action
The Basics
Your body has a built-in system for managing appetite and energy balance. After you eat, your gut releases hormones that tell your brain you're full, signal your pancreas to manage blood sugar, and regulate how fast food moves through your digestive system. Mazdutide amplifies two of these natural signaling pathways.
The first pathway is GLP-1, which is the same system that medications like semaglutide (Ozempic) target. When GLP-1 receptors are activated, you feel full sooner, your stomach empties more slowly, and your blood sugar stays more stable after meals. This is the appetite-suppression side of mazdutide.
The second pathway is glucagon, which is less commonly targeted in weight loss medications. Glucagon tells your liver to burn stored fat for fuel and increases the rate at which your body generates heat (a process called thermogenesis). In other words, it makes your body use more energy even when you're not exercising. This is the "burn more calories" side of mazdutide, and it's what differentiates it from GLP-1-only medications.
By activating both pathways simultaneously, mazdutide aims to reduce how much you eat while also increasing how much energy your body burns. Clinical research has shown that this combination produces greater fat loss relative to lean mass loss compared with GLP-1 agonists alone [1][2].
The Science
Mazdutide activates two class B G-protein coupled receptors (GPCRs) through a single molecular entity:
GLP-1 Receptor (GLP-1R): Binding triggers Gs-protein mediated adenylyl cyclase activation, increasing intracellular cAMP and activating protein kinase A (PKA). Downstream effects include glucose-dependent insulin secretion from pancreatic beta cells, suppression of glucagon secretion from alpha cells, delayed gastric emptying via vagal afferent signaling, and activation of central satiety circuits in the arcuate nucleus and paraventricular nucleus of the hypothalamus [4][5].
Glucagon Receptor (GCGR): Hepatic GCGR activation stimulates glycogenolysis and gluconeogenesis acutely, but the chronic metabolic effects relevant to weight management include increased hepatic fatty acid oxidation via CPT1a upregulation, enhanced energy expenditure through non-shivering thermogenesis, and mobilization of hepatic lipid stores [4][6]. This addresses the limitation of GLP-1 monotherapy, which reduces caloric intake but does not directly increase energy expenditure.
The balanced agonism at both receptors is engineered to maximize metabolic benefit: GLP-1R activation offsets the hyperglycemic potential of GCGR stimulation, while GCGR activation adds a thermogenic component absent from GLP-1-only therapies. Phase 2 data demonstrated preferential fat-mass reduction relative to lean mass [2], and Phase 3 GLORY-2 data showed 71.9% liver fat content reduction by MRI-PDFF at 60 weeks [3].
Pathway Visualization Image
Pharmacokinetics
The Basics
Mazdutide is designed to stay active in your body for about a week after each injection, which is why it only needs to be given once per week. The structural modifications to the peptide slow down how quickly your body breaks it down, maintaining steady levels throughout the week.
After a subcutaneous injection, the compound gradually enters your bloodstream over several hours. It reaches its peak concentration within a day or two and then slowly declines over the rest of the week. By the time your next weekly injection is due, there's still enough active compound in your system to maintain some effect, which is why the therapeutic benefits build up over the first few weeks of treatment.
Because the compound accumulates over multiple weekly doses (reaching what's called "steady state"), the effects generally become more pronounced over the first 4-8 weeks, even at the same dose. This is also why dose escalation protocols start low and gradually increase: giving too much too soon, before your body has adapted to the GLP-1 effects, is what causes the worst nausea and GI symptoms.
The Science
Mazdutide's pharmacokinetic profile is engineered for once-weekly subcutaneous administration through structural modifications that reduce proteolytic degradation and extend circulating half-life. Specific PK parameters (Tmax, Cmax, AUC, absolute bioavailability, clearance, volume of distribution) have not been fully published in publicly available literature as of the current KB sources.
Clinical trial dosing protocols consistently employ once-weekly administration with dose-escalation schedules over 4-8 weeks, indicating the pharmacokinetics support sustained receptor engagement across the dosing interval [1][2][3]. The extended half-life is attributed to structural features analogous to other long-acting incretin analogues (albumin binding, acylation, or PEG conjugation), though the specific pharmacokinetic engineering details of mazdutide have not been disclosed in the available sources.
Metabolism occurs primarily through proteolytic degradation with renal clearance. Steady-state concentrations are expected within 4-5 weeks of weekly dosing based on general long-acting peptide pharmacokinetics.
