Methylene Blue: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Methylthioninium chloride, MB, Basic Blue 9, Tetramethylthionine
Attribute
Administration
- Detail
- Oral (solution, capsule, sublingual); Intravenous (clinical settings only)
Attribute
Research Status
- Detail
- FDA-approved for methemoglobinemia (ProvayBlue). Off-label for vasoplegic syndrome and ifosfamide encephalopathy. Not approved for cognitive enhancement or mitochondrial support.
Attribute
Typical Dose Range
- Detail
- 0.5-4 mg/kg/day oral (wellness); 1-2 mg/kg IV (clinical)
Attribute
Half-Life
- Detail
- 5-6.5 hours (plasma); up to 24.7 hours (terminal, tissue redistribution)
Attribute
Cycle Length
- Detail
- 4-5 days on / 2 days off; or 4 weeks on / 2 weeks off (hormetic cycling)
Attribute
Storage
- Detail
- Powder/tablets: room temperature, dry, light-protected; Solution: 2-8°C after opening
Overview / What Is Methylene Blue?
The Basics
Methylene Blue is one of the oldest synthetic compounds still in active medical use. First created in 1876 as a textile dye, it was repurposed for medicine within 15 years when researchers discovered it could treat malaria. That discovery made it one of the first synthetic drugs ever used in humans, predating antibiotics by decades.
What makes Methylene Blue unusual in the supplement and biohacking world is that it is not a peptide, a hormone, or a natural compound. It is a synthetic dye, a small molecule with a molecular weight of just 319.85 g/mol. Its deep blue color is not incidental; the same chemical property that makes it blue (its ability to accept and donate electrons) is what gives it biological activity. When you take it, your body puts those electrons to work inside the mitochondria, the energy-producing structures in every cell.
The compound has a well-documented paradox at its core: at low doses, it acts as a potent antioxidant and mitochondrial enhancer. At high doses, it reverses course and becomes a pro-oxidant that generates the very damage it prevents at lower levels. This inverted U-shaped dose-response curve is one of the most important things to understand before considering Methylene Blue, because the difference between benefit and harm is determined almost entirely by dose.
