Survodutide: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- BI 456906, BI-456906
Attribute
Administration
- Detail
- Subcutaneous injection, once weekly
Attribute
Research Status
- Detail
- Investigational. Phase 3 clinical trials ongoing. FDA Fast Track (May 2021), FDA Breakthrough Therapy designation for non-cirrhotic MASH with F2-F3 fibrosis (Oct 2024), EMA PRIME (Nov 2023). Not approved for any indication.
Attribute
Typical Dose Range
- Detail
- 0.6 to 6.0 mg once weekly (Phase 2 trial doses); gradual titration over 10-20 weeks to target maintenance dose
Attribute
Half-Life
- Detail
- Approximately 10-14 days (fatty acid modification enables albumin binding for extended duration)
Attribute
Cycle Length
- Detail
- 12-16 weeks minimum in research protocols; Phase 3 trials extend to 48-76 weeks
Attribute
Storage
- Detail
- Lyophilized: store at -20C or below, protected from light and moisture. Reconstituted: refrigerate at 2-8C, protected from light, avoid repeated freeze-thaw cycles
Overview / What Is Survodutide?
The Basics
Survodutide is an investigational peptide designed to tackle obesity, type 2 diabetes, and fatty liver disease by activating two key metabolic receptors at the same time. It belongs to the emerging class of multi-receptor agonists that build on the success of GLP-1 drugs like semaglutide (Ozempic/Wegovy) by adding a second mechanism of action.
The first mechanism is GLP-1 receptor activation, which reduces appetite, slows stomach emptying, and improves blood sugar control. If you are familiar with semaglutide or tirzepatide, this part will sound familiar. The second mechanism is glucagon receptor activation, which increases your body's energy expenditure and promotes fat burning in the liver. Think of it as having two coordinated systems working together: one that reduces how much energy comes in, and another that increases how much energy goes out.
This dual approach is what sets survodutide apart from pure GLP-1 drugs. The glucagon component is especially relevant for people dealing with metabolic dysfunction-associated steatohepatitis (MASH, formerly called NASH), a form of fatty liver disease where the liver accumulates excess fat and becomes inflamed. Survodutide's ability to directly promote fat burning in the liver makes it a promising candidate for this condition, which currently has very limited treatment options.
Survodutide is being developed by Boehringer Ingelheim in partnership with Zealand Pharma. Phase 2 clinical trials showed weight loss of up to 18.7% over 46 weeks, and Phase 3 programs (SYNCHRONIZE for obesity, THUNDER for MASH) are currently underway.
The Science
Survodutide (BI 456906) is a synthetic unimolecular dual agonist derived from a glucagon backbone with modifications to confer GLP-1 receptor (GLP-1R) co-activity. The compound activates both the glucagon receptor (GCGR) and the GLP-1R, with an in vitro potency ratio of approximately 1:8 (GCGR to GLP-1R) [1]. A C-terminal fatty acid modification enables reversible albumin binding, extending the plasma half-life to approximately 10-14 days and supporting once-weekly subcutaneous dosing [2].
The peptide was developed through a collaboration between Zealand Pharma (molecular design) and Boehringer Ingelheim (clinical development). The preclinical pharmacology was characterized in Zimmermann et al. (2022), demonstrating robust anti-obesity efficacy in rodent models with simultaneous improvements in hepatic steatosis markers [2].
In the Phase 2 obesity trial (N=387), survodutide produced dose-dependent weight loss ranging from 6.2% (0.6 mg) to 18.7% (4.8 mg, based on actual doses received) compared to 2.3% with placebo over 46 weeks [3]. A separate Phase 2 trial in MASH (N=293) demonstrated histologic improvement in MASH without worsening fibrosis in 47-62% of participants across dose groups compared to 14% with placebo [4].
Multiple Phase 3 programs are active: SYNCHRONIZE-1 and SYNCHRONIZE-2 (obesity with and without T2D), SYNCHRONIZE-CVOT (cardiovascular outcomes), and THUNDER (MASH) [5][6][7].
Molecular Identity
Attribute
Common Names
- Detail
- Survodutide, BI 456906, BI-456906
Attribute
Molecular Formula
- Detail
- C192H289N47O61
Attribute
Molecular Weight
- Detail
- Approximately 4,500 Da (4.5 kDa)
Attribute
Structural Type
- Detail
- Acylated unimolecular dual agonist peptide; glucagon-derived backbone with GLP-1R co-activity
Attribute
Functional Class
- Detail
- Dual GLP-1R/GCGR agonist; incretin-based metabolic therapeutic
Attribute
Target Receptors
- Detail
- Glucagon receptor (GCGR) and GLP-1 receptor (GLP-1R)
Attribute
Developer
- Detail
- Boehringer Ingelheim (clinical development) / Zealand Pharma (molecular design)
Mechanism of Action
The Basics
Survodutide works by flipping two metabolic switches at once. The first switch, GLP-1 receptor activation, tells your brain that you are full, slows down how quickly food moves through your stomach, and helps your body manage blood sugar more effectively. This is the same mechanism that makes drugs like semaglutide effective for weight loss.
The second switch, glucagon receptor activation, does something different. It tells your body to burn more energy, particularly by promoting fat breakdown in the liver. Your liver is one of the main organs responsible for processing and storing fat, and the glucagon signal essentially tells it to use stored fat as fuel rather than continuing to accumulate it.
What makes this combination interesting is that these two mechanisms complement each other without canceling out. You might expect the glucagon component to raise blood sugar (since glucagon normally does that), but the GLP-1 component counterbalances this effect by stimulating insulin release. The net result is weight loss from both reduced calorie intake and increased calorie burning, with the added benefit of directly reducing liver fat.
