DSIP: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Delta Sleep-Inducing Peptide, Emideltide, DSIP nonapeptide, Deltaran
Attribute
Administration
- Detail
- Injectable (subcutaneous), Intranasal
Attribute
Research Status
- Detail
- Research Compound. No FDA Approval. FDA Category 2 for compounded injectables. Small European clinical trials (1980s-90s).
Attribute
Typical Dose Range
- Detail
- 100-300 mcg/day subcutaneous (some community reports up to 500 mcg)
Attribute
Half-Life
- Detail
- Short plasma half-life (minutes); biological activity estimated 6-8 hours
Attribute
Cycle Length
- Detail
- 4-12 weeks (commonly 8-12 weeks with 5 on / 2 off pattern); 4-8 week break between cycles
Attribute
Storage
- Detail
- Lyophilized: -20°C long-term; Reconstituted: 2-8°C (use within ~4 weeks)
Overview / What Is DSIP?
The Basics
DSIP stands for Delta Sleep-Inducing Peptide, a name that is somewhat misleading. Despite the name, DSIP does not knock you out or force sleep the way a prescription sleeping pill would. Instead, it works more like a volume knob for deep sleep. When your body is already winding down for the night, DSIP appears to amplify the signal, helping you achieve deeper, more restorative slow-wave sleep.
First discovered in 1977 in the brains of sleeping rabbits, DSIP is one of the oldest peptides in the research space. It gained attention because researchers noticed that animals in deep sleep had higher concentrations of this tiny nine-amino-acid molecule in their blood. Your body actually produces DSIP naturally, with levels rising in the late afternoon and falling by morning.
What makes DSIP different from common sleep aids is its circadian dependence. Taking it during the day does little. Taking it during the biological evening, when your body is already preparing for sleep, is when it appears to make a difference. This makes DSIP particularly interesting for people whose sleep depth has been degraded by stress, travel, or irregular schedules, while their overall sleep timing remains roughly intact.
Beyond sleep, early research suggests DSIP may help buffer stress hormones, modulate pain perception, and provide antioxidant support at the cellular level. However, the human evidence base is notably thin: most clinical data comes from small European trials conducted in the 1980s and 1990s, and research largely stopped when academic funding shifted elsewhere.
The Science
Delta sleep-inducing peptide (DSIP) is a nonapeptide (sequence: Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu) first isolated by Schoenenberger and Monnier in 1977 from the cerebral venous blood of rabbits during electrically induced sleep [1]. The molecule is endogenously produced, crossing the blood-brain barrier with concentrations varying according to circadian rhythm, higher in the late afternoon and evening, lower in the morning [2].
DSIP is classified as a neuromodulatory peptide with circadian-dependent effects on sleep architecture. In experimental models, it biases the brain toward deeper, more consolidated non-rapid eye movement (NREM) sleep, specifically slow-wave sleep (SWS), the phase most tightly linked to tissue repair, growth hormone secretion, and memory consolidation [3]. Its effects depend critically on timing relative to the circadian cycle, which distinguishes it from pharmaceutical hypnotics that force sedation regardless of timing.
Despite over four decades of intermittent study, the specific receptor through which DSIP exerts its primary effects has never been conclusively identified [4]. This gap between observable effects and molecular mechanism is unusual for a peptide with this degree of study and represents the most significant barrier to full mechanistic understanding.
The broader profile extends beyond sleep into stress hormone buffering (HPA axis modulation), pain modulation (opioidergic pathway interactions), antioxidant activity (reduced lipid peroxidation markers in brain tissue), and hormonal regulation (influences on LH and GH secretion patterns) [4][5].
Molecular Identity
Attribute
Common Names
- Detail
- DSIP, Delta Sleep-Inducing Peptide, Emideltide, Deltaran
Attribute
Amino Acid Sequence
- Detail
- Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu
Attribute
Single-Letter Code
- Detail
- WAGGDASGE
Attribute
Molecular Formula
- Detail
- C₃₅H₄₈N₁₀O₁₅
Attribute
Molecular Weight
- Detail
- 848.824 g/mol
Attribute
CAS Number
- Detail
- 62568-57-4
Attribute
PubChem CID
- Detail
- 68816
Attribute
Structural Type
- Detail
- Linear nonapeptide
Attribute
Source
- Detail
- Endogenous (found in mammalian brain tissue and plasma); synthetic versions available
Attribute
Discovery
- Detail
- 1977, Schoenenberger and Monnier, isolated from rabbit cerebral venous blood
Attribute
Functional Class
- Detail
- Neuromodulatory peptide; sleep architecture modulator; stress-axis modulator
Mechanism of Action
The Basics
To understand how DSIP works, think of sleep as having layers. There is light sleep, deep sleep (slow-wave sleep), and dream sleep (REM). Most pharmaceutical sleeping pills work by essentially shutting down the brain, like flipping a breaker switch. The problem is they suppress all layers indiscriminately, often reducing the deep, restorative sleep phases you actually need.
DSIP takes a different approach. Rather than forcing the brain offline, it appears to tip the balance in favor of deeper sleep once you are already in the process of falling asleep. Imagine your brain has a dial that controls how deep your sleep goes. DSIP turns that dial up, but only when the music is already playing. During the day, when your wakefulness systems are fully engaged, the same dose does essentially nothing.
DSIP also appears to help manage stress hormones. Cortisol, your body's primary stress hormone, normally drops in the evening to allow sleep. In people under chronic stress, cortisol stays elevated at night, keeping the brain in a heightened state that blocks deep sleep. DSIP seems to dampen this elevated evening cortisol, removing one of the barriers to restful sleep.