Today, Methylene Blue is FDA-approved for one indication: the treatment of methemoglobinemia, a condition where hemoglobin cannot release oxygen properly. Beyond that approved use, it is being investigated for cognitive enhancement, neuroprotection, antidepressant effects, and mitochondrial support. These applications have generated significant interest in the longevity and biohacking communities, though large-scale human trials for these off-label uses remain limited.
The Science
Methylene Blue (3,7-bis(dimethylamino)phenothiazin-5-ium chloride; CAS 61-73-4) is a tricyclic phenothiazine compound first synthesized by Heinrich Caro at BASF in 1876. Paul Ehrlich recognized its selective tissue affinity in 1891 and pioneered its use as an antimalarial agent, coining the term "magic bullet" to describe its ability to concentrate preferentially in diseased tissues [1][2].
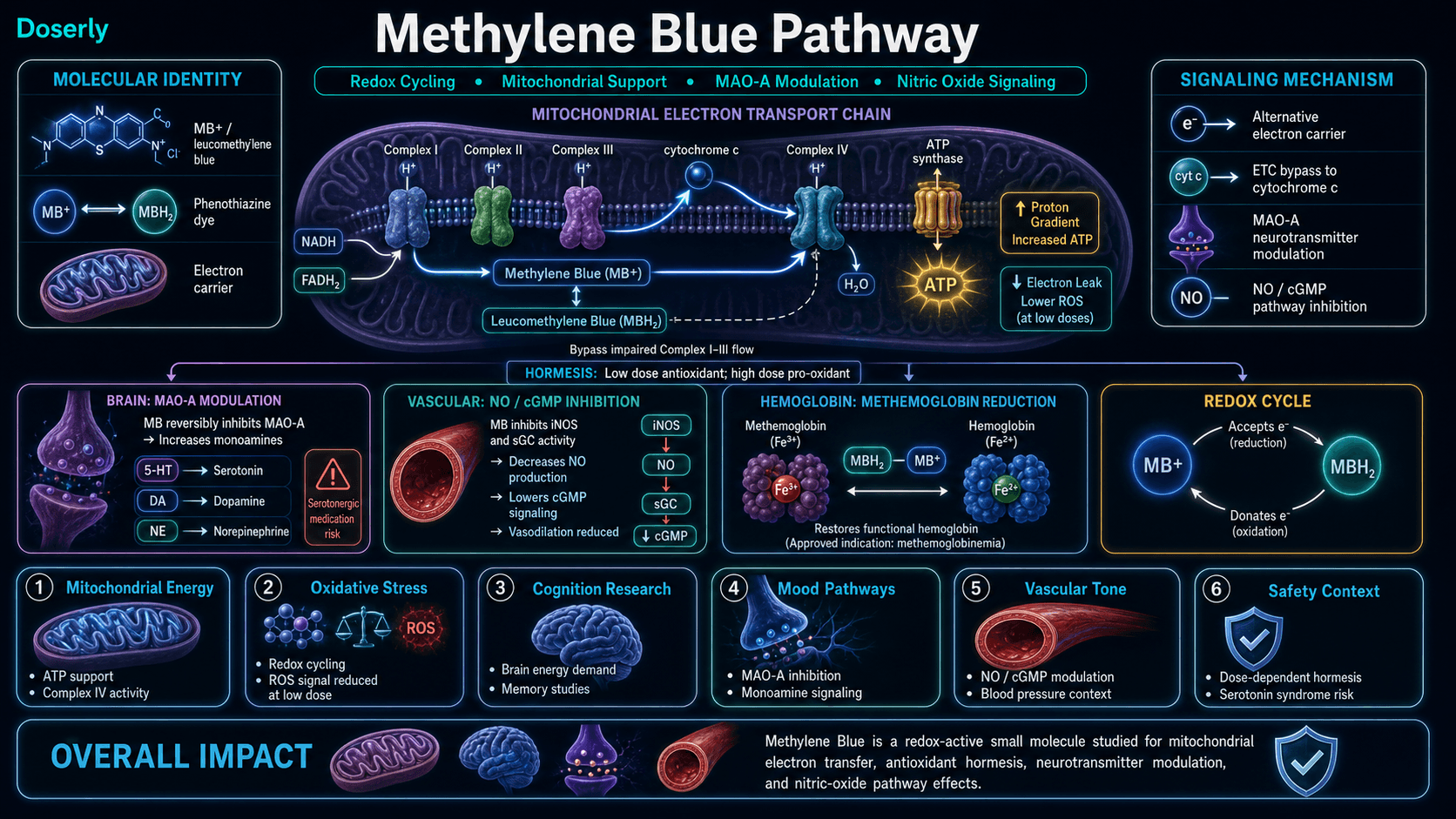
The compound's pharmacological versatility stems from its redox-active phenothiazinium core, which cycles between an oxidized form (methylene blue, blue) and a reduced form (leucomethylene blue, colorless). This redox cycling enables MB to function as an alternative electron carrier in the mitochondrial electron transport chain, accepting electrons from NADH and FADH2 and donating them directly to cytochrome c, effectively bypassing Complex I through III [3][4].
The hormetic dose-response is well-characterized: at concentrations of 10-100 nanomolar, MB donates electrons to the ETC, augmenting ATP synthesis and reducing reactive oxygen species (ROS) formation. At concentrations above approximately 2 micromolar, MB begins abstracting electrons from the ETC, generating superoxide and transitioning from antioxidant to pro-oxidant [5]. This biphasic response has been consistently demonstrated across in vitro, animal, and limited human studies.
MB also functions as a reversible monoamine oxidase A (MAO-A) inhibitor, inhibiting the enzymatic degradation of serotonin, dopamine, and norepinephrine [6]. This MAO inhibition underlies both its antidepressant potential and its most serious drug interaction risk: serotonin syndrome when combined with serotonergic medications.