The Science
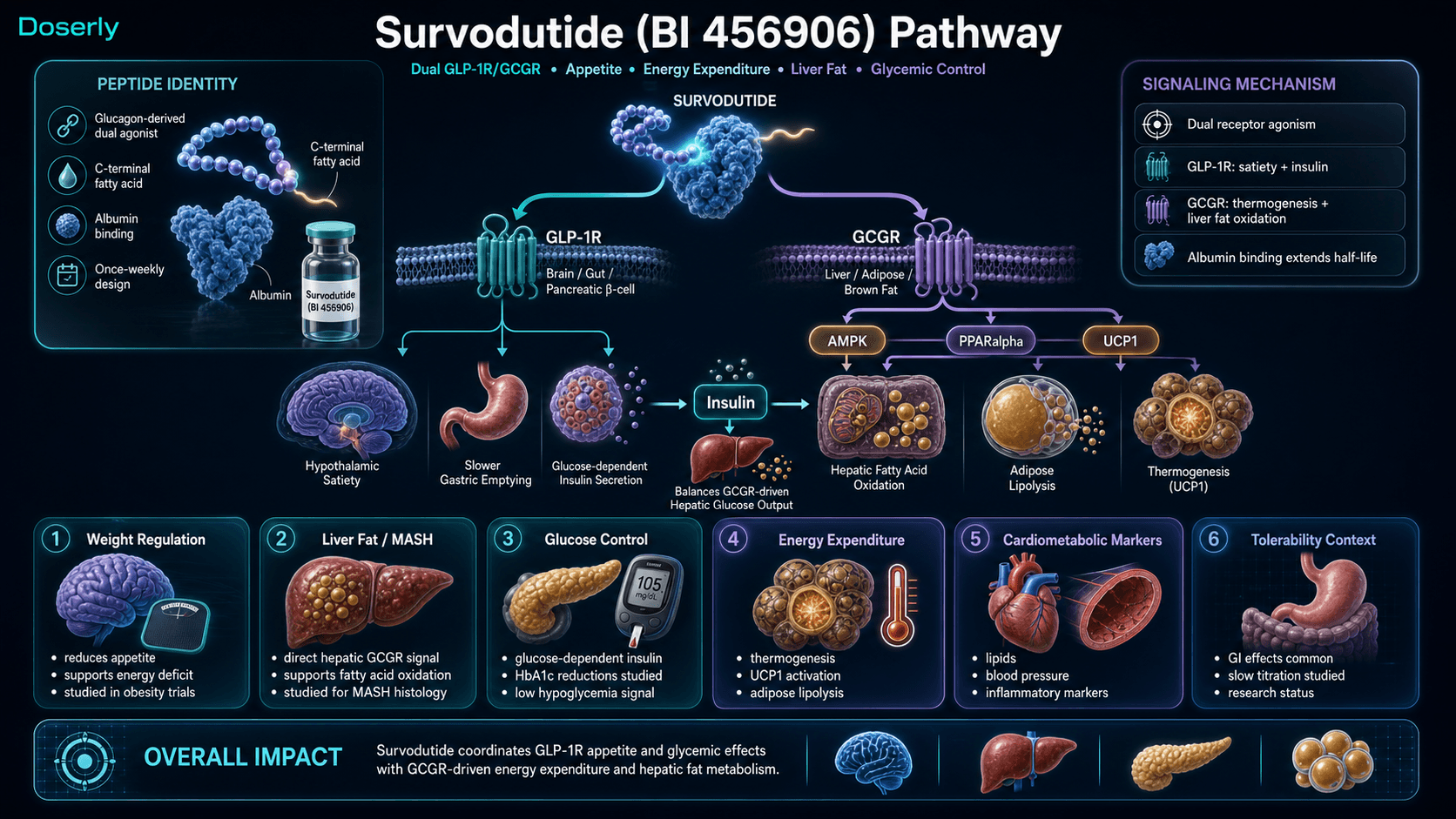
GLP-1R agonism mediates appetite suppression through hypothalamic signaling, delays gastric emptying via vagal afferent pathways, and enhances glucose-dependent insulin secretion from pancreatic beta cells [8]. These effects are well-characterized across the GLP-1 agonist drug class.
GCGR agonism activates complementary metabolic pathways: thermogenesis via brown adipose tissue uncoupling protein 1 (UCP1) activation, hepatic fatty acid oxidation through AMPK-dependent and PPARalpha-mediated pathways, enhanced adipose lipolysis, and potentially additional central appetite effects via hypothalamic GCGR expression [2][9]. The hepatic effect is particularly relevant for MASH, as hepatocytes lack GLP-1 receptors, meaning GLP-1 agonists can only reduce liver fat indirectly through systemic weight loss. GCGR agonism provides a direct hepatic mechanism [4].
The glucose homeostasis balance is managed through receptor interplay: GLP-1R-mediated glucose-dependent insulin secretion and glucagon suppression offset GCGR-mediated hepatic glucose output, preventing hyperglycemia in the context of dual receptor co-activation [2][9]. In Phase 2 trials, survodutide demonstrated dose-dependent HbA1c reductions in T2D populations without clinically significant hypoglycemia in non-diabetic cohorts [3][10].
In a preclinical mouse model, the dual GLP-1R/GCGR agonist mechanism ameliorated MASH by reducing inflammation, steatosis, apoptosis, and oxidative stress while simultaneously increasing mitochondrial biogenesis and liver regeneration [11].
Pathway Visualization Image
Pharmacokinetics
The Basics
Survodutide is designed for convenience. A fatty acid chain attached to the peptide allows it to bind to albumin (a protein in your blood), which dramatically slows its breakdown and elimination. The result is a half-life of roughly 10 to 14 days, meaning a single injection provides coverage for a full week with a comfortable margin.