Research & Clinical Evidence
The Basics
Mazdutide has a stronger clinical evidence base than most compounds covered in peptide guides. It has been studied in multiple Phase 2 and Phase 3 clinical trials enrolling thousands of participants, primarily in China. In 2025, it became the first GLP-1/glucagon dual agonist to receive regulatory approval anywhere in the world.
The weight loss results have been substantial. In the Phase 3 GLORY-1 trial, participants with obesity lost an average of 11-14% of their body weight over 48 weeks [1]. In the larger GLORY-2 trial studying a higher 9 mg dose, the average weight loss reached 18.55% at 60 weeks, with 44% of participants losing 20% or more of their body weight [3]. Among participants without diabetes, the mean reduction was even higher at 20.08% [3].
Beyond weight loss, clinical trials have shown improvements in blood sugar control (HbA1c reduction of approximately 1.5-1.7%), blood pressure, cholesterol, liver fat content, and uric acid levels [1][2][5]. The liver fat data is particularly noteworthy: in a subset of GLORY-2 participants, liver fat content measured by MRI dropped by 71.9% [3].
A head-to-head Phase 3 trial (DREAMS-3) compared mazdutide directly against semaglutide in patients with type 2 diabetes and obesity. Mazdutide demonstrated superiority in achieving combined glycemic and weight loss targets: 48% of mazdutide patients achieved both HbA1c below 7% and at least 10% weight loss, compared to 21.6% for semaglutide [7].
The Science
Phase 1b dose-ranging (Ji et al., 2022): A randomized, placebo-controlled trial evaluated mazdutide 9 mg and 10 mg in Chinese adults with overweight/obesity. Results established safety and preliminary efficacy at higher doses, informing Phase 3 dose selection [4].
Phase 2 obesity trial (Ji et al., 2023): A 24-week randomized controlled trial in Chinese adults with overweight/obesity demonstrated dose-dependent weight loss of 6.7-11.3% at 3-6 mg weekly. The 6 mg arm produced the most pronounced effects, with over 51% of participants achieving 10% or greater weight loss. Improvements were observed in blood pressure, lipids, HbA1c, ALT, uric acid, and preferential fat-mass versus lean-mass reduction [2].
Phase 2 T2D trial (Zhang et al., 2024): A 20-week randomized, double-blind, placebo-controlled trial in Chinese patients with type 2 diabetes showed meaningful HbA1c reductions of approximately 1.7% alongside approximately 7% body weight loss [5].
Phase 3 GLORY-1 (Ji et al., 2025): Once-weekly mazdutide in Chinese adults with obesity or overweight. 48-week results demonstrated 11-14% mean body weight reduction with 4-6 mg maintenance dosing [1].
Phase 3 GLORY-2 (Innovent, 2025): Evaluated mazdutide 9 mg in 462 Chinese adults with obesity (BMI 30 or greater) over 60 weeks. Mean weight reduction of 18.55% versus 3.02% for placebo. 44.0% of participants achieved 20% or greater weight loss. Among non-diabetic participants, mean reduction was 20.08%. Liver fat content reduction of 71.9% by MRI-PDFF. No new safety signals; GI adverse events were mostly mild to moderate and transient [3].
Phase 3 DREAMS-3 (2025): Head-to-head comparison against semaglutide in 349 Chinese adults with early-stage T2D and obesity. Mazdutide achieved superior combined glycemic and weight loss endpoints: HbA1c reduction of approximately 2% (vs. ~1.5% for semaglutide) and weight reduction of 10.29% (vs. 6.00% for semaglutide). Primary endpoint (composite HbA1c <7% + 10% or greater weight loss) met by 48.0% vs. 21.6% (p < 0.001) [7].
Systematic review and meta-analysis: A comprehensive review across diabetic and non-diabetic populations confirmed consistent weight loss efficacy (6-14% over 24-48 weeks, higher with 9 mg dosing) with a tolerability profile consistent with the GLP-1 class [8].
Biomarker Evidence Matrix
Category
Fat Loss
- Evidence Strength
- 9/10
- Reported Effectiveness
- 7/10
- Summary
- Multiple Phase 2/3 RCTs demonstrate 6-20% body weight loss with preferential fat mass reduction. Community reports confirm meaningful fat loss, often in stacking contexts.
Category
Weight Management
- Evidence Strength
- 9/10
- Reported Effectiveness
- 7/10
- Summary
- Phase 3 GLORY trials show 11-20% weight reduction over 48-60 weeks. Community reports align with clinical data.
Category
Appetite & Satiety
- Evidence Strength
- 8/10
- Reported Effectiveness
- 6/10
- Summary
- GLP-1R mechanism well-established for appetite suppression. Community reports are positive but note mazdutide may be less suppressive than tirzepatide at comparable doses.