The Science
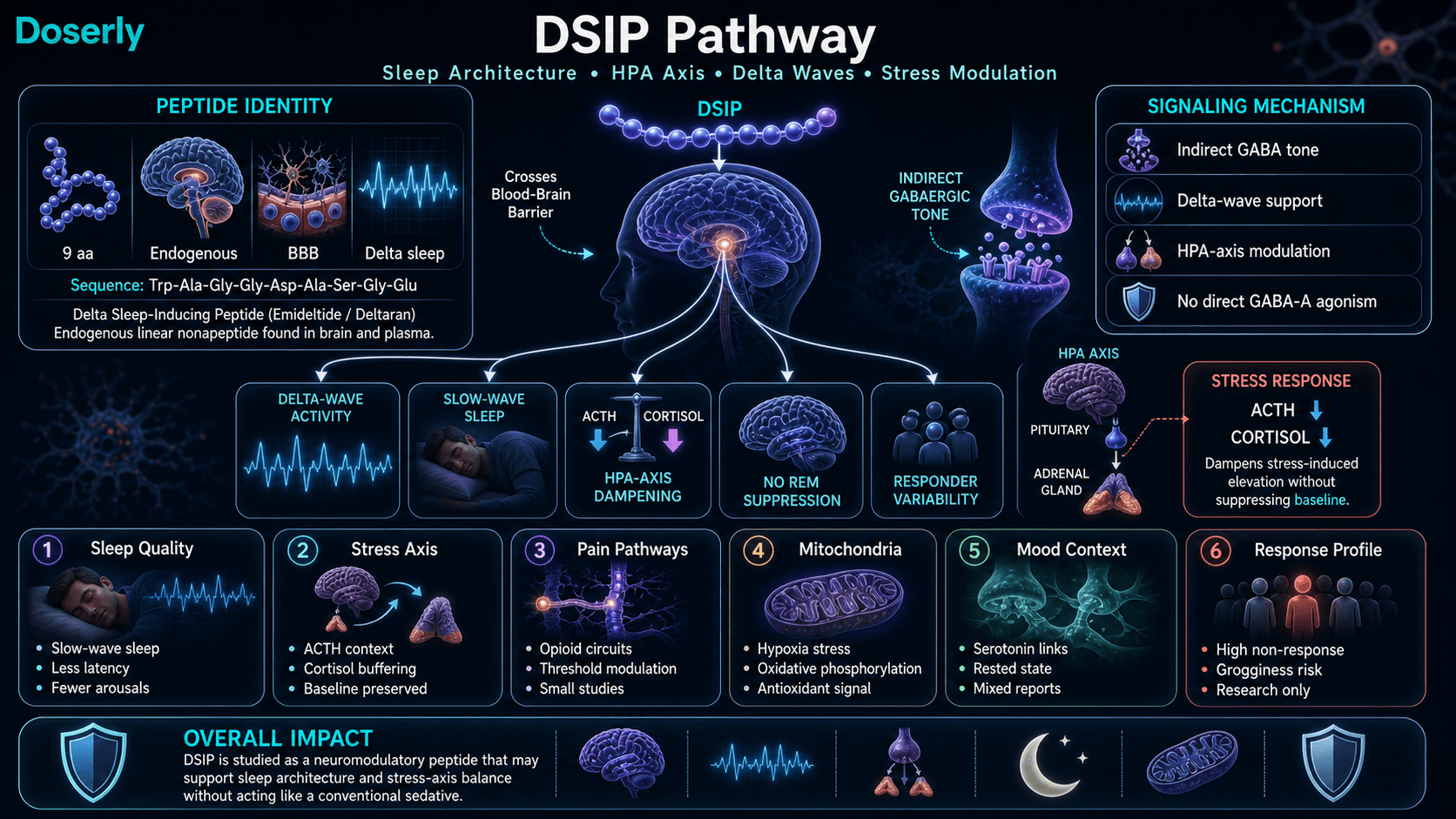
DSIP does not induce sleep through direct GABA-A receptor agonism, the mechanism employed by benzodiazepines and Z-drugs. Instead, available mechanistic data suggest it modulates GABAergic signalling indirectly, biasing GABAergic tone upward without acting as a direct receptor agonist [4].
The practical consequence is a shift in sleep architecture: increased proportion of slow-wave sleep, reduced sleep latency, and fewer nocturnal arousals. Electroencephalographic studies in both animals and humans demonstrate increased delta-wave activity following administration, without the suppression of REM sleep characteristic of most pharmaceutical sedatives [3].
HPA axis modulation: DSIP modulates the hypothalamic-pituitary-adrenal (HPA) axis. In animal models, administration is associated with dampening of stress-induced ACTH and cortisol elevation without suppressing baseline cortisol function [5]. Salieva et al. (1992) demonstrated that DSIP increases hypothalamic substance P and resistance to emotional stress in rats [6].
Opioid pathway interactions: DSIP modulates pain perception thresholds through engagement with endogenous opioidergic circuits. Research in rats indicates these effects are dose-dependent and operate through central opioid receptors, though the interaction appears indirect rather than involving direct receptor binding [4][7].
Antioxidant activity: In animal models, DSIP reduces markers of lipid peroxidation and enhances free radical scavenging enzyme activity in brain tissue. Bondarenko et al. (2011) proposed that these properties contributed to geroprotective effects in rat models [8]. DSIP also maintains oxidative phosphorylation in mitochondria under hypoxic stress conditions, suggesting a role in preserving cellular energy metabolism during oxygen deprivation [9].
Somatostatin inhibition: DSIP has been found to inhibit somatostatin, a protein produced in muscle cells that inhibits muscle growth. This effect on skeletal muscle hypertrophy and hyperplasia represents one of the less-explored aspects of the peptide's broad physiological profile [10].
Pathway Visualization Image
Pharmacokinetics
The Basics
DSIP has a very short life in the bloodstream. After injection, it is cleared from plasma within minutes. However, the biological effects, particularly on sleep architecture, appear to last for 6 to 8 hours. This means the peptide may trigger a cascade of downstream effects that persist well after the molecule itself has been metabolized.
This distinction between how long the peptide is measurable in blood versus how long its effects last is important. The short plasma half-life means precise injection timing matters. Most protocols suggest administering 30 to 60 minutes before the desired sleep onset. Some research suggests effects may persist for multiple nights after a single dose, though this finding is not consistent across all studies.
DSIP crosses the blood-brain barrier, which is essential for its central nervous system effects. The peptide is found naturally in both brain tissue and blood plasma, with concentrations following a circadian pattern.