After a subcutaneous injection, levels in the blood build gradually. Because the half-life is long, it takes several weeks of consistent weekly dosing for the compound to reach steady-state levels in your system. This is one reason why the dose escalation period spans 10 to 20 weeks: the body needs time to equilibrate, and gradual dose increases help manage tolerability.
The Science
Survodutide employs a fatty acid conjugation strategy (similar to semaglutide and tirzepatide) to achieve prolonged pharmacokinetics via non-covalent albumin binding. The estimated terminal half-life of approximately 10-14 days supports once-weekly subcutaneous administration [2][12].
Pharmacokinetic data from Phase 1 and Phase 2 studies demonstrate dose-proportional exposure across the tested dose range (0.3 to 6.0 mg). Steady-state concentrations are typically reached after 4-5 weeks of consistent weekly dosing. Subcutaneous bioavailability has not been precisely published but is consistent with the class (estimated 40-80% based on analogous GLP-1R agonist pharmacokinetics) [12].
Hepatic metabolism contributes to clearance, with renal elimination playing a minor role given the molecular weight (~4.5 kDa). Specific pharmacokinetic parameters in hepatically impaired populations (the primary MASH target) were evaluated in a dedicated cirrhosis cohort, which demonstrated acceptable tolerability and exposure [13].
Research & Clinical Evidence
The Basics
The clinical evidence for survodutide spans two main areas: obesity/weight management and fatty liver disease (MASH). Both have reached the point where Phase 3 trials are underway, which means the early data was promising enough for regulators to grant expedited development pathways.
For weight loss, Phase 2 data showed that people taking the highest dose lost an average of about 18.7% of their body weight over 46 weeks. More than half of participants in the highest dose group lost 15% or more. These numbers are competitive with other next-generation obesity treatments, falling between semaglutide (~15%) and retatrutide (~24%) in cross-trial comparisons.
For fatty liver disease, the results were equally encouraging. In a Phase 2 trial published in the New England Journal of Medicine, 47 to 62% of participants across dose groups showed improvement in liver disease without their scarring getting worse, compared to just 14% on placebo. This led to FDA Breakthrough Therapy designation in October 2024.
The Science
Obesity (Phase 2, N=387)
In the dose-finding Phase 2 trial, participants with BMI of 27 or greater (without T2D) received survodutide at 0.6, 2.4, 3.6, or 4.8 mg weekly for 46 weeks. Dose-dependent weight loss was observed: -6.2% (0.6 mg), -12.5% (2.4 mg), -13.2% (3.6 mg), and -14.9% (4.8 mg; -18.7% in the estimand based on actual doses received) versus -2.3% with placebo. At the 4.8 mg dose, 82.8% achieved at least 5% weight loss, 68.8% achieved at least 10%, and 54.7% achieved at least 15% [3].
A separate dose-response study in T2D patients demonstrated significant HbA1c reductions alongside weight loss, with survodutide outperforming semaglutide 1.0 mg at comparable timepoints [10].
MASH and Fibrosis (Phase 2, N=293)
Published in the New England Journal of Medicine (Sanyal et al., 2024), this 48-week trial randomized adults with biopsy-confirmed MASH and fibrosis stages F1-F3 to survodutide 2.4, 4.8, or 6.0 mg weekly versus placebo. The primary endpoint of histologic improvement in MASH without worsening fibrosis was achieved in 47% (2.4 mg), 62% (4.8 mg), and 57% (6.0 mg) versus 14% placebo. All secondary endpoints were also met, including improvements in fibrosis regression and hepatic fat reduction [4].
Cardiovascular (Phase 3 ongoing)
The SYNCHRONIZE-CVOT trial is evaluating cardiovascular outcomes in patients with obesity and established cardiovascular disease or high cardiovascular risk [7].
Meta-analyses
A meta-analysis by Wan et al. (2024) confirmed consistent weight-loss efficacy across multiple randomized controlled trials, supporting the robustness of the Phase 2 findings [14].
Biomarker Evidence Matrix
Category
Fat Loss
- Evidence Strength
- 8/10
- Reported Effectiveness
- 7/10
- Summary
- Phase 2 RCT demonstrates 12.5-18.7% weight loss (dose-dependent); community reports cite clinical data positively
Category
Weight Management
- Evidence Strength
- 8/10
- Reported Effectiveness
- 7/10
- Summary
- Consistent dose-dependent weight reduction across Phase 2 trials; maintenance dosing protocols under investigation
Category
Appetite & Satiety
- Evidence Strength
- 7/10
- Reported Effectiveness
- 7/10
- Summary
- GLP-1R agonism provides well-established appetite suppression; clinical data supports dose-dependent effect
Category
Food Noise
- Evidence Strength
- 4/10
- Reported Effectiveness
- 6/10
- Summary
- GLP-1 class effect expected; limited survodutide-specific data; one community report supports food noise reduction
Category
Energy Levels
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- GCGR component expected to increase energy expenditure; community reports are mixed; caloric restriction may offset
Category
Nausea & GI Tolerance
- Evidence Strength
- 9/10
- Reported Effectiveness
- 3/10
- Summary
- Strong Phase 2 data: nausea 66%, diarrhea 49%, vomiting 41%; universal community consensus on GI challenges
Category
Digestive Comfort
- Evidence Strength
- 7/10
- Reported Effectiveness
- 3/10
- Summary
- GI adverse events well-documented in clinical trials; burping, diarrhea, constipation commonly reported
Category
Heart Health
- Evidence Strength
- 6/10
- Reported Effectiveness
- 6/10
- Summary
- Phase 2 secondary endpoints show cardiovascular marker improvements; SYNCHRONIZE-CVOT Phase 3 underway
Category
Heart Rate & Palpitations
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Community reports suggest favorable RHR profile vs. retatrutide/mazdutide; limited formal data
Category
Side Effect Burden
- Evidence Strength
- 8/10
- Reported Effectiveness
- 4/10
- Summary
- Well-characterized in Phase 2; 24.6% discontinuation rate; GI effects dominate during dose escalation
Category
Treatment Adherence
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- Once-weekly dosing favorable; slow titration schedule requires patience; limited direct community data
Category
Daily Functioning
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Limited data; GI effects during escalation can impact daily activities; generally manageable
Categories scored: 12
Categories with community data: 12
Categories not scored (insufficient data): Muscle Growth, Sleep Quality, Focus & Mental Clarity, Memory & Cognition, Mood & Wellbeing, Anxiety, Stress Tolerance, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Joint Health, Inflammation, Pain Management, Recovery & Healing, Physical Performance, Gut Health, Skin Health, Hair Health, Blood Pressure, Hormonal Symptoms, Temperature Regulation, Fluid Retention, Body Image, Immune Function, Bone Health, Longevity & Neuroprotection, Cravings & Impulse Control, Social Connection, Withdrawal Symptoms, Other
Benefits & Potential Effects
The Basics
The primary benefit of survodutide is significant weight loss. In clinical trials, the highest-dose groups lost nearly one-fifth of their body weight over about 11 months. This level of weight loss can meaningfully reduce the strain on joints, improve mobility, lower blood pressure, and improve overall metabolic health.