Category
Food Noise
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- GLP-1 mechanism supports food noise reduction, but no mazdutide-specific studies or substantial community reports. Extrapolated from GLP-1 class evidence.
Category
Energy Levels
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Glucagon component theoretically supports energy via thermogenesis. Limited direct evidence; one community report of improved energy vs. semaglutide.
Category
Nausea & GI Tolerance
- Evidence Strength
- 8/10
- Reported Effectiveness
- 4/10
- Summary
- Well-documented in all clinical trials. GI effects (nausea, diarrhea, vomiting) are the most common adverse events, mostly mild-moderate and transient. Community reports are mixed.
Category
Digestive Comfort
- Evidence Strength
- 6/10
- Reported Effectiveness
- 4/10
- Summary
- Delayed gastric emptying documented. Some users report digestive discomfort during titration.
Category
Heart Health
- Evidence Strength
- 7/10
- Reported Effectiveness
- 5/10
- Summary
- BP and lipid improvements demonstrated in trials. No long-term cardiovascular outcomes data (unlike semaglutide's SELECT trial).
Category
Blood Pressure
- Evidence Strength
- 7/10
- Reported Effectiveness
- 6/10
- Summary
- Clinical trials show BP improvements. One community report confirms significant BP reduction.
Category
Heart Rate & Palpitations
- Evidence Strength
- 6/10
- Reported Effectiveness
- 4/10
- Summary
- Documented HR increase of 5-9 bpm in trials. Sinus tachycardia reported as mild and transient.
Category
Joint Health
- Evidence Strength
- 3/10
- Reported Effectiveness
- 7/10
- Summary
- No direct pharmacological evidence for joint effects. One community report of dramatic improvement, likely secondary to weight loss.
Category
Inflammation
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- ALT/liver enzyme improvements suggest anti-inflammatory effect. Two community reports of perceived reduced inflammation.
Category
Side Effect Burden
- Evidence Strength
- 8/10
- Reported Effectiveness
- 5/10
- Summary
- Well-characterized in Phase 2/3 trials. GI effects predominate; 2.9% discontinuation rate in GLORY-2.
Category
Treatment Adherence
- Evidence Strength
- 7/10
- Reported Effectiveness
- 6/10
- Summary
- Once-weekly dosing supports adherence. Low discontinuation rates in clinical trials.
Category
Gut Health
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Liver fat reduction documented; direct gut effects not specifically studied.
Categories scored: 15
Categories with community data: 16
Categories not scored (insufficient data): Muscle Growth, Sleep Quality, Focus & Mental Clarity, Memory & Cognition, Mood & Wellbeing, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Pain Management, Recovery & Healing, Physical Performance, Skin Health, Hair Health, Hormonal Symptoms, Temperature Regulation, Fluid Retention, Body Image, Immune Function, Bone Health, Longevity & Neuroprotection, Cravings & Impulse Control, Social Connection, Daily Functioning, Withdrawal Symptoms
Benefits & Potential Effects
The Basics
The primary benefit of mazdutide, based on clinical trial data, is substantial weight loss. Most participants in the larger trials lost between 11-20% of their body weight, which for someone weighing 220 pounds would mean losing roughly 24-44 pounds. What makes this particularly meaningful is that the weight loss appears to come predominantly from fat rather than muscle, which is a significant concern with many weight loss approaches.
Beyond the scale, mazdutide has shown improvements across a range of metabolic markers. Blood sugar levels improve, blood pressure comes down, cholesterol profiles shift in a healthier direction, and liver fat decreases substantially. For people dealing with metabolic syndrome or early type 2 diabetes alongside obesity, this breadth of metabolic improvement is notable.
The glucagon receptor component also adds something that pure GLP-1 medications do not: an increase in energy expenditure. Rather than only reducing how much you eat, mazdutide also increases how much energy your body burns. Some community members have reported feeling more energetic on mazdutide compared to semaglutide, though individual experiences vary widely.
Inflammation reduction is an emerging benefit that several users have highlighted. While the research has not specifically studied mazdutide's anti-inflammatory effects, users have reported that reduced inflammation was among the most valued outcomes of their treatment.
The Science
Evidence-based potential effects supported by Phase 2 and Phase 3 clinical trial data include:
Body weight reduction: Dose-dependent weight loss of 6-20% across 24-60 week trials. GLORY-2 demonstrated 18.55% mean reduction at 60 weeks with 9 mg dosing, with 44% of participants achieving 20% or greater reduction [3]. GLORY-1 showed 11-14% at 48 weeks with 4-6 mg [1].