The Science
DSIP exhibits a short plasma elimination half-life, with intravenous clearance occurring within minutes [11]. However, biological activity as measured by EEG changes and sleep architecture modifications persists for 6 to 8 hours following administration, suggesting downstream neuroendocrine cascading beyond the peptide's direct presence in circulation [3].
The peptide readily crosses the blood-brain barrier to exert central effects [11]. Endogenous DSIP concentrations demonstrate circadian variation, with higher levels in the late afternoon and evening, and lower levels in the morning, consistent with a physiological role in the wakefulness-to-sleep transition [2].
Some studies report that effects persist for multiple nights following dosing [11], though this finding is not universally replicated. The mechanism of such extended effects remains unclear and may involve downstream gene expression changes or neuroendocrine resetting rather than direct peptide activity.
Subcutaneous bioavailability in animal models is reported as excellent. Oral bioavailability is low due to gastrointestinal degradation [10].
Research & Clinical Evidence
DSIP and Sleep
The Basics
The relationship between DSIP and sleep is both the most studied and most debated aspect of this peptide. In clinical trials, results have been mixed. Some studies show clear improvements in sleep quality, particularly for people with chronic insomnia, while one well-designed double-blind trial found no significant effect. The overall picture is that DSIP may help normalize disrupted sleep rather than enhance already-normal sleep.
What the positive studies found was encouraging: people with chronic insomnia experienced fewer nighttime awakenings, better sleep efficiency, and improvements in both deep sleep and REM sleep. Subjective reports were even more positive, with participants reporting feeling sleepier, sleeping longer (up to 59% increase compared to placebo), and falling asleep faster.
Interestingly, the peptide does not appear to work like a sedative. Standard EEG measures of sedation, which were designed to detect drug-induced sedation, show no change. This may mean that DSIP promotes a natural form of sleep initiation that current testing methods were not designed to detect.
The Science
Schneider-Helmert et al. (1981): Six healthy volunteers received intravenous DSIP in a controlled setting. Subjects reported immediate sleep pressure, increased total sleep time, reduced sleep latency, and improved sleep efficiency. No sedative effects were detected. Next-day cognitive function was preserved [12].
Schneider-Helmert (1984): Ten patients with chronic insomnia showed statistically significant reductions in nocturnal arousals, increased sleep efficiency, and increases in both REM and slow-wave sleep. This is one of the few trials to demonstrate architectural improvement, not just increased sleep duration [13].
Schneider-Helmert (1992): Fourteen chronic insomniacs treated over seven nights showed increased sleep efficiency and decreased subjective tiredness to levels comparable to healthy controls. Effect sizes were modest, and the authors acknowledged inconsistency across endpoints [14].
The evidence presents a nuanced picture. Subjective sleep improvements are consistently reported across multiple trials, including feelings of sleepiness, longer perceived sleep duration, and faster sleep onset. Objective polysomnographic data is less consistent, with some trials showing clear architectural improvements and others showing no statistically significant changes. One well-designed double-blind trial by Monti et al. (1987) found no significant effects on any measured sleep parameter [15]. The overall evidence suggests DSIP may normalize disrupted sleep patterns, with effects more pronounced in individuals with existing sleep dysfunction than in healthy sleepers.
DSIP and Pain
The Basics
Early research suggests DSIP may help with chronic pain through a pathway similar to, but distinct from, the body's natural painkillers. In one small human trial, six out of seven patients with migraines and other chronic pain conditions experienced significant relief. Notably, DSIP does not appear to create the dependency problems associated with opioid pain medications, even though both interact with some of the same brain pathways.
The Science
Larbig et al. (1984) found that intravenous DSIP administration reduced chronic pain severity in six of seven patients with migraines, vasomotor headaches, and psychogenic pain episodes [7]. Animal studies demonstrate dose-dependent analgesic effects through central opioid receptors [16]. DSIP may also reduce withdrawal symptoms in patients with physiologic dependence on other pain medications [7][17].
DSIP and Withdrawal
The Basics
One of the more striking areas of DSIP research involves substance withdrawal. In a study of over 100 patients withdrawing from alcohol or opiates, DSIP treatment resulted in symptom improvement in 97% of alcohol-dependent patients and 87% of opiate-dependent patients. While these results are from a single study group and need replication, they suggest DSIP may have real value in managing the physiological crisis of withdrawal.
The Science
Dick et al. (1984) treated approximately 107 inpatients presenting with alcohol or opiate withdrawal syndromes with intravenous DSIP. Clinical symptoms of withdrawal improved in 97% of alcohol-dependent patients and 87% of opiate-dependent patients [17]. Opiate withdrawal proved more refractory, requiring more injections over a longer period. These results have not been independently replicated but align with the peptide's neuromodulatory profile across stress and opioid pathways.
DSIP and Metabolic Protection
The Basics
Research in animal models suggests DSIP can protect cells from the metabolic damage caused by oxygen deprivation, the kind of damage that occurs during a stroke or heart attack. It appears to help mitochondria (the energy factories inside cells) maintain normal function even under stressful conditions. This may make DSIP a potent antioxidant that works at a fundamental cellular level.
The Science
DSIP maintains oxidative phosphorylation in rat brain mitochondria under hypoxic conditions, preventing the metabolic shift to less efficient oxygen-independent respiration [9]. The peptide restricts changes in monoamine oxidase type A (MAO-A) and serotonin levels under hypoxic stress [18]. Analysis of cerebrospinal fluid in patients with major depression has revealed decreased DSIP levels compared to controls, suggesting a possible connection between endogenous DSIP and mood regulation [19].
DSIP and Cancer Research
The Basics
Preliminary animal research has explored DSIP as a potential cancer prevention tool. In one study, mice given monthly DSIP treatments showed dramatically fewer tumors over their lifetimes compared to untreated mice. The peptide also appears to protect the brain from some of the harmful effects of chemotherapy. These findings are very early-stage and have not been tested in humans.