Molecular Identity
Attribute
Chemical Name
- Detail
- 3,7-bis(dimethylamino)phenothiazin-5-ium chloride
Attribute
Molecular Formula
- Detail
- C16H18ClN3S
Attribute
Molecular Weight
- Detail
- 319.85 g/mol
Attribute
CAS Number
- Detail
- 61-73-4
Attribute
PubChem CID
- Detail
- 6099
Attribute
DrugBank ID
- Detail
- DB09241
Attribute
ATC Code
- Detail
- V03AB17
Attribute
Chemical Class
- Detail
- Phenothiazine (tricyclic)
Attribute
Redox Forms
- Detail
- Oxidized (blue, MB+) / Reduced (colorless, leucomethylene blue)
Attribute
Key Metabolite
- Detail
- Azure B (N-demethylated product)
Mechanism of Action
The Basics
The simplest way to understand how Methylene Blue works is to think of your mitochondria as a factory assembly line that converts food into cellular energy (ATP). This assembly line has several stations (Complexes I through V), and electrons pass from one station to the next like products moving down the belt. When a station breaks down or gets sluggish, the entire line slows, your cells produce less energy, and leftover electrons escape to form damaging free radicals.
Methylene Blue acts like a bypass conveyor that can carry electrons around broken stations. At low doses, it picks up electrons from the beginning of the line and delivers them further down, keeping the factory running even when some stations are impaired. This means more energy production and fewer free radicals simultaneously.
Beyond the mitochondrial factory, Methylene Blue also affects brain chemistry. It slows the breakdown of several neurotransmitters, including serotonin, dopamine, and norepinephrine, by inhibiting the enzyme (monoamine oxidase A) responsible for clearing them. This is the same mechanism used by a class of antidepressant medications called MAO inhibitors, which is why Methylene Blue can influence mood, focus, and motivation, and why it carries similar interaction risks.
Additionally, MB blocks the production of nitric oxide (a molecule that relaxes blood vessels), which is why it can raise blood pressure and why it is used in hospital settings to treat dangerously low blood pressure after heart surgery.
The Science
Methylene Blue exerts its biological effects through four primary mechanisms:
1. Alternative Mitochondrial Electron Transfer
MB accepts electrons from NADH via Complex I and from FADH2 via Complex II, then donates them directly to cytochrome c at Complex IV, bypassing the Q cycle and Complex III entirely [3][4]. This short-circuit of the electron transport chain has two consequences: it maintains the proton gradient driving ATP synthase even when upstream complexes are dysfunctional, and it reduces electron leakage that generates superoxide radicals. At nanomolar concentrations (10-100 nM), this mechanism enhances mitochondrial Complex IV activity by approximately 30% and cellular oxygen consumption by 37-70% [7].
2. Antioxidant and Redox Cycling
MB catalytically cycles between its oxidized and reduced forms, intercepting superoxide radicals at their point of generation within mitochondria. Unlike conventional antioxidants that are consumed stoichiometrically (one molecule neutralizes one radical), MB acts catalytically, with each molecule neutralizing multiple radicals through continuous redox cycling [4][5]. MB also reduces peroxynitrite (ONOO-) formation by limiting nitric oxide-superoxide interactions.
3. Monoamine Oxidase Inhibition
MB reversibly inhibits MAO-A with greater potency than MAO-B (Ki approximately 27 nM for MAO-A) [6]. This inhibition increases synaptic concentrations of serotonin, dopamine, and norepinephrine. The MAO-A inhibition becomes clinically significant at doses above approximately 1-2 mg/kg, creating the pharmacological basis for both antidepressant effects and serotonin syndrome risk.
4. Nitric Oxide Synthase and Guanylate Cyclase Inhibition
MB inhibits both inducible nitric oxide synthase (iNOS) and soluble guanylate cyclase (sGC), reducing cGMP-mediated vasodilation [8]. This mechanism underlies its clinical use in vasoplegic syndrome, where excessive NO production causes refractory hypotension. The same mechanism can elevate blood pressure in healthy individuals.
Additional mechanisms under investigation include acetylcholinesterase inhibition (with preference for muscarinic receptors) [9], tau aggregation inhibition via cysteine sulfhydryl oxidation [10], and upregulation of heme synthesis pathways [7].
Pathway Visualization
Pharmacokinetics
The Basics
How quickly Methylene Blue works and how long it lasts depends heavily on how you take it and what form you use. Taken as a liquid solution by mouth, it reaches peak blood levels in about 1 to 2 hours and stays active for roughly 5 to 6 hours. This is why most protocols suggest dosing in the morning or before cognitively demanding tasks, and why some protocols allow twice-daily dosing.