Glycemic control: HbA1c reduction of 1.5-2.0% across diabetic populations. DREAMS-3 demonstrated superiority over semaglutide for combined glycemic and weight endpoints [7].
Body composition: Preferential fat-mass reduction relative to lean mass in Phase 2 data, distinguishing mazdutide from approaches that produce proportionally higher lean mass loss [2].
Hepatic fat reduction: MRI-PDFF measured liver fat content reduction of 71.9% at 60 weeks in GLORY-2 subset analysis [3]. This is clinically significant for MASLD/MASH populations.
Cardiometabolic parameters: Improvements in blood pressure, triglycerides, LDL cholesterol, uric acid, and ALT documented across trials [1][2].
Energy expenditure: GCGR activation drives increased thermogenesis and fatty acid oxidation, contributing to energy expenditure above baseline. This mechanism is absent from pure GLP-1 agonists and represents a theoretical advantage for fat loss maintenance [4][6].
Reading about potential benefits is the starting point. Knowing whether you're actually experiencing them is where real value begins. Doserly lets you track the specific health markers that matter for your protocol, from body composition and energy levels to sleep quality, mood, and recovery time, building a personal dataset that goes beyond subjective impressions.
The app's proactive monitoring doesn't wait for you to notice a problem. It surfaces patterns in your logged data that might suggest suboptimal timing, flags potential interactions with other items in your health stack, and helps you identify which benefits are tracking with what the research suggests and which aren't materializing. Think of it as a second set of eyes on your protocol, always watching the trends.
Keep sensitive protocol records in a purpose-built app.
Doserly is designed for private health tracking with structured records, offline-ready workflows, and exportable history when you need it.
Privacy
Health records
Privacy controls help you manage records; keep clinical records where required.
Side Effects & Safety Considerations
The Basics
The side effect profile of mazdutide is consistent with what you would expect from any GLP-1-based medication. The most common issues are gastrointestinal: nausea, diarrhea, and vomiting. These are most pronounced during the dose-escalation phase (the first few weeks when your dose is being gradually increased) and tend to diminish as your body adjusts.
The good news is that these GI effects are generally described as mild to moderate. In the GLORY-2 trial, only 2.9% of participants discontinued treatment due to adverse events [3]. The gradual dose-escalation approach is specifically designed to minimize these effects, which is why protocols start at a lower dose and increase slowly.
A few safety considerations deserve special attention. First, heart rate may increase modestly (about 5-9 beats per minute on average). Clinical trials documented occasional sinus tachycardia, but these episodes were generally mild and transient [5]. Second, lipase levels may increase in some individuals. While no investigator-suspected pancreatitis was reported in the Phase 2 obesity trial, this requires monitoring given the class-level concern with GLP-1 medications [5]. Third, anti-drug antibodies developed in 23-33% of trial participants, though these did not appear to affect the medication's performance [5].
Liver enzyme elevations have been a topic of discussion in the community. While mazdutide generally reduces ALT levels (a positive sign for liver health), the rapid fat loss it produces can cause temporary enzyme elevations as fat is mobilized from the liver. This is a well-recognized phenomenon with rapid weight loss of any type, not specific to mazdutide, but it underscores the importance of regular blood work monitoring.
The Science
Gastrointestinal effects: The predominant adverse event class across all trials. Phase 2 data reported diarrhea, nausea, vomiting, and decreased appetite as the most frequent treatment-emergent adverse events, with higher incidence at higher doses and during escalation periods [2][4][5]. GLORY-2 confirmed this pattern, with the majority of GI events classified as mild-to-moderate and transient [3].
Cardiovascular: Mean heart rate increases of 5-9 bpm documented. ECG events including sinus tachycardia reported as generally mild and transient [5]. Long-term cardiovascular outcomes data (comparable to the semaglutide SELECT trial) are not yet available.
Pancreatic enzymes: Occasional lipase elevations observed without clinical sequelae. No investigator-suspected pancreatitis in the 24-week Phase 2 obesity trial. Class-level vigilance for pancreatitis remains prudent for all GLP-1-based therapies [5].
Immunogenicity: Anti-drug antibody formation in 23-33% of participants across trials, without apparent impact on efficacy or safety [5].
Hepatobiliary: GLP-1-class warnings for gallbladder disease apply. Clinical monitoring recommended. ALT reductions observed on average, suggesting net hepatoprotective effect, but individual transient elevations may occur during rapid hepatic fat mobilization [5].