Beyond the scale, the liver benefits may be equally important. Many people carrying excess weight also have fatty liver disease without knowing it. Survodutide's glucagon component directly targets liver fat, and clinical data shows substantial improvement in liver inflammation and fat content. For people with diagnosed MASH, this represents a potential treatment in a field where few options currently exist.
Blood sugar management is another benefit. In studies involving people with type 2 diabetes, survodutide improved HbA1c levels alongside weight reduction, addressing both conditions simultaneously.
The potential cardiovascular benefits are being studied in an ongoing large-scale Phase 3 trial. Improvements in blood lipids and blood pressure were observed as secondary findings in the Phase 2 program.
The Science
Weight reduction: Dose-dependent weight loss of 6.2-18.7% versus 2.3% placebo over 46 weeks in non-diabetic adults with obesity (Phase 2, N=387). The dual mechanism (reduced caloric intake via GLP-1R plus increased energy expenditure via GCGR) is hypothesized to produce additive or synergistic effects exceeding GLP-1R monoagonism [3].
Hepatic fat reduction and MASH improvement: In the Phase 2 MASH trial, survodutide achieved improvement in MASH histology without worsening fibrosis in 47-62% of participants versus 14% placebo. Up to 83% of participants in certain responder analyses showed improvement. The GCGR component provides direct hepatic mechanism via fatty acid oxidation independent of systemic weight loss [4].
Glycemic control: In T2D populations, survodutide produced dose-dependent HbA1c reductions exceeding semaglutide 1.0 mg at comparable timepoints, with low hypoglycemia risk in non-diabetic populations [10].
Cardiovascular markers: Phase 2 data showed improvements in lipid profiles, blood pressure, and inflammatory markers as secondary endpoints [3]. The SYNCHRONIZE-CVOT Phase 3 trial will provide definitive cardiovascular outcome data [7].
Side Effects & Safety Considerations
The Basics
The most important thing to understand about survodutide's side effects is that they are heavily concentrated in the gastrointestinal system and heavily concentrated in the early weeks of treatment during dose escalation.
Nausea is the most common side effect, reported by roughly two-thirds of participants in clinical trials. Diarrhea affects about half, and vomiting about 40%. These numbers are notably higher than some pure GLP-1 drugs, likely because the dual receptor activation amplifies GI signaling. The practical reality is that most people experience some degree of GI discomfort when starting survodutide.
The good news is that slow, gradual dose titration significantly reduces the severity and duration of these effects. Most GI symptoms peak during the dose escalation phase and improve as the body adjusts to each new dose level. This is why published protocols emphasize patience with the titration schedule, increasing by small increments every one to two weeks rather than jumping to higher doses quickly.
About one in four clinical trial participants discontinued treatment, predominantly during the dose escalation phase. Serious adverse events were reported at rates similar to placebo in the obesity trial.
Standard GLP-1 class warnings also apply: potential risk of gallbladder disease with substantial weight loss, theoretical pancreatitis signal based on class experience (not specifically elevated with survodutide), and caution in individuals with a personal or family history of medullary thyroid carcinoma or MEN2 syndrome.
The Science
Phase 2 adverse event profile: Adverse events occurred in 91% of survodutide recipients versus 75% of placebo recipients. GI adverse events were the most frequent: nausea (approximately 66% in MASH cohort versus 23% placebo), diarrhea (approximately 49% versus 23%), and vomiting (approximately 41% versus 4%). These rates are dose-dependent and concentrated during the rapid dose-escalation phase of the trials [3][4].
Discontinuation: Approximately 24.6% of survodutide-treated participants discontinued treatment in the Phase 2 obesity trial, predominantly during the 20-week dose escalation period [3].
Serious adverse events: Rates of serious adverse events were similar between survodutide and placebo groups in the Phase 2 obesity trial. No unexpected safety signals were identified [3].
Cardiovascular safety: Phase 2 data did not show clinically significant increases in resting heart rate, which distinguishes survodutide from some other multi-receptor agonists (e.g., retatrutide) that have been associated with heart rate increases [3][15].
Hepatic safety: In the MASH population, liver enzyme improvements (ALT, AST) were observed alongside histologic improvement, suggesting hepatoprotective rather than hepatotoxic effects [4].
Glycemic safety: Hypoglycemia risk is low in non-diabetic populations. Monitoring is recommended when survodutide is combined with other glucose-lowering agents [3][10].