One of the most practically important facts about Methylene Blue is that its oral bioavailability varies enormously depending on the formulation. A liquid solution delivers about 72% of the compound into your bloodstream, while a capsule or tablet may deliver as little as 6.5%. This tenfold difference means that 10 mg from a solution could have a similar effect to 100 mg from a capsule, a distinction that is poorly appreciated in most consumer discussions.
Once in the bloodstream, Methylene Blue crosses the blood-brain barrier rapidly and concentrates in brain tissue at levels 10 to 20 times higher than in blood plasma. This preferential brain accumulation, first observed by Paul Ehrlich over a century ago, is what makes it relevant for cognitive and neurological applications.
The compound is metabolized primarily in red blood cells and peripheral tissues, converted to a colorless form called leucomethylene blue. About 75% is excreted through the kidneys, which is why urine turns blue or green, a harmless but startling effect.
The Science
Parameter
Oral bioavailability (solution)
- Value
- 72.3 ± 23.9%
- Source
- Walter-Sack et al., 2009 [11]
Parameter
Oral bioavailability (capsule)
- Value
- ~6.5-15%
- Source
- Formulation studies
Parameter
Tmax (oral solution)
- Value
- 1-2 hours
- Source
- Peter et al., 2000 [12]
Parameter
Plasma half-life
- Value
- 5-6.5 hours
- Source
- Peter et al., 2000 [12]
Parameter
Terminal half-life (tissue)
- Value
- 24.7 ± 7.2 hours
- Source
- EMA product information
Parameter
Volume of distribution
- Value
- ~20 mL/kg
- Source
- DiSanto & Wagner, 1972 [13]
Parameter
Brain:plasma ratio
- Value
- ~10-20:1
- Source
- Multiple preclinical studies
Parameter
Protein binding
- Value
- 71-77%
- Source
- Rabbit plasma data
Parameter
Primary metabolism
- Value
- Reduction to leucomethylene blue
- Source
- Erythrocytes, peripheral tissues
Parameter
Active metabolite
- Value
- Azure B (N-demethylation)
- Source
- —
Parameter
Renal excretion
- Value
- ~74% (10 mg dose); 20-30% (100 mg dose)
- Source
- DiSanto & Wagner, 1972 [13]
Parameter
P-glycoprotein
- Value
- Inhibitor (in vitro)
- Source
- EMA data
Parameter
BBB penetration
- Value
- Yes (rapid, within minutes)
- Source
- Multiple studies
Parameter
Clearance
- Value
- 3.0 ± 0.7 L/min
- Source
- Clinical data
Renal impairment significantly affects MB pharmacokinetics: AUC increases by 52% in mild (eGFR 60-89), 116% in moderate (eGFR 30-59), and 192% in severe (eGFR 15-29) renal impairment. Hepatic impairment increases AUC by 35-81% depending on severity (Child-Pugh classification).
Research & Clinical Evidence
The Basics
Methylene Blue has more than a century of medical history, but its research profile is uneven. For its approved use (methemoglobinemia), the evidence is strong and well-established. For cognitive enhancement and neuroprotection, the picture is more nuanced: a handful of promising human studies exist alongside a much larger body of animal and cell research.
The strongest human evidence comes from a study of 248 elderly surgical patients, where a single intravenous dose of Methylene Blue reduced the rate of postoperative delirium (a form of acute cognitive dysfunction) by 76%. This is a striking result from a well-designed randomized controlled trial, though it used an IV dose in a hospital setting, not the oral supplementation that most people are interested in.
For memory enhancement in healthy people, a single study of 26 volunteers found that a one-time oral dose improved short-term memory by about 7% on brain imaging measures. This is encouraging but limited to one study with a small sample size.
The antidepressant evidence is older but consistent. Studies from the 1980s and 2010s found that Methylene Blue improved depression symptoms, particularly in severe depression and bipolar disorder, at doses ranging from 15 to 300 mg per day. These results make pharmacological sense given its MAO inhibitor mechanism.