The Science
In a longitudinal study, female mice receiving DSIP on 5 consecutive days per month from age 3 months showed a 2.6-fold decrease in spontaneous tumor development, accompanied by a 22.6% decrease in the frequency of chromosomal defects in bone marrow [20]. As a potential chemotherapy adjuvant, DSIP and its preparation Deltaran increased cerebral blood supply in animal models of ischemia. In one model, animals given Deltaran showed 100% survival compared to 62% in controls [21].
Biomarker Evidence Matrix
Category
Sleep Quality
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Small human trials (n=6-16) show inconsistent results; one negative double-blind trial exists. Community reports are polarized: dramatic improvements for responders, no effect for an estimated 30-50% of users.
Category
Stress Tolerance
- Evidence Strength
- 4/10
- Reported Effectiveness
- 6/10
- Summary
- Animal data supports HPA axis modulation. Small uncontrolled human trials report improved stress tolerance. Community reports note stress resilience improvements as a secondary benefit.
Category
Pain Management
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- One small human trial (n=7) showed 6/7 patients improved. Animal studies support dose-dependent analgesic effects via opioid pathways. Minimal community discussion.
Category
Mood & Wellbeing
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- Decreased CSF DSIP levels found in depressed patients. Animal data suggests MAO-A and serotonin modulation. Community mood improvements appear downstream of sleep quality changes.
Category
Cravings & Impulse Control
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Single study (n=107) showed 97% improvement in alcohol withdrawal and 87% in opiate withdrawal. Not independently replicated. Community data absent for this category.
Category
Energy Levels
- Evidence Strength
- 2/10
- Reported Effectiveness
- 5/10
- Summary
- No direct energy research. Community reports are mixed: responders feel more rested and energized; others report morning grogginess. Effects appear secondary to sleep quality.
Category
Side Effect Burden
- Evidence Strength
- 5/10
- Reported Effectiveness
- 7/10
- Summary
- No lethal dose identified in any animal model. Human trials report only transient headache, nausea, and grogginess. No dependency or withdrawal signals. Well-tolerated profile.
Category
Withdrawal Symptoms
- Evidence Strength
- 4/10
- Reported Effectiveness
- 7/10
- Summary
- No dependency signals in any published study. Community reports confirm no rebound insomnia or withdrawal effects upon cessation.
Category
Anxiety
- Evidence Strength
- 2/10
- Reported Effectiveness
- 5/10
- Summary
- Limited data. Indirect effects through cortisol dampening are plausible. Community reports are essentially neutral on anxiety.
Category
Longevity & Neuroprotection
- Evidence Strength
- 3/10
- Reported Effectiveness
- N/A
- Summary
- Animal data supports antioxidant activity, geroprotective effects, and tumor prevention. No human longevity data. Community data not collected for this category.
Categories scored: 10
Categories with community data: 8
Categories not scored (insufficient data): Fat Loss, Muscle Growth, Weight Management, Appetite & Satiety, Food Noise, Focus & Mental Clarity, Memory & Cognition, Motivation & Drive, Emotional Aliveness, Emotional Regulation, Libido, Sexual Function, Joint Health, Inflammation, Recovery & Healing, Physical Performance, Gut Health, Digestive Comfort, Nausea & GI Tolerance, Skin Health, Hair Health, Heart Health, Blood Pressure, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Fluid Retention, Body Image, Immune Function, Bone Health, Social Connection, Treatment Adherence, Daily Functioning
Benefits & Potential Effects
The Basics
The benefits most consistently discussed in connection with DSIP center on sleep quality. For people who respond to DSIP, the primary benefit is deeper, more restorative sleep with more time spent in slow-wave and REM phases. Users who track their sleep with devices like Oura Rings or Whoop bands sometimes report 30 to 40 extra minutes of deep and REM sleep per night.
Beyond sleep, DSIP may offer stress-buffering effects. Some users report feeling more resilient to daily stressors and notice that situations that previously felt overwhelming become more manageable. This likely connects to the peptide's ability to modulate cortisol dynamics.
Other potential benefits from the research literature, primarily from animal studies, include pain modulation, antioxidant protection at the cellular level, and possible protective effects against substance withdrawal symptoms. These benefits are less well-established in humans.
An important caveat: DSIP does not appear to work for everyone. Community reports and at least one clinical practitioner estimate that roughly half of users experience meaningful benefits, while the other half notice little to no effect. This is an unusually high non-response rate and should be factored into any decision.
The Science
Based on available research data, DSIP's potential effects include:
- Slow-wave sleep enhancement: Increased delta-wave activity on EEG without REM suppression [3][13]. Improved sleep efficiency and reduced nocturnal arousals in chronic insomniacs [14].
- Stress hormone buffering: Dampening of stress-induced cortisol elevation without suppressing baseline cortisol function. Increased hypothalamic substance P and stress resistance in animal models [5][6].
- Pain modulation: Dose-dependent analgesic effects via central opioid pathway interactions (animal models). Clinical improvement in 6/7 chronic pain patients in a small uncontrolled trial [7].
- Antioxidant and geroprotective activity: Reduced lipid peroxidation markers and enhanced free radical scavenging enzyme activity in brain tissue (animal models) [8].
- Withdrawal symptom management: 97% improvement in alcohol withdrawal, 87% in opiate withdrawal in a single clinical series (n=107) [17].
- Somatostatin inhibition: Potential effects on skeletal muscle via inhibition of the growth-limiting protein somatostatin (animal data) [10].
Side Effects & Safety Considerations
The Basics
DSIP has one of the cleaner safety profiles in the peptide space. No study in animals or humans has ever identified a lethal dose, and no serious adverse events have been reported across any published dataset. The most common side effect is morning grogginess, particularly at higher doses. Most users manage this by reducing the dose or taking it earlier in the evening (60 to 90 minutes before bed instead of 30 minutes).
Vivid or lucid dreams are reported frequently enough to be considered a characteristic effect rather than just a side effect. Some users find this enjoyable; others find the dreams unsettling, especially at higher doses.
Important safety considerations: DSIP should not be combined with alcohol, benzodiazepines, Z-drugs, or other sedatives due to overlapping mechanisms. People with suspected sleep apnea should address that condition first. DSIP should be avoided during pregnancy and breastfeeding. Do not drive or operate machinery until you understand your individual response to the peptide.