Hypoglycemia: Asymptomatic hypoglycemia uncommon without concurrent use of insulin or secretagogues [5].
The side effects and contraindications above give you a map of what to watch for. Doserly turns that map into a daily practice. Log the specific biomarkers and symptoms associated with this compound's known risk profile, and the app builds a timeline of how your body is responding across your cycle.
Trending in the wrong direction on a key marker? Noticing a pattern that started two weeks into your protocol? Doserly connects the dots between your protocol timeline and your logged data, making it easier to spot emerging issues early and have informed, data-backed conversations with your healthcare provider about what's working and what needs attention.
Keep side effects, flags, and follow-up notes visible.
Doserly helps you document safety observations, side effects, medication changes, and follow-up questions so important context is not scattered.
Safety log
Flags and notes

Safety notes are not emergency guidance; seek medical help when appropriate.
Dosing Protocols
The Basics
Mazdutide is administered as a once-weekly subcutaneous injection. The key principle across all dosing approaches is gradual escalation: starting at a lower dose and increasing over several weeks. This allows your body to adapt to the GLP-1 effects and significantly reduces the nausea and GI discomfort that would occur if you started at a full dose.
Sources report several dosing approaches. The most commonly cited clinical trial protocol starts at 2.5 mg weekly for the first 4 weeks, then increases to 5 mg weekly from week 5 onward. For the higher-dose regimen studied in GLORY-2, patients escalated to 9 mg.
Community and clinical sources generally agree on the range of 2.5-6 mg per week as the standard therapeutic window, with some Phase 1b research exploring doses up to 9-10 mg. The conservative approach starts lower (0.5-1.5 mg) and increases more slowly, which may be appropriate for individuals new to GLP-1 medications or those sensitive to GI effects. The standard approach mirrors clinical trial protocols. Doses above 6 mg carry a higher risk of gastrointestinal side effects and should only be considered under close medical supervision.
Maintenance dosing is an important consideration for longer-term use. Some practitioners recommend identifying the lowest effective dose, one at which weight is stable and appetite is managed without excessive suppression. This requires careful attention to nutritional adequacy, as doses that suppress appetite too aggressively can lead to insufficient caloric intake.
The Science
Clinical trial dosing protocols have employed the following escalation schemes:
Phase 2 obesity trial [2]:
- 3 mg arm: 1.5 mg weeks 1-4, then 3 mg weeks 5-24
- 4.5 mg arm: 1.5 mg weeks 1-4, 3 mg weeks 5-8, 4.5 mg weeks 9-24
- 6 mg arm: 2 mg weeks 1-4, 4 mg weeks 5-8, 6 mg weeks 9-24
Phase 3 GLORY-2 [3]:
- Escalation to 9 mg (specific titration schedule from the 60-week protocol)
Phase 1b dose-ranging [4]:
- 9 mg and 10 mg doses explored for safety and preliminary efficacy
All protocols specify once-weekly subcutaneous administration. Dose escalation intervals of 4 weeks per step are consistently employed across trials, with the rationale of minimizing GI adverse events through gradual receptor desensitization. Higher doses (above 6 mg) demonstrated greater efficacy but also higher GI adverse event incidence [4][5].
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders

Reminder tracking supports consistency; it does not select a protocol for you.
What to Expect
Most clinical trial protocols for mazdutide span 24-60 weeks. Based on the available data and community reports, here is what the trajectory generally looks like:
Weeks 1-4 (Low-dose introduction): The initial dose-escalation period. Appetite suppression may begin within the first week for some individuals, though others notice minimal change at the starting dose. GI effects (nausea, decreased appetite) are most likely to appear during this phase and the first dose increase. Most people tolerate this phase well. Weight loss during this period is typically modest, often 1-3% of body weight, with some of this reflecting water weight changes.
Weeks 5-8 (Dose escalation continues): As the dose increases, appetite suppression typically becomes more pronounced. Most users report a clear shift in their relationship with food during this window. GI effects from the dose increase usually resolve within 1-2 weeks. Weight loss accelerates, with clinical trial data showing steady progress from this point forward.
Weeks 9-16 (Maintenance dose reached): By this point, most protocols have reached their target maintenance dose. The GI adaptation is largely complete. Weight loss continues at a steady rate. Metabolic improvements (blood sugar, blood pressure, cholesterol) become measurable in blood work. Users commonly report feeling adapted to the medication with a new baseline for appetite and energy.