For Alzheimer's disease, clinical trials with a modified form of Methylene Blue (LMTM/TRx0237) produced disappointing Phase III results in 2016-2017, failing to show benefit when added to existing Alzheimer's medications. However, subgroup analyses suggested possible benefit in patients not on other Alzheimer's drugs. This is considered a hypothesis for further research rather than established evidence.
Animal and cell studies are extensive, demonstrating neuroprotection in models of Parkinson's disease, traumatic brain injury, stroke, and aging-related mitochondrial decline. These findings are mechanistically compelling but have not yet been confirmed in large-scale human trials for these indications.
The Science
Postoperative Cognitive Protection
A randomized, double-blind, placebo-controlled trial of 248 elderly patients undergoing major non-cardiac surgery demonstrated that a single 2 mg/kg intravenous dose of MB administered within one hour after anesthesia induction reduced postoperative delirium incidence from 24.2% to 7.3% (odds ratio 0.24, 95% CI 0.12-0.47, p<0.001) [14]. This remains the largest and most rigorous cognitive-outcome RCT for MB.
Memory Enhancement in Healthy Volunteers
A multimodal fMRI study of 26 healthy volunteers (aged 22-62) in a randomized, double-blind, placebo-controlled design found that a single 280 mg oral dose of MB increased fMRI activity during encoding in memory-related brain regions and improved short-term memory retrieval by approximately 7% compared to placebo (p<0.05) [15]. The effect was associated with increased cerebral blood flow and enhanced coupling between frontal and posterior cortical regions.
Fear Extinction and Anxiety
A controlled study found that post-session oral MB administration enhanced fear extinction and contextual memory retention at one-month follow-up in adults with claustrophobia [16]. This finding has implications for PTSD treatment paradigms.
Antidepressant Effects
A 1987 controlled trial found 15 mg/day MB was a significant antidepressant in severe depression [17]. A two-year double-blind crossover trial in 31 bipolar disorder patients found that 300 mg/day MB alongside lithium significantly reduced depression and mania compared to 15 mg/day [18]. A 2017 randomized crossover study found 195 mg/day MB combined with lamotrigine reduced residual depression and anxiety symptoms in bipolar disorder [19].
Alzheimer's Disease
MB inhibits tau aggregation through oxidation of cysteine sulfhydryl groups, keeping tau in a monomeric, non-pathological state in vitro [10]. However, Phase III trials of LMTM (leucomethylthioninium mesylate, a stabilized reduced form of MB) in mild-to-moderate Alzheimer's disease failed to meet primary endpoints when added to standard acetylcholinesterase inhibitor therapy (TauRx trials, 2016-2017). Post-hoc analyses suggested possible benefit as monotherapy, but this requires prospective confirmation [20].
Neuroprotection (Preclinical)
In multiple animal models, MB has demonstrated: rescue of dopaminergic neurons from rotenone toxicity (Parkinson's model) [3]; attenuation of cerebral ischemia-reperfusion injury (stroke model) [3]; reversal of cognitive deficits in aging mice [7]; and protection against traumatic brain injury sequelae. These findings await human translation.
Longevity
MB extended lifespan by approximately 30.8% in C. elegans (nematode worm) models. MB delayed cellular senescence, enhanced mitochondrial Complex IV activity by 30%, and increased cellular oxygen consumption by 37-70% in human cell culture [7]. No human longevity data exists.
Antimicrobial Activity
MB retains antimalarial activity against chloroquine-resistant Plasmodium falciparum through selective inhibition of parasite glutathione reductase [1]. It is under investigation as a component of combination antimalarial therapy.
Biomarker Evidence Matrix
Category
Focus & Mental Clarity
- Evidence Strength
- 6/10
- Reported Effectiveness
- 7/10
- Summary
- Single RCT in healthy volunteers showed 7% memory improvement on fMRI. Consistent community reports of improved focus and clarity.
Category
Energy Levels
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Mechanistic basis via mitochondrial ATP enhancement is strong. Human evidence limited to surrogate markers and anecdotal reports.
Category
Mood & Wellbeing
- Evidence Strength
- 7/10
- Reported Effectiveness
- 7/10
- Summary
- Multiple controlled human studies for depression (15-300 mg/day). MAO-A inhibition provides clear pharmacological basis. Community reports consistently positive.