The Science
Pollard and Pomfrett (2001) conducted the most comprehensive safety review in the literature: no lethal dose was identified in any animal model, and human trials reported only transient headache, nausea, and occasional vertigo with no dependency, withdrawal, or organ toxicity signals [22].
Side Effect
Morning grogginess
- Likelihood
- Dose-dependent; more common at 200-300+ mcg
- Management
- Reduce dose or administer 60-90 min before bed
Side Effect
Vivid/lucid dreams
- Likelihood
- Commonly reported
- Management
- Not harmful; typically resolves or dose-reduce if distressing
Side Effect
Transient headache
- Likelihood
- Occasional
- Management
- Ensure adequate hydration; reduce dose if persistent
Side Effect
Nausea
- Likelihood
- Rare
- Management
- Administer on a light stomach; reduce dose
Side Effect
Next-day sedation
- Likelihood
- Rare; signals excessive dose
- Management
- Reduce dose by 50-100 mcg
Side Effect
Daytime drowsiness
- Likelihood
- Reported at higher doses, especially early in use
- Management
- Lower dose; may resolve with continued use
The FDA has placed DSIP on its Category 2 list of bulk drug substances that may present significant safety risks when used in compounding. The stated concern is immunogenicity, a class-level concern applicable to compounded injectable peptides generally, not a specific toxicity finding for DSIP [23]. No immunogenicity events have been reported in the published literature.
Contraindications: Concurrent use with sedative medications (benzodiazepines, Z-drugs, alcohol) is inadvisable due to overlapping GABAergic mechanisms. Not indicated for sleep disorders with underlying structural causes (obstructive sleep apnea, restless leg syndrome). Avoid during pregnancy and breastfeeding. Long-term continuous use has not been studied.
The side effects and contraindications above give you a map of what to watch for. Doserly turns that map into a daily practice. Log the specific biomarkers and symptoms associated with this compound's known risk profile, and the app builds a timeline of how your body is responding across your cycle.
Trending in the wrong direction on a key marker? Noticing a pattern that started two weeks into your protocol? Doserly connects the dots between your protocol timeline and your logged data, making it easier to spot emerging issues early and have informed, data-backed conversations with your healthcare provider about what's working and what needs attention.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
Dosing Protocols
The Basics
DSIP dosing is one area where the published research and community experience diverge somewhat. The research literature describes doses of 100 to 300 mcg per day, administered subcutaneously 30 to 60 minutes before desired sleep onset. Most clinical protocols suggest starting at 100 mcg for 2 to 3 nights to assess individual response, then increasing to 200 mcg if sleep latency remains above 30 minutes.
Community experience adds nuance. While the published literature uses 100 to 300 mcg, the most enthusiastic community reports tend to come from users at 350 to 500 mcg. Users who start at 100 mcg frequently report no noticeable effect, which has led some community members to suggest that the standard starting dose may be too low for many people. However, formal safety data above 300 mcg is limited, and higher doses are associated with increased morning grogginess.
An important pattern from community reports is that DSIP appears to lose effectiveness after 3 to 4 consecutive nights of use. Most protocols account for this with a 5-nights-on, 2-nights-off cycling pattern, or by using the peptide intermittently (3 to 4 nights per week). Continuous nightly use is not supported by the available data and may lead to diminishing returns.
Commonly reported parameters across sources include:
- Dose range: 100-300 mcg subcutaneous (community reports extend to 500 mcg)
- Timing: 30-60 minutes before desired sleep onset
- Frequency: 5 nights per week, or intermittent (3-4 nights per week)
- Cycle length: 4-12 weeks per course
- Break between cycles: 4-8 weeks
- Starting approach: Begin at 100-200 mcg for 2-3 nights; increase by 50 mcg increments as needed
- Intranasal route: 100-500 mcg, 15-30 min pre-bed, split between nostrils (less commonly reported)
The Science
Published research protocols have primarily utilized intravenous administration at 25 nmol/kg body weight [14], which translates to approximately 200-300 mcg for a 70-80 kg adult. Subcutaneous administration at 100-300 mcg has become the standard community and clinical practice approach, though no pharmacokinetic comparison study between routes exists [11][12][13].
Schneider-Helmert (1981) administered DSIP intravenously, producing immediate sleep pressure and increased total sleep time with no next-day cognitive impairment at the tested dose range [12]. The transition to subcutaneous self-administration represents a practical evolution that has not been formally validated against the original intravenous protocols.
Some studies indicate that DSIP does not induce pharmacological tolerance with continued use [11], though community reports of diminishing returns after 3-4 consecutive nights suggest practical tolerance or receptor downregulation may occur. The 5-on/2-off protocol widely adopted in the community addresses this pattern.
Consistency is the difference between a protocol that delivers results and one that wastes time and money. Doserly was built for exactly this: keeping you on track with the precision your protocol demands.
The built-in calculators handle the math you shouldn't be doing in your head. The reconstitution calculator tells you exactly how much bacteriostatic water to add for your target concentration. The dose calculator converts between units, milligrams, and syringe markings so you draw the right amount every time. The injection site heat map tracks where you've administered and when, helping you rotate sites systematically to reduce tissue damage, scarring, and absorption inconsistencies from overusing the same area. Pair that with smart reminders tuned to your protocol's timing requirements, and you build the kind of daily consistency that separates optimized protocols from haphazard ones.
Turn symptom and safety notes into a clearer timeline.
Doserly helps you log doses, symptoms, and safety observations side by side so patterns are easier to discuss with a qualified clinician.
Pattern view
Logs and observations

Pattern visibility is informational and should be reviewed with a clinician.
What to Expect
The timeline below reflects patterns drawn from published research and community reports. Individual responses to DSIP vary widely, and an estimated 30 to 50 percent of users may not experience meaningful effects at any dose. Those who do respond typically describe the following progression:
Days 1-3: Some users report noticeably deeper sleep from the first night, particularly at doses of 200 mcg or above. Vivid dreams are commonly reported early. Others notice little or no change, especially at starting doses of 100 mcg. Mild morning grogginess is possible as your body adjusts.