Weeks 17-48+ (Sustained phase): In the GLORY trials, weight loss continued without plateauing through 48-60 weeks [1][3]. The GLORY-2 data specifically noted "continuous weight loss, with no plateau observed in Week 60" [3]. Metabolic improvements continue to accumulate. Liver fat reduction reaches its most pronounced levels during this extended phase.
After stopping: Limited data exists on post-cessation outcomes for mazdutide specifically. Based on the GLP-1 class as a whole, some weight regain is expected after discontinuation. Community discussion about maintenance dosing suggests identifying the lowest effective dose for long-term use may help mitigate this.
Interaction Compatibility
Good With (Potentially Synergistic)
- Tirzepatide: Multiple community members report stacking mazdutide with tirzepatide. The rationale is covering all three incretin receptor types: GLP-1 (both), GIP (tirzepatide), and glucagon (mazdutide). One user reported 20% body weight loss over 6 months with this combination. Note: this is community-reported stacking, not clinically studied.
- NAD+: Based on the general principle that compounds creating caloric deficits increase NAD+ demand for beta-oxidation. No mazdutide-specific stacking data.
- MOTS-C: Metabolic support peptide that may complement GLP-1 agents. No mazdutide-specific interaction data.
- Tesamorelin: For lean mass preservation during rapid weight loss. Theoretical synergy, not studied with mazdutide.
- Metformin: Commonly used alongside GLP-1 agents in type 2 diabetes management. Clinical trials permitted concurrent metformin use.
Not Good With (Use Caution)
- Other GLP-1 agonists (Semaglutide, Retatrutide): Doubling GLP-1 receptor stimulation increases GI side effect risk without proportional benefit. Community reports of switching between these compounds rather than stacking.
- Insulin/secretagogues: Increased hypoglycemia risk when combined with insulin or insulin-secreting medications. Dose adjustments required under medical supervision.
- Survodutide: Same dual GLP-1/glucagon mechanism. No rationale for combining two compounds with identical receptor targets.
- Compounds affecting gastric motility: Mazdutide already slows gastric emptying. Additional agents with the same effect could compound GI distress.
Administration Guide
Mazdutide is administered via subcutaneous injection once per week. The following practical information applies to the typical research-grade peptide format.
Materials typically required:
- Mazdutide lyophilized vial (available in 5 mg and 10 mg sizes)
- Bacteriostatic water for reconstitution
- Insulin syringes (U-100, 1 mL or 3 mL capacity)
- Alcohol swabs
- Sharps container for disposal
Reconstitution: Standard reconstitution uses 3.0 mL of bacteriostatic water per 5 mg vial (yielding approximately 1.67 mg/mL) or 3.0 mL per 10 mg vial (yielding approximately 3.33 mg/mL). These concentrations provide practical unit measurements on standard U-100 insulin syringes.
Timing considerations: Clinical trials specify administration on the same day each week. There are no specific fasting requirements documented for mazdutide. Rotating injection sites (abdomen, thighs, upper arms) is standard practice for subcutaneous peptide administration.
Post-administration monitoring: Watch for injection site reactions (redness, swelling, mild discomfort) which are common but typically mild. GI effects (nausea, decreased appetite) are most likely in the hours and days following injection, especially during dose-escalation phases. Heart rate monitoring is recommended given the documented 5-9 bpm increase.
Supplies & Planning
Vial sizes: Mazdutide is commonly available in 5 mg and 10 mg lyophilized vial formats in the research peptide market.
Syringes: U-100 insulin syringes. For standard reconstitution concentrations, 1 mL syringes provide adequate volume for most doses. At higher doses (above 5 mg), 3 mL syringes or split-dose injections across two sites may be needed.
Reconstitution solution: Bacteriostatic water is the standard reconstitution solution. Typical volumes are 3.0 mL per vial.
Storage containers: Reconstituted vials should be stored upright in a refrigerator. Consider a dedicated storage container or designated shelf space.
Additional supplies: Alcohol swabs (2 per injection session: one for vial stopper, one for injection site), sharps disposal container, and vial labels with reconstitution date.
Specific quantities of vials, syringes, and supplies depend on the dose, cycle length, and reconstitution approach chosen in consultation with a healthcare provider. Use Doserly's reconstitution calculator for precise preparation math.