Category
Memory & Cognition
- Evidence Strength
- 6/10
- Reported Effectiveness
- 6/10
- Summary
- One RCT (n=26) showed 7% improvement. Fear extinction study supports memory consolidation effects. Community reports positive but non-specific.
Category
Anxiety
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- Fear extinction study supports anxiolytic potential. Community reports mixed: calming at low doses, anxiety-inducing at high doses.
Category
Sleep Quality
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- No direct clinical evidence. Community reports mixed: improved deep sleep reported, but late dosing disrupts sleep onset.
Category
Longevity & Neuroprotection
- Evidence Strength
- 5/10
- Reported Effectiveness
- 5/10
- Summary
- Strong preclinical data (neuroprotection in multiple disease models, lifespan extension in worms). No human longevity data. Postoperative delirium RCT is closest human evidence.
Category
Motivation & Drive
- Evidence Strength
- 3/10
- Reported Effectiveness
- 6/10
- Summary
- No direct clinical evidence. MAO-A inhibition (dopamine increase) provides plausible mechanism. Community reports positive but thin.
Category
Inflammation
- Evidence Strength
- 4/10
- Reported Effectiveness
- 4/10
- Summary
- Antioxidant mechanism well-established. Anti-inflammatory effects demonstrated in preclinical models. Limited community reporting on inflammation specifically.
Category
Physical Performance
- Evidence Strength
- 3/10
- Reported Effectiveness
- 4/10
- Summary
- Minimal human evidence. Community reports mixed: some report improved endurance, others report impaired exercise capacity at higher doses.
Category
Side Effect Burden
- Evidence Strength
- 8/10
- Reported Effectiveness
- 4/10
- Summary
- Well-documented side effect profile from clinical use. Serotonin syndrome risk well-established. Community highly aware of safety concerns. Score reflects burden, not safety.
Category
Stress Tolerance
- Evidence Strength
- 3/10
- Reported Effectiveness
- 5/10
- Summary
- No direct clinical evidence. MAO inhibition provides plausible mechanism. Thin community reports of improved stress resilience.
Category
Skin Health
- Evidence Strength
- 2/10
- Reported Effectiveness
- 3/10
- Summary
- Minimal evidence. Some research on photoprotection; no clinical trials for skin outcomes.
Category
Treatment Adherence
- Evidence Strength
- —
- Reported Effectiveness
- 5/10
- Summary
- Oral administration is convenient but dosing precision matters. Blue urine and taste are adherence challenges. Cycling required.
Categories scored: 14
Categories with community data: 14
Categories not scored (insufficient data): Fat Loss, Muscle Growth, Weight Management, Appetite & Satiety, Food Noise, Libido, Sexual Function, Joint Health, Pain Management, Recovery & Healing, Gut Health, Digestive Comfort, Nausea & GI Tolerance, Hair Health, Heart Health, Blood Pressure, Heart Rate & Palpitations, Hormonal Symptoms, Temperature Regulation, Fluid Retention, Body Image, Immune Function, Bone Health, Cravings & Impulse Control, Social Connection, Emotional Aliveness, Emotional Regulation, Withdrawal Symptoms, Daily Functioning
Benefits & Potential Effects
The Basics
The potential benefits of Methylene Blue cluster around three main areas: brain function, cellular energy, and mood. Most people who explore this compound are interested in one or more of these.
For brain function, the most consistently reported benefit is improved mental clarity and focus. Users describe a sharpened ability to concentrate on demanding tasks, better information retention, and what some call "cleaner" cognitive energy compared to stimulants like caffeine. These effects make sense given how MB works: by improving the energy supply to neurons, it allows the brain to operate more efficiently without the jittery overstimulation that comes from simply pushing neurons harder.
For cellular energy, the mitochondrial mechanism suggests that MB could improve energy output in any cell with mitochondria, which means essentially every cell in the body. In practice, people most commonly notice this as sustained daytime energy without the crash pattern associated with stimulants. Athletes and fitness enthusiasts report mixed experiences, with some noting improved endurance and others finding exercise actually feels harder (likely dose-dependent).