Days 4-7: If the peptide is working for you, deeper sleep patterns become more consistent. Sleep tracking devices may show increased time in deep and REM stages. Some users notice an initial decline in effectiveness around day 3 to 4 of consecutive use, which is why most protocols build in off-days.
Weeks 2-4: Sleep quality improvements, if present, stabilize. Users often report feeling more rested in the morning, with better energy and mood throughout the day. Stress resilience may improve as a secondary effect. The off-day cycling pattern (5 on / 2 off, or 3-4 nights per week) becomes important for maintaining effectiveness.
Weeks 5-8+: Continued benefits for responders. Some practitioners position DSIP as a circadian "reset" tool and suggest transitioning off after 8 to 12 weeks to see if sleep improvements persist. Some community reports suggest benefits can carry over for a period after stopping, while others note sleep quality returns to baseline within 1 to 2 weeks of cessation.
After stopping: No withdrawal symptoms or rebound insomnia has been reported in the literature or community. Sleep patterns typically return to baseline within 1 to 2 weeks. Some users report persistent vivid dreams for 1 to 2 days after the last dose.
The week-by-week expectations above are drawn from research and community reports, but your experience will be uniquely yours. Doserly's biomarker tracking transforms those general timelines into personal data points you can actually see and measure.
Log the specific markers relevant to this compound, whether that's pain levels, energy, sleep quality, body composition, recovery time, or mood, and watch your own trend lines emerge over weeks and months. Did your key markers start shifting in week three, like the research suggests? Is your experience tracking with what the community reports, or diverging? Over time, this creates something more valuable than any guide: an evidence-based picture of how your body responds to this specific compound, at your specific dose, within your specific health context.
Build reminders around the routine, not just the compound.
Doserly can keep timing, skipped doses, and schedule changes organized so the plan you read about becomes easier to follow and review.
Today view
Upcoming reminders
Reminder tracking supports consistency; it does not select a protocol for you.
Interaction Compatibility
Good With (Potentially Synergistic)
- Selank: Addresses the anxiety and cortical hyperarousal that can block sleep onset. Selank quiets the stress circuits, creating the conditions under which DSIP's sleep-architecture effects can express. Commonly recommended pairing (250-500 mcg Selank in the early evening, followed by DSIP at bedtime).
- Epithalon: Works upstream on the circadian system by supporting pineal function and endogenous melatonin secretion. Complements DSIP's downstream sleep-architecture modulation.
- Sermorelin: Growth hormone secretagogue that benefits from deeper slow-wave sleep. DSIP may potentiate GH pulse magnitude by extending the SWS window during which the largest nocturnal GH pulse occurs.
- Tesamorelin: Similar rationale to sermorelin. GH pulse potentiation during deeper slow-wave sleep phases.
- Ipamorelin: Another GH secretagogue that may benefit from the deeper SWS window DSIP creates.
- Pinealon: Protects the neural tissue that maintains circadian and sleep architecture long-term.
- BPC-157: Some community reports suggest pairing when pain disrupts sleep.
- KPV: Suggested if gut irritation contributes to nighttime disruption.
Not Good With (Use Caution)
- Benzodiazepines, Z-drugs (zolpidem, zopiclone): Overlapping GABAergic mechanisms create risk of excessive sedation. Do not combine.
- Alcohol: Compounds sedative effects and disrupts the sleep architecture DSIP is designed to improve.
- Other sedative medications: Additive central nervous system depression risk.
- MK-677: While not contraindicated, some people experience sleep disruption from GH secretagogues. Monitor if combining.
Administration Guide
Materials required:
- Insulin syringes (U-100; 30- or 50-unit syringes for small-volume doses in weeks 1-2)
- Alcohol swabs (for vial stopper and injection site)
- Bacteriostatic water for reconstitution
Recommended reconstitution solution: Bacteriostatic water. For a 5 mg vial, 3.0 mL bacteriostatic water yields a concentration of approximately 1.67 mg/mL (1 unit on a U-100 syringe equals approximately 16.7 mcg). For a 10 mg vial, 3.0 mL yields approximately 3.33 mg/mL (1 unit equals approximately 33.3 mcg).
Timing considerations: DSIP is administered in the evening, typically 30 to 60 minutes before the desired sleep onset. The circadian dependence of this peptide makes evening timing critical; daytime administration produces weaker or negligible effects. Some practitioners suggest administering slightly earlier (60 to 90 minutes before bed) if morning grogginess is experienced.
An intranasal route is also reported in some protocols, with doses split between nostrils 15 to 30 minutes before bed, though subcutaneous injection is the most commonly used and studied route.
Post-administration care: Monitor sleep quality and morning alertness. Consider tracking sleep with a wearable device to objectively measure changes in deep sleep and REM duration. If morning grogginess occurs, reduce the dose for the next administration. Keep a log of injection sites to maintain consistent rotation.
Supplies & Planning
Peptide vials: DSIP is commonly available in 2 mg, 5 mg, and 10 mg vial sizes. The appropriate vial size depends on the target dose and anticipated cycle length. Consult a healthcare provider for individualized guidance.
Syringes: U-100 insulin syringes. For smaller doses (under 10 units), 30-unit or 50-unit syringes offer improved readability and dosing precision compared to standard 100-unit syringes.
Reconstitution solution: Bacteriostatic water in 10 mL vials. Each vial reconstitution uses approximately 3.0 mL.
Alcohol swabs: Two per administration (one for the vial stopper, one for the injection site).
Sharps container: For safe syringe disposal.
Storage: A dedicated refrigerator space for reconstituted vials, protected from light.
For help calculating reconstitution volumes and dose measurements, use the Doserly reconstitution calculator.