Class warnings: Based on incretin class experience, standard precautions include monitoring for gallbladder disease symptoms with substantial weight loss, awareness of pancreatitis risk, and avoidance in individuals with personal or family history of medullary thyroid carcinoma or MEN2 syndrome until clarified in approval labeling [3].
The side effects and contraindications above give you a map of what to watch for. Doserly turns that map into a daily practice. Log the specific biomarkers and symptoms associated with this compound's known risk profile, and the app builds a timeline of how your body is responding across your cycle.
Trending in the wrong direction on a key marker? Noticing a pattern that started two weeks into your protocol? Doserly connects the dots between your protocol timeline and your logged data, making it easier to spot emerging issues early and have informed, data-backed conversations with your healthcare provider about what's working and what needs attention.
Keep side effects, flags, and follow-up notes visible.
Doserly helps you document safety observations, side effects, medication changes, and follow-up questions so important context is not scattered.
Safety log
Flags and notes

Safety notes are not emergency guidance; seek medical help when appropriate.
Dosing Protocols
The Basics
Survodutide dosing follows one consistent pattern: start low, go slow, and give your body time to adjust. All clinical trial protocols use once-weekly subcutaneous injections with gradual dose escalation over many weeks.
The dose range spans from 0.6 mg at the starting level up to 6.0 mg at the highest studied maintenance dose. Getting from start to target takes 10 to 20 weeks depending on the protocol, with dose increases of 0.3 to 0.6 mg at intervals of one to two weeks. The patience required during this titration phase is perhaps the single most important practical consideration, as rushing the escalation is the primary driver of intolerable GI side effects.
Commonly reported titration approaches from available sources range from conservative (0.3 mg increments every two weeks, reaching 3.0 mg maintenance by approximately week 19) to standard (0.6 mg increments every two to four weeks, reaching 3.0 to 6.0 mg by weeks 11-17). Clinical trial designs used faster escalation schedules to reach target doses within the trial timeframe, but community protocols frequently favor slower titration to manage GI tolerability.
Some sources discuss maintenance dosing for individuals who wish to continue survodutide after reaching weight goals. The key consideration is finding the lowest effective dose that maintains benefits without excessive appetite suppression. Adequate caloric and protein intake becomes an important monitoring parameter during any sustained protocol. Coordination with a healthcare provider and certified nutritionist is strongly recommended for long-term use.
The Science
Phase 2 obesity trial doses: 0.6, 2.4, 3.6, and 4.8 mg weekly for 46 weeks with biweekly dose escalation [3]. A dose-response relationship was observed, with weight loss increasing at higher doses without evidence of a plateau, leading to the inclusion of 6.0 mg in Phase 3 programs [5].
Phase 2 MASH trial doses: 2.4, 4.8, and 6.0 mg weekly for 48 weeks, with a rapid-dose-escalation phase followed by a maintenance phase [4].
Phase 3 doses: The SYNCHRONIZE-1 trial randomizes participants to survodutide 3.6 mg, survodutide 6.0 mg, or placebo [5]. Stepwise titration over approximately 20 weeks is employed.
Research compound protocols: Community-derived protocols from practitioner sources suggest starting doses of 0.3 to 0.6 mg with increments of 0.3 to 0.6 mg every one to two weeks. Target maintenance doses range from 3.0 to 6.0 mg depending on individual response and tolerability. These protocols are not validated in clinical trials and should be discussed with a healthcare provider.
Protocol Source
Phase 2 Clinical Trial
- Starting Dose
- 0.6 mg
- Increment
- Varied
- Target
- 4.8 mg
- Timeline
- 20 weeks escalation + 26 weeks maintenance
Protocol Source
Phase 3 Clinical Trial
- Starting Dose
- Low (titration)
- Increment
- Stepwise
- Target
- 3.6 or 6.0 mg
- Timeline
- ~20 weeks escalation + 56 weeks maintenance
Protocol Source
Community Conservative
- Starting Dose
- 0.3 mg
- Increment
- 0.3 mg/2 weeks
- Target
- 3.0 mg
- Timeline
- 19+ weeks
Protocol Source
Community Standard
- Starting Dose
- 0.3 mg
- Increment
- 0.6 mg/2-4 weeks
- Target
- 3.0-6.0 mg
- Timeline
- 17+ weeks
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders

Reminder tracking supports consistency; it does not select a protocol for you.
What to Expect
Survodutide's effects unfold gradually over many weeks, largely tracking with the dose escalation schedule. The following timeline is drawn from clinical trial data and community reports.
Weeks 1-2 (Starting Dose: 0.3-0.6 mg)
Most people notice very little at the starting dose. Some report mild burping or slight changes in appetite, while others feel no different. This is expected. The low starting dose is designed to let your body begin adapting to the compound, not to produce dramatic effects. Clinical trial participants frequently reported wondering whether they received placebo during these early weeks.
Weeks 3-6 (Early Titration: 0.6-1.2 mg)
As doses increase, appetite suppression typically becomes noticeable. Food portions may naturally decrease. Some GI effects begin to appear at this stage, primarily mild nausea, particularly after meals. Staying well hydrated and eating smaller, more frequent meals can help manage these early effects.
Weeks 7-12 (Mid Titration: 1.2-2.4 mg)
This is often when meaningful weight loss becomes visible on the scale. The GI side effects may intensify briefly with each dose increase but typically improve within a few days at each new level. By this point, most people have developed a sense of how their body responds to dose increases and can better anticipate and manage side effects.