For mood, Methylene Blue's MAO inhibitor activity means it genuinely increases levels of serotonin, dopamine, and norepinephrine. This is not speculative; it is the same pharmacological mechanism used by prescription antidepressants in the MAO inhibitor class. Clinical trials have demonstrated antidepressant effects at doses ranging from 15 to 300 mg per day, and community users frequently report improved mood stability, motivation, and emotional resilience.
It is worth emphasizing what the evidence does not support: Methylene Blue is not a proven treatment for Alzheimer's disease (Phase III trials failed), it has not been shown to extend human lifespan, and its cognitive benefits in healthy people are based on a single small study. The compound shows genuine promise in several areas, but the gap between mechanistic potential and proven human benefit remains significant for most applications outside its approved indication.
The Science
Cognitive Enhancement: MB's cognitive effects are mediated by enhanced cerebral metabolic rate (CMRO2) through mitochondrial Complex IV augmentation, increased cerebral blood flow, and modulation of cholinergic signaling via acetylcholinesterase inhibition [9][15]. The fMRI study demonstrated that MB increased BOLD signal coupling between prefrontal and posterior cortical regions during encoding, suggesting enhanced network integration rather than simple stimulation [15].
Neuroprotection: The dual antioxidant-mitochondrial mechanism provides neuroprotection through multiple pathways: reduced mitochondrial ROS generation, maintained ATP synthesis under stress conditions, enhanced cellular resistance to apoptotic signals, and reversal of premature senescence markers [3][4][7]. These effects have been demonstrated in models of Parkinson's (rotenone, 6-OHDA), Alzheimer's (tau aggregation, amyloid toxicity), stroke (ischemia-reperfusion), and traumatic brain injury.
Antidepressant and Anxiolytic: Reversible MAO-A inhibition increases monoamine neurotransmitter availability [6]. Additionally, the cGMP pathway inhibition and NO modulation may contribute to mood effects independently of monoamine mechanisms [8]. The fear extinction finding [16] suggests MB may enhance the consolidation of safety learning, a mechanism relevant to anxiety disorder treatment.
Anti-aging: MB delayed replicative senescence and extended cellular lifespan in human fibroblast cultures, associated with enhanced Complex IV activity and heme synthesis [7]. These in vitro findings correlate with the C. elegans lifespan extension data but have not been replicated in mammalian lifespan studies.
The benefits outlined above span multiple body systems, and your experience will be uniquely yours. Rather than guessing which effects are attributable to this compound versus other factors in your life, Doserly helps you log specific outcomes alongside your protocol details, building a clear picture of what's changing and when.
Over weeks and months, this creates something more useful than any anecdotal report: your own evidence-based record of how this compound affects you personally, at your specific dose, within the context of your full health protocol. When it's time to decide whether to continue, adjust, or discontinue, you have real data to inform that conversation with your healthcare provider.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
Side Effects & Safety Considerations
The Basics
Methylene Blue's side effect profile requires careful attention because it includes one potentially life-threatening interaction and several dose-dependent effects that distinguish it from most supplements.
The most critical safety concern is serotonin syndrome. If you are taking any medication that increases serotonin levels (including SSRIs like Prozac, Zoloft, or Lexapro; SNRIs like Effexor or Cymbalta; MAO inhibitors; tramadol; St. John's wort; or several others), combining it with Methylene Blue can trigger a dangerous condition called serotonin syndrome. Symptoms include high fever, seizures, muscle rigidity, and it can be fatal. This is not a theoretical risk; the FDA has issued multiple warnings about this interaction. If you take any psychiatric medication, do not use Methylene Blue without explicit guidance from your prescribing physician.
The second critical concern is G6PD deficiency, a genetic enzyme deficiency affecting approximately 400 million people worldwide, with higher prevalence in populations of African, Mediterranean, Middle Eastern, and Southeast Asian descent. In G6PD-deficient individuals, Methylene Blue can cause severe hemolytic anemia (destruction of red blood cells) instead of its intended therapeutic effect. Testing for G6PD deficiency before using MB is strongly recommended.
Common and generally mild side effects include: blue or green discoloration of urine (universal at any meaningful dose, completely harmless), temporary blue staining of the tongue and teeth (sublingual dosing), mild nausea, headache, dizziness, and a metallic or unpleasant taste. These typically resolve with dose reduction or tend to diminish over time.