Storage & Handling
Lyophilized (unreconstituted) powder:
- Long-term storage: -20°C (-4°F) in dry, dark conditions
- Short-term storage (weeks to months): 2-8°C (35.6-46.4°F) is acceptable
- Minimize moisture exposure; avoid repeated temperature cycling
Reconstituted solution:
- Refrigerate at 2-8°C (35.6-46.4°F)
- Use within approximately 4 weeks of reconstitution
- Avoid freeze-thaw cycles with reconstituted solution
- Protect from light
Handling best practices:
- Allow lyophilized vials to reach room temperature before opening to reduce condensation uptake
- Add reconstitution solution slowly down the vial wall to avoid foaming
- Gently swirl or roll the vial to dissolve; do not shake
- Always use sterile technique when accessing the vial
Lifestyle Factors
The effectiveness of DSIP is closely tied to the foundation of good sleep hygiene. Because the peptide amplifies existing sleep drive rather than generating it, the behavioral and environmental factors that support natural sleep become especially important.
Consistent sleep-wake schedule: Going to bed and waking at the same times daily, including weekends, reinforces the circadian rhythms that DSIP depends on to function.
Light exposure management: Bright light within 30 to 60 minutes of waking anchors the circadian oscillator. Dimming lights 2 hours before bed, particularly blue light from screens, supports the natural melatonin rise that works in concert with DSIP's effects.
Cool, dark sleep environment: Room temperature of 65 to 68°F (18 to 20°C) supports the core body temperature drop needed for sleep initiation. Complete darkness eliminates light cues that can fragment sleep architecture.
Caffeine timing: Caffeine has a 5 to 6 hour half-life. Eliminating caffeine by early afternoon prevents it from interfering with the sleep onset that DSIP is designed to support.
Meal timing: Avoid large meals within 3 hours of bed. Digestion keeps the body metabolically active and can blunt the growth hormone release that occurs during DSIP-enhanced deep sleep.
Physical activity: Regular exercise, ideally earlier in the day, increases sleep pressure and supports deeper slow-wave sleep. Intense exercise close to bedtime can interfere with the wind-down process.
Stress management: Because DSIP modulates the stress axis, complementary stress management practices (meditation, breathing exercises, journaling) may enhance its effectiveness by reducing the cortisol load that DSIP works to counteract.
Regulatory Status & Research Classification
United States (FDA): DSIP is not FDA-approved for any indication. It is classified as a research compound. The FDA has placed DSIP on its Category 2 list of bulk drug substances that may present significant safety risks when used in compounding, citing immunogenicity concerns applicable to compounded injectable peptides as a class [23]. DSIP's unpatentable nature (as a naturally occurring peptide) has historically limited commercial incentive for the large-scale clinical trials needed for FDA approval.
Canada (Health Canada): Not approved. No DIN or NPN assigned. Available through compounding pharmacies in some provinces.
United Kingdom (MHRA): Not approved as a medicine. Classified as an unlicensed substance. Available through some compounding and research chemical suppliers.
Australia (TGA): Not included on the Australian Register of Therapeutic Goods. Not scheduled under the TGA's scheduling framework for this specific compound.
European Union (EMA): No marketing authorization. Most clinical research on DSIP was conducted in European institutions (Switzerland, Germany) in the 1980s and 1990s, but this did not lead to regulatory applications.
WADA status: Not currently listed on the WADA Prohibited List.
Active clinical trials: No active clinical trials registered on ClinicalTrials.gov as of 2026. Research into DSIP largely ceased in the mid-1990s, not because safety signals emerged, but because academic interest and funding shifted elsewhere. A 2024 study describing a DSIP fusion peptide produced via Pichia pastoris expression represents one of the few recent additions to this research field [24].
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is DSIP?
DSIP (delta sleep-inducing peptide) is a nine-amino-acid neuropeptide first isolated in 1977. It modulates slow-wave sleep architecture, stress hormone dynamics, and pain perception. Despite its name, it does not force sedation. It biases the brain toward deeper NREM sleep in a circadian-dependent manner.
What are the benefits of DSIP?
Based on available research, DSIP may deepen slow-wave sleep, reduce sleep latency, buffer stress-induced cortisol elevation, and modulate pain perception. The strongest human evidence comes from small European trials showing improved sleep architecture in chronic insomniacs. Results in alcohol and opiate withdrawal (97% and 87% improvement respectively) are notable but come from a single study group.
Does DSIP actually work?
DSIP produces a polarized response pattern. Community reports and clinical observations suggest roughly half of users experience meaningful sleep improvements, while the other half notice little to no effect. One well-designed double-blind trial found no significant effects on any measured sleep parameter. For those who do respond, improvements in deep sleep and REM duration are consistently reported.
What dose of DSIP do most sources report?
Commonly reported ranges in the literature are 100 to 300 mcg subcutaneously, 30 to 60 minutes before desired sleep onset. Some community members report better results at 350 to 500 mcg, though safety data above 300 mcg is limited. Starting at 100 to 200 mcg and adjusting based on individual response is the most frequently cited approach. Always consult a healthcare professional for guidance on any protocol.
How does DSIP compare to melatonin?
They target different layers of sleep. Melatonin signals circadian timing (when to sleep). DSIP modulates sleep architecture (how deeply you sleep once you get there). Melatonin has vastly more clinical validation and is appropriate for jet lag and schedule shifting. DSIP is investigational with a thinner evidence base, potentially useful when sleep depth is the specific deficit.
Is DSIP safe?
No lethal dose has been identified in any animal model. Human trials report only transient headache, nausea, and occasional grogginess, with no dependency, withdrawal, or organ toxicity signals. The FDA placed DSIP on its Category 2 list due to class-level immunogenicity concerns for compounded injectables, not based on DSIP-specific toxicity data. Long-term use has not been studied. Consult a healthcare professional before use.
Can DSIP be taken with other peptides?
DSIP is commonly paired with Selank (for anxiety-gating at sleep onset) and growth hormone secretagogues like sermorelin, tesamorelin, or ipamorelin (which may benefit from the deeper slow-wave sleep window DSIP creates). It should not be combined with sedative medications, benzodiazepines, or alcohol. Discuss any combination protocol with a healthcare provider.
How long does DSIP take to work?
Some users report effects from the first night, particularly at doses of 200 mcg or above. Others notice improvements developing over the first week. The peptide does not help everyone, and users who see no effect after 1 to 2 weeks at adequate doses are unlikely to respond. Effects may diminish after 3 to 4 consecutive nights of use, which is why cycling protocols are commonly recommended.