Weeks 13-20 (Approaching Maintenance: 2.4-6.0 mg)
Weight loss accelerates as the dose approaches the therapeutic range. In clinical trials, the most significant weight loss occurred during the maintenance phase after titration was complete. Energy levels may change as the glucagon receptor component becomes more prominent at higher doses. Liver enzyme markers typically begin improving in this period for individuals with fatty liver disease.
Weeks 20+ (Maintenance Phase)
With the dose stabilized, GI side effects generally diminish or resolve. Weight loss continues at a steady pace. In Phase 2 trials, weight loss had not plateaued at 46 weeks, suggesting continued benefit with longer treatment. Metabolic improvements (blood sugar, lipids, liver markers) tend to consolidate during this phase.
The week-by-week expectations above are drawn from research and community reports, but your experience will be uniquely yours. Doserly's biomarker tracking transforms those general timelines into personal data points you can actually see and measure.
Log the specific markers relevant to this compound, whether that's pain levels, energy, sleep quality, body composition, recovery time, or mood, and watch your own trend lines emerge over weeks and months. Did your key markers start shifting in week three, like the research suggests? Is your experience tracking with what the community reports, or diverging? Over time, this creates something more valuable than any guide: an evidence-based picture of how your body responds to this specific compound, at your specific dose, within your specific health context.
Turn symptom and safety notes into a clearer timeline.
Doserly helps you log doses, symptoms, and safety observations side by side so patterns are easier to discuss with a qualified clinician.
Pattern view
Logs and observations
Pattern visibility is informational and should be reviewed with a clinician.
Interaction Compatibility
Potentially Synergistic Combinations
- Tirzepatide: Some community members combine survodutide with tirzepatide to approximate the triple-receptor coverage of retatrutide (adding GIPR agonism from tirzepatide to survodutide's GLP-1R/GCGR agonism). This is an emerging, unvalidated practice sometimes called "ghetto reta" in community forums. No clinical data supports this combination, and it carries additive GI risk. Discuss with a healthcare provider before considering.
- NAD+: Metabolic support compound. NAD+ supplementation may support beta-oxidation pathways activated by GCGR agonism, similar to the rationale for combining NAD+ with retatrutide.
- Cagrilintide: Amylin analog with complementary appetite suppression mechanism. Some community interest in combining with GLP-1/glucagon agonists for enhanced satiety, though no survodutide-specific data exists.
Not Recommended Combinations
- Semaglutide: Overlapping GLP-1R agonism creates redundant mechanism with additive GI risk and no expected benefit.
- Retatrutide: Overlapping GLP-1R and GCGR agonism. Retatrutide already covers both of survodutide's receptor targets plus GIPR, making combination redundant and potentially dangerous from a GI tolerability standpoint.
- Mazdutide: Overlapping dual GLP-1R/GCGR mechanism. Essentially the same drug class with no rationale for combination.
- Other GLP-1R agonists (Orforglipron): Overlapping mechanism with additive side effect risk.
Monitoring Required
- Insulin or sulfonylureas: GCGR agonism may affect hepatic glucose output. Enhanced hypoglycemia monitoring required when combined with glucose-lowering agents.
Administration Guide
Survodutide is administered as a once-weekly subcutaneous injection. Consistency in timing (same day each week) and proper preparation are important for maintaining stable drug levels.
Materials typically required:
- Insulin syringes (U-100) or 1 mL Luer-lock syringes with appropriate needles
- Bacteriostatic water for reconstitution
- Alcohol swabs for vial stopper and injection site
- Sharps disposal container
Recommended reconstitution solution: Bacteriostatic water. A common reconstitution volume is 2.0 mL per 10 mg vial, producing a concentration of 5 mg/mL (5,000 mcg/mL). At this concentration, 1 unit on a U-100 insulin syringe equals 0.01 mL, which equals 50 mcg.
Timing considerations: No specific timing requirements relative to meals have been established for survodutide. Administration on the same day each week at a consistent time supports adherence. Injection should be on a day when GI side effects (if present) will be least disruptive to daily activities.
Post-administration care: Monitor for injection site reactions (redness, swelling, itching), which are generally mild and transient. During the dose escalation phase, particular attention should be paid to GI symptoms (nausea, vomiting, diarrhea). If GI side effects are persistent or severe, the prescribing healthcare provider should be consulted about potentially slowing the titration schedule.
Important note: For maintenance doses of 6.0 mg (120 units at 5 mg/mL concentration), the injection volume of 1.20 mL exceeds a standard 100-unit (1 mL) insulin syringe. In this case, a 1 mL or 3 mL Luer-lock syringe with an appropriate needle should be used, or the dose may be split into two separate injections.
Supplies & Planning
The following materials are typically associated with a survodutide protocol. Specific quantities depend on the prescribed dose and duration, which should be determined in coordination with a healthcare provider.
Peptide vials: Survodutide is commonly available as a 10 mg lyophilized powder. The number of vials needed depends entirely on the weekly dose and protocol duration. For reference, at a 5 mg/mL reconstitution concentration:
- An 8-week protocol at titrating doses may require approximately 2 vials
- A 12-week protocol may require approximately 3-4 vials
- A 16-week protocol at higher maintenance doses may require 5-7 vials
Syringes: One injection syringe per week (plus spares). For doses at or below 4.8 mg (96 units at 5 mg/mL), standard U-100 insulin syringes are sufficient. For 6.0 mg doses, 1 mL Luer-lock syringes are needed.
Reconstitution supplies: Bacteriostatic water (10 mL bottles), mixing syringes with larger-gauge needles for reconstitution.
Ancillary supplies: Alcohol swabs (2 per week: one for vial stopper, one for injection site), sharps container for needle disposal.
Storage supplies: Refrigerator access for reconstituted vials. Freezer access for long-term storage of unreconstituted vials.
Readers should consult the reconstitution calculator for precise preparation math based on their specific vial size and target concentration.