Storage & Handling
Lyophilized (powder) form:
- Store at -20°C (-4°F) or below for long-term stability
- Protect from moisture and light
- Dry, dark conditions preferred
Reconstituted (liquid) form:
- Refrigerate at 2-8°C (35.6-46.4°F) immediately after reconstitution
- Use bacteriostatic water for multi-dose stability
- Discard after 28 days or if cloudiness, particulates, or discoloration appear
- Do not freeze reconstituted solution; freeze-thaw cycles can denature the peptide
General handling:
- Label reconstituted vials with date and concentration
- Allow reconstituted vials to reach room temperature briefly before withdrawing a dose (reduces viscosity)
- Use aseptic technique when accessing multi-dose vials
- Never share vials or syringes between individuals
Lifestyle Factors
Weight management compounds work best when complemented by lifestyle practices that support their mechanisms. For mazdutide specifically, several factors can meaningfully influence outcomes:
Nutrition: Maintaining adequate protein intake is critical during rapid weight loss to preserve lean mass. Sources generally recommend a balanced, nutrient-dense diet with sufficient protein, particularly given that mazdutide can significantly reduce appetite and overall caloric intake. If appetite suppression makes it difficult to consume adequate calories, this is a signal to discuss dosing with a healthcare provider. The maintenance protocol discussion in community sources emphasizes that adequate caloric intake according to biometrics must be attainable.
Exercise: Combining resistance training with aerobic exercise supports the preferential fat loss that mazdutide appears to promote. Resistance training specifically helps preserve lean mass during caloric deficit, which is a key concern during rapid weight loss with any GLP-1 agent.
Hydration and electrolytes: GI effects (diarrhea, nausea) during dose escalation can deplete fluids and electrolytes. Monitoring hydration and electrolyte intake is recommended, especially during the first weeks of a new dose level.
Sleep: Consistent sleep of 7-9 hours nightly supports metabolic health, hormonal balance, and adherence to any protocol. Disrupted sleep can increase appetite hormones and undermine the benefits of the medication.
Monitoring: Regular blood work is strongly recommended, including metabolic panels (glucose, HbA1c, lipids), liver enzymes (ALT, AST), pancreatic enzymes (lipase, amylase if symptoms arise), and cardiovascular markers (heart rate, blood pressure). Community protocols suggest monitoring anthropometrics (body weight, BMI, waist circumference), vitals, glycemia, lipids, and pancreato-biliary markers.
Regulatory Status & Research Classification
China (NMPA): Approved. Mazdutide received NMPA approval in June 2025 for two indications: (1) chronic weight management as an adjunct to reduced-calorie diet and increased physical activity in adults with BMI 28 or greater (obesity) or BMI 24 or greater with at least one weight-related comorbidity; (2) glycemic control in adults with type 2 diabetes. China is currently the only country where mazdutide is approved for clinical use [1][3].
United States (FDA): Not approved. Mazdutide remains an investigational compound in the US. Clinical development outside China is ongoing but regulatory filings have not been publicly announced for the US market as of March 2026.
European Union (EMA): Not approved. No marketing authorization application has been publicly disclosed.
Other jurisdictions: No approvals have been announced outside China. Innovent Biologics has indicated plans for global regulatory submissions, but timelines have not been specified.
WADA status: Not listed on the World Anti-Doping Agency's prohibited list as a specific named substance, though GLP-1 receptor agonists are not among the prohibited substance classes. Athletes should verify current WADA status independently.
Active clinical trials: Multiple Phase 3 trials are ongoing or completed in China, including GLORY-1, GLORY-2, DREAMS-1, DREAMS-2, DREAMS-3, and MASLD/MASH programs [1][3][7]. ClinicalTrials.gov identifiers include NCT06184568 (DREAMS-3).
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is mazdutide and how is it different from semaglutide or tirzepatide?
Mazdutide is a dual GLP-1/glucagon receptor agonist. Semaglutide (Ozempic/Wegovy) targets only the GLP-1 receptor. Tirzepatide (Mounjaro/Zepbound) targets GLP-1 and GIP receptors. Mazdutide's unique feature is glucagon receptor activation, which increases energy expenditure and promotes liver fat burning, rather than the GIP receptor activation that tirzepatide uses. In the DREAMS-3 head-to-head trial, mazdutide demonstrated superior combined glycemic and weight loss outcomes compared to semaglutide [7].
How much weight loss can be expected with mazdutide?
Based on clinical trial data, commonly reported ranges are 6-20% of body weight over 24-60 weeks, depending on the dose and duration. The Phase 3 GLORY-2 trial reported an average of 18.55% at 60 weeks with the 9 mg dose [3]. Individual results vary significantly based on starting weight, dose, diet, exercise, and biological factors. Consult a healthcare professional for personalized guidance.
Is mazdutide FDA-approved?
As of March 2026, mazdutide is not FDA-approved. It was approved in China (NMPA) in June 2025. It remains investigational in the United States, European Union, and most other countries.