Sources & References
Clinical Trials and Human Studies
[1] Schoenenberger GA, Monnier M. "Characterization of a delta-electroencephalogram (-sleep)-inducing peptide." Proc Natl Acad Sci USA. 1977. PubMed: 265573.
[3] Schneider-Helmert D, Schoenenberger GA. "The influence of synthetic DSIP on disturbed human sleep." Experientia. 1983;39(1):53-55. PubMed: 1603268.
[7] Larbig W, et al. "Therapeutic effects of delta-sleep-inducing peptide (DSIP) in patients with chronic, pronounced pain episodes." Eur Neurol. 1984;23(5):372-385.
[12] Schneider-Helmert D, et al. "Acute and delayed effects of DSIP (delta sleep-inducing peptide) on human sleep behavior." Int J Clin Pharmacol Ther Toxicol. 1981;19(8):341-345. PubMed: 6895513.
[13] Schneider-Helmert D. "Effects of delta-sleep-inducing peptide on 24-hour sleep-wake behaviour in severe chronic insomnia." Eur Neurol. 1984;23(5):358-363. PubMed: 6391925.
[14] Schneider-Helmert D, et al. "Effects of delta sleep-inducing peptide on sleep of chronic insomniac patients. A double-blind study." Pharmacopsychiatry. 1992. PubMed: 1299794.
[15] Monti JM, et al. "Sleep effects of DSIP in man: a double-blind study." Int J Clin Pharmacol Res. 1987;7(2):105-110. PubMed: 3583493.
[17] Dick P, et al. "DSIP in the treatment of withdrawal syndromes from alcohol and opiates." Eur Neurol. 1984;23(5):364-371.
[19] "Decreased concentrations of delta-sleep inducing peptide in plasma and cerebrospinal fluid from depressed patients." Nordisk Psykiatrisk Tidsskrift. Vol 39, sup11.
Reviews and Comprehensive Assessments
[4] Graf MV, Kastin AJ. "Delta-sleep-inducing peptide (DSIP): a review." Neurosci Biobehav Rev. 1984;8(1):83-93. PubMed: 6389048.
[5] Schneider-Helmert D, Schoenenberger GA. "Effects of DSIP in man: multifunctional psychophysiological properties." Neuropsychobiology. 1983;9(4):197-206. PubMed: 6319012.
[11] Pollard BJ, Pomfrett CJD. "Delta sleep-inducing peptide." Eur J Anaesthesiol. 2001;18:419-422.
[22] Pollard BJ, Pomfrett CJD. "Delta sleep-inducing peptide." Eur J Anaesthesiol. 2001;18:419-422. (Safety review: no lethal dose identified in any animal model; no significant side effects in human trials.)
Animal and In-Vitro Studies
[2] Sudakov KV, et al. "Delta-sleep-inducing peptide sequelae." Ann N Y Acad Sci. 1995. PubMed: 7485714.
[6] Salieva RM, et al. "Delta-sleep-inducing peptide increases hypothalamic substance P and resistance to emotional stress." Neurosci Behav Physiol. 1992;22(4):275-279. PubMed: 1382246.
[8] Bondarenko TI, et al. "Mechanism of geroprotective action of delta sleep-inducing peptide." Adv Gerontol. 2011;1:328-339.
[9] "Delta sleep inducing peptide (DSIP): effect on respiration activity in rat brain mitochondria and stress protective potency under experimental hypoxia." PubMed: 12668217.
[10] "DSIP: the sleep peptide or an unknown hypothalamic hormone?" PubMed: 7817664.
[16] "Potent antinociceptive effect of centrally administered delta-sleep-inducing peptide (DSIP)." PubMed: 2853064.
[18] "Effects of delta-sleep inducing peptide (DSIP) and some analogues on the activity of monoamine oxidase type A in rat brain under hypoxia stress." PubMed: 7628639.
[20] "Effect of delta-sleep inducing peptide-containing preparation Deltaran on biomarkers of aging, life span and spontaneous tumor incidence." PubMed: 12782416.
[21] Sinyukhin AB, et al. "Delta sleep-inducing peptide analogue corrects the CNS functional state of children treated with antiblastomic therapy." Eur Neuropsychopharmacol. 2009;19:S681-S682.
Regulatory and Recent Research
[23] U.S. Food & Drug Administration. Category 2 Bulk Drug Substances. 2025.
[24] Li J, et al. "DSIP fusion peptide produced via Pichia pastoris expression." Front Pharmacol. 2024. DOI: 10.3389/fphar.2024.1439536.
Additional References
[25] Steiger A, et al. "Effects of GHRH and somatostatin on sleep EEG and nocturnal GH secretion." Neuroendocrinology. 1992;56(4):566-573. PubMed: 1361964.
[26] Mikhaleva II, Prudchenko IA, et al. "Delta sleep-inducing peptide modulates stress responses." Peptides. 2004. PubMed: 15084686.
[27] Yehuda S, Carasso RL. "DSIP: brain mechanisms and function." Int J Neurosci. 1988;38(3-4):345-353.
Related Peptide Guides
- Selank - Anxiolytic peptide commonly paired with DSIP for sleep onset support
- Epithalon - Pineal bioregulator that supports endogenous melatonin production upstream of DSIP's effects
- Pinealon - Neural tissue protector that maintains the infrastructure DSIP's architecture depends on
- Sermorelin - GH secretagogue that may benefit from DSIP-enhanced slow-wave sleep windows
- Tesamorelin - GH secretagogue with complementary pre-sleep administration timing
- Ipamorelin - Selective GH secretagogue for pairing with sleep-architecture support
- BPC-157 - Repair peptide suggested when pain disrupts sleep quality
- KPV - Anti-inflammatory peptide for gut-related sleep disruption
- MK-677 - GH secretagogue (note: some users report sleep disruption)
- VIP - Master circadian clock synchronizer operating at a different tier than DSIP
Need the reconstitution math for DSIP: Complete Research Guide?
Open the calculator with DSIP: Complete Research Guide prefilled to estimate concentration, draw volume, and related measurement math from the reconstitution details you already have.