Storage & Handling
Lyophilized (unreconstituted) storage:
- Store at -20C or colder for long-term preservation
- Protect from light and moisture
- Minimize temperature fluctuations
- Allow vials to reach room temperature before opening to reduce condensation uptake
Reconstituted storage:
- Refrigerate at 2-8C (standard refrigerator temperature)
- Protect from light (store in original packaging or wrap in foil)
- Avoid repeated freeze-thaw cycles, which can degrade the peptide
- Use reconstituted solution within a reasonable timeframe (generally within the duration needed for a single vial at the current dose)
Handling best practices:
- Always use sterile technique when reconstituting and drawing doses
- Gently swirl or roll the vial to dissolve; never shake vigorously, as this can damage the peptide and cause foaming
- Inspect reconstituted solution for particles or discoloration before use
- Label each vial with the reconstitution date and concentration
- Dispose of needles and syringes in an approved sharps container
Lifestyle Factors
The following lifestyle considerations may complement a survodutide protocol based on clinical trial recommendations and general metabolic health principles.
Nutrition: GLP-1R agonists can substantially reduce appetite, making it important to prioritize nutrient-dense foods when you do eat. A protein-forward diet (at least 1.0-1.2 g protein per kg of target body weight daily) supports lean mass preservation during weight loss, which is particularly important given concerns about muscle loss with GLP-1 class agents. Smaller, more frequent meals may help manage GI side effects during dose escalation. Adequate fiber and hydration support digestive function.
Exercise: Resistance training is strongly recommended to preserve lean body mass during weight loss. In GLP-1 class studies, a significant portion of weight lost can be lean tissue (25-40% in some analyses), and resistance exercise is the primary countermeasure. Aerobic activity supports cardiovascular health and complements the metabolic benefits. Start or maintain an exercise routine before beginning the protocol if possible.
Hydration: Particularly important given the GI side effects. Nausea, vomiting, and diarrhea can all contribute to dehydration. Increased water intake is recommended throughout the protocol, with electrolyte supplementation if GI symptoms are persistent.
Sleep: Prioritize consistent sleep quality. Metabolic health, appetite regulation, and GI function are all influenced by sleep. Poor sleep can blunt the metabolic benefits of incretin therapy.
Monitoring: Regular monitoring of body weight, waist circumference, blood pressure, fasting glucose or HbA1c, lipid panel, and liver enzymes (ALT, AST) is recommended during any metabolic intervention. For individuals with known or suspected fatty liver disease, additional imaging (MRI-PDFF, FibroScan) and fibrosis markers (FIB-4, ELF) may be appropriate in coordination with a hepatologist.
Regulatory Status & Research Classification
United States (FDA):
- Approval status: Not approved for any indication
- FDA Fast Track designation: Granted May 2021 for obesity
- FDA Breakthrough Therapy designation: Granted October 2024 for non-cirrhotic MASH with liver fibrosis stages F2-F3
- Active clinical trials: SYNCHRONIZE-1 (NCT06066515, Phase 3, obesity without T2D), SYNCHRONIZE-2 (Phase 3, obesity with T2D), SYNCHRONIZE-CVOT (cardiovascular outcomes), THUNDER (Phase 3, MASH). See ClinicalTrials.gov for complete listing.
European Union (EMA):
- PRIME designation: Granted November 2023 for MASH
- Marketing authorization: Not granted; Phase 3 trials ongoing
Canada (Health Canada):
- No specific regulatory actions publicly reported as of March 2026
- Clinical trial sites active in Canada as part of the SYNCHRONIZE program
United Kingdom (MHRA):
- No specific regulatory actions publicly reported
Australia (TGA):
- Clinical trial sites active in Australia as part of SYNCHRONIZE-1
WADA Status: Not prohibited. Survodutide does not appear on the World Anti-Doping Agency Prohibited List.
Developer: Boehringer Ingelheim (clinical development and commercialization) in partnership with Zealand Pharma (molecular design and early development).
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is survodutide and how is it different from semaglutide?
Survodutide is a dual GLP-1/glucagon receptor agonist, meaning it activates two metabolic receptors instead of one. Semaglutide activates only the GLP-1 receptor. The added glucagon receptor activation in survodutide increases energy expenditure and promotes liver fat burning, which is why survodutide is being studied not just for obesity but specifically for fatty liver disease (MASH). In cross-trial comparisons, survodutide showed approximately 18.7% weight loss versus approximately 15% for semaglutide, though these are not head-to-head numbers and should be interpreted cautiously.
How does survodutide compare to retatrutide?
Retatrutide is a triple agonist (GLP-1/GIP/glucagon receptors), while survodutide is a dual agonist (GLP-1/glucagon receptors). Survodutide lacks GIP receptor agonism. In Phase 2 trials, retatrutide showed approximately 24% weight loss versus survodutide's approximately 18.7%, though these are cross-trial comparisons with different populations and durations. Both share the glucagon receptor component relevant for liver disease. Retatrutide is Eli Lilly's compound; survodutide is Boehringer Ingelheim's.
Is survodutide FDA-approved?
No. As of March 2026, survodutide is not approved by any regulatory authority for any indication. It is in Phase 3 clinical trials. FDA Fast Track and Breakthrough Therapy designations have been granted, which expedite the review process but do not guarantee approval.
What are the most common side effects?
Gastrointestinal effects dominate: nausea (approximately 66%), diarrhea (approximately 49%), and vomiting (approximately 41%) based on Phase 2 MASH trial data. These are consistent with the GLP-1 drug class and are most severe during the dose escalation phase. Gradual titration significantly reduces severity.
What doses are being studied?