What are the main side effects?
Gastrointestinal effects are the most common: nausea, diarrhea, vomiting, and decreased appetite. These are typically mild-to-moderate and most pronounced during dose escalation. A modest heart rate increase (5-9 bpm average) has been documented. Anti-drug antibodies develop in 23-33% of users but do not appear to affect efficacy. Consult a healthcare professional about monitoring recommendations [5].
How does mazdutide compare to retatrutide?
Retatrutide is a triple agonist targeting GLP-1, GIP, and glucagon receptors. Mazdutide is a dual agonist targeting GLP-1 and glucagon. Retatrutide has shown higher average weight loss in trials (up to 24% at 48 weeks). However, no direct head-to-head trial between mazdutide and retatrutide has been published. Some community members have reported that mazdutide provides better appetite suppression than retatrutide for certain individuals, though others have reported the opposite. Retatrutide remains investigational worldwide, while mazdutide is approved in China.
Can mazdutide be stacked with other peptides?
Community members report stacking mazdutide with tirzepatide, though this has not been studied in clinical trials. Stacking with other GLP-1 agonists (semaglutide, retatrutide) is generally not recommended due to overlapping mechanisms and increased side effect risk. Any combination protocol should be discussed with a qualified healthcare provider.
How should mazdutide be stored?
Lyophilized (powder): store at -20°C. Reconstituted: refrigerate at 2-8°C and use within 28 days. Do not freeze reconstituted solution. Protect from light.
Sources & References
[1] Ji L, Jiang H, Bi Y, et al. "Once-Weekly Mazdutide in Chinese Adults with Obesity or Overweight." GLORY-1 Phase 3 trial results. New England Journal of Medicine. (2025).
[2] Ji L, Jiang H, Cheng Z, et al. "A phase 2 randomised controlled trial of mazdutide in Chinese overweight adults or adults with obesity." Nature Communications. (2023).
[3] Innovent Biologics. "Mazdutide 9 mg achieves up to 20.1% weight loss as GLORY-2 Study meets primary and all key secondary endpoints." Press release and Phase 3 GLORY-2 trial results. (November 2025).
[4] Ji L, Gao L, Jiang H, et al. "Safety and efficacy of a GLP-1 and glucagon receptor dual agonist mazdutide (IBI362) 9 mg and 10 mg in Chinese adults with overweight or obesity: A randomised, placebo-controlled, multiple-ascending-dose phase 1b trial." EClinicalMedicine. (2022). PubMed.
[5] Zhang B, Cheng Z, Chen J, et al. "Efficacy and Safety of Mazdutide in Chinese Patients With Type 2 Diabetes: A Randomized, Double-Blind, Placebo-Controlled Phase 2 Trial." Diabetes Care. (2024). PubMed.
[6] International Journal of Obesity (Nature). "Pipeline for future obesity medications (including mazdutide dual agonist mechanism)." Review article.
[7] ClinicalTrials.gov identifier: NCT06184568. "A study comparing IBI362 vs semaglutide in Chinese adults with early type 2 diabetes and obesity" (DREAMS-3 Phase 3 trial). Innovent Biologics press release (October 2025); PatientCareOnline coverage.
[8] Frontiers in Endocrinology. "Systematic review and meta-analysis: Efficacy and safety of mazdutide on weight loss (diabetic and non-diabetic patients)."
[9] Shirley M. "Mazdutide: First Approval." Drugs. (2025).
Related Peptide Guides
- Semaglutide - GLP-1 receptor agonist; the most prescribed and studied incretin therapy
- Tirzepatide - Dual GLP-1/GIP receptor agonist; commonly stacked with mazdutide in community protocols
- Retatrutide - Triple GLP-1/GIP/glucagon agonist; the closest mechanistic relative with all three receptor targets
- Survodutide - Dual GLP-1/glucagon agonist; same receptor targets as mazdutide but different molecular structure and receptor affinity ratios
- Cagrilintide - Amylin analogue used in combination approaches with GLP-1 agents
- Orforglipron - Non-peptide oral GLP-1 agonist; next-generation oral approach
- NAD+ - Metabolic support compound; theoretically relevant for supporting beta-oxidation during caloric deficit
- MOTS-C - Mitochondrial-derived metabolic peptide; potential complementary compound
- Tesamorelin - GH secretagogue used for lean mass preservation during weight loss
- AOD-9604 - Fat loss peptide; different mechanism (GH fragment)
Need the reconstitution math for Mazdutide: Complete Research Guide?
Open the calculator with Mazdutide: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.