Phase 2 trials tested 0.6 to 6.0 mg weekly. Phase 3 trials use 3.6 mg and 6.0 mg as the target maintenance doses with gradual titration over approximately 20 weeks. Community-derived protocols suggest various titration schedules, but these are not validated in clinical trials. Any dosing decisions should be made in consultation with a healthcare provider.
Does survodutide help with fatty liver disease?
Phase 2 data published in the New England Journal of Medicine showed that 47-62% of participants with biopsy-confirmed MASH had histologic improvement without worsening fibrosis after 48 weeks of treatment, compared to 14% with placebo. A Phase 3 trial (THUNDER) is evaluating this further. The glucagon receptor component provides a direct liver fat-burning mechanism.
Does survodutide increase heart rate?
Based on available Phase 2 data, survodutide did not show clinically significant increases in resting heart rate. This is noted by community members as a potential advantage over retatrutide and mazdutide, which have been associated with heart rate increases. Definitive cardiovascular data will come from the Phase 3 SYNCHRONIZE-CVOT trial.
Can survodutide be combined with tirzepatide?
Some community members report combining survodutide with tirzepatide to approximate retatrutide's triple-receptor coverage. This is an unvalidated practice with no clinical data supporting safety or efficacy. The combination carries additive GI risk. Any combination therapy should be discussed thoroughly with a healthcare provider.
Sources & References
Clinical Trials (Human)
[1] Zimmermann T, Thomas L, Baader-Pagler T, et al. BI 456906: discovery and preclinical pharmacology of a novel GCGR/GLP-1R dual agonist with robust anti-obesity efficacy. Mol Metab. 2022;66:101633. PubMed
[2] Zimmermann T, et al. BI 456906: preclinical pharmacology characterizing the GCGR/GLP-1R dual agonist mechanism and albumin-binding pharmacokinetic profile. Mol Metab. 2022;66:101633.
[3] le Roux CW, Steen O, Lucas KJ, Startseva E, Unseld A, Hennige AM. Glucagon and GLP-1 receptor dual agonist survodutide for obesity: a randomised, double-blind, placebo-controlled, dose-finding phase 2 trial. Lancet Diabetes Endocrinol. 2024;12:162-73. PubMed
[4] Sanyal AJ, Bedossa P, Fraessdorf M, et al. A Phase 2 Randomized Trial of Survodutide in MASH and Fibrosis. N Engl J Med. 2024;391:311-319. DOI: 10.1056/NEJMoa2401755. PubMed ClinicalTrials.gov: NCT04771273.
[5] Wharton S, le Roux CW, Kosiborod MN, et al. Survodutide for treatment of obesity: rationale and design of two randomized phase 3 clinical trials (SYNCHRONIZE-1 and -2). Obesity. 2025;33(1):67-77. DOI: 10.1002/oby.24184.
[6] le Roux CW, Wharton S, Bozkurt B, et al. Survodutide for treatment of obesity: Baseline characteristics of participants in a randomized, double-blind, placebo-controlled, phase 3 trial (SYNCHRONIZE-1). Diabetes Obes Metab. 2026;28:337-346. DOI: 10.1111/dom.70196.
[7] Kosiborod MN, Platz E, Wharton S, et al. Survodutide for the treatment of obesity: rationale and design of the SYNCHRONIZE-CVOT trial. JACC Heart Fail. 2024.
Preclinical and Mechanistic Studies
[8] Drucker DJ. Mechanisms of Action and Therapeutic Application of Glucagon-like Peptide-1. Cell Metab. 2018;27(4):740-756.
[9] GLP-1/glucagon dual agonism: mechanistic overview and therapeutic potential. Nat Rev Endocrinol. 2023.
[10] Bluher M, et al. Dose-response effects on HbA1c and bodyweight reduction of survodutide in T2D. Diabetes Obes Metab. 2024.
[11] Valdecantos MP, Pardo V, Ruiz L, et al. A novel glucagon-like peptide 1/glucagon receptor dual agonist improves steatohepatitis and liver regeneration in mice. Hepatology. 2017;65:950-68.
[12] Guo H, et al. Efficacy, tolerability, and pharmacokinetics of survodutide, a glucagon/GLP-1 receptor dual agonist, in cirrhosis. J Hepatol. 2023.
Meta-analyses and Reviews
[13] Guo H, et al. Survodutide pharmacokinetics in cirrhosis cohort. J Hepatol. 2023.
[14] Wan H, et al. Meta-analysis of survodutide weight-loss efficacy across randomized controlled trials. Diabetol Metab Syndr. 2024.
[15] Vinton TY. Survodutide: a novel peptide for treatment of obesity and metabolic diseases. Proc (Bayl Univ Med Cent). 2025;38(4). PMCID: PMC12184103.
Related Peptide Guides
- Semaglutide - GLP-1 receptor agonist; the established benchmark for weight loss and metabolic therapy
- Tirzepatide - Dual GLP-1/GIP receptor agonist; complementary mechanism sometimes combined with survodutide by community members
- Retatrutide - Triple GLP-1/GIP/glucagon agonist; survodutide's closest mechanistic relative with added GIP component
- Mazdutide - Another dual GLP-1/glucagon agonist; same drug class as survodutide with different potency profile
- Cagrilintide - Amylin analog with complementary appetite suppression mechanism
- Orforglipron - Oral GLP-1 receptor agonist; non-injectable metabolic option
- NAD+ - Metabolic support compound; may complement GCGR-activated fat oxidation pathways
- 5-Amino-1MQ - NNMT inhibitor for metabolic enhancement
- AOD-9604 - Growth hormone fragment for fat loss
- MOTS-C - Mitochondrial peptide for metabolic health
- Tesamorelin - GHRH analog for visceral fat reduction and lean mass preservation
Need the reconstitution math for Survodutide: Complete Research Guide?
Open the calculator with Survodutide: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.