At higher doses (above 2-4 mg/kg), the compound's hormetic flip occurs: the antioxidant becomes a pro-oxidant. Signs of excessive dosing include anxiety, restlessness, overstimulation, sleep disruption, and chest discomfort. Above 7 mg/kg, there is risk of paradoxical methemoglobinemia (the very condition it is designed to treat at lower doses).
An additional safety consideration that receives less attention is contamination risk. Multiple independent analyses have found that a majority of commercially available Methylene Blue products contain detectable levels of heavy metals including arsenic, lead, cadmium, and mercury. Only pharmaceutical-grade (USP) Methylene Blue with a Certificate of Analysis should be used for any human application.
The Science
Serotonin Syndrome: MB's inhibition of MAO-A (Ki ~27 nM) becomes clinically significant at doses above 1-2 mg/kg [6]. When combined with serotonin reuptake inhibitors, the dual blockade of serotonin degradation (MAO-A) and reuptake creates conditions for serotonergic crisis. The FDA contraindication applies to: SSRIs, SNRIs, MAOIs, tricyclic antidepressants, buspirone, tramadol, linezolid, dextromethorphan, St. John's wort, tryptophan, and 5-HTP. A minimum washout period of 5 half-lives of the serotonergic agent is generally recommended before initiating MB.
G6PD Deficiency: MB's mechanism for treating methemoglobinemia requires NADPH generated by the hexose monophosphate shunt, which depends on glucose-6-phosphate dehydrogenase. G6PD-deficient patients cannot generate adequate NADPH, and MB administration causes oxidative hemolysis rather than methemoglobin reduction. Prevalence: 4.9% globally, up to 20-30% in certain populations [21].
Hormetic Pro-oxidant Transition: At concentrations above approximately 2 micromolar (corresponding to oral doses >2-4 mg/kg), MB transitions from electron donor to electron acceptor in the mitochondrial ETC, generating superoxide and disrupting the proton gradient [5]. This dose-dependent reversal is consistent across all available pharmacological data.
Genotoxicity and Carcinogenicity: National Toxicology Program (NTP) bioassays found clear evidence of carcinogenicity in male rats (thyroid follicular cell tumors) and equivocal evidence in female rats and mice. Multiple in vitro genotoxicity assays have returned positive results. The clinical relevance of these findings to low-dose intermittent human use is uncertain but warrants consideration for long-term protocols.
Contamination: Analysis of commercially available MB products has found that approximately 60% contain detectable heavy metal contamination. Industrial and aquarium-grade MB may contain 8-11% impurities by mass. Only USP pharmaceutical grade is appropriate for human use.
Pregnancy and Lactation: Pregnancy Category X. Associated with intestinal atresia, hemolytic anemia, hyperbilirubinemia, and methemoglobinemia in neonates. Breastfeeding should be interrupted for a minimum of 8 days following MB exposure.
Side effect profiles are most useful when you can compare them against your own experience in real time. Doserly lets you log symptoms, severity, and timing alongside your dosing data, creating a side-by-side view of your protocol and your body's response.
This kind of systematic tracking catches things that memory alone misses. A subtle mood shift that began three days after a dose increase. Sleep disruption that correlates with evening administration. These patterns become visible when the data is laid out on a timeline, and they give your healthcare provider actionable information rather than vague concerns. Early detection of emerging side effects means earlier intervention.
Keep side effects, flags, and follow-up notes visible.
Doserly helps you document safety observations, side effects, medication changes, and follow-up questions so important context is not scattered.
Safety log
Flags and notes

Safety notes are not emergency guidance; seek medical help when appropriate.
Dosing Protocols
The Basics
Dosing Methylene Blue requires more precision than most supplements because of the inverted U-shaped response curve: too little does nothing, the right amount provides benefit, and too much causes harm. The difference between these zones varies by individual, but the general principle is consistent across all sources.
The accepted therapeutic range for oral use is 0.5 to 4 mg/kg of body weight per day. For a person weighing 70 kg (154 lbs), that translates to roughly 35 to 280 mg. However, most practitioners and experienced users work within a narrower band. For general mitochondrial support and cognitive enhancement, 0.5 to 1.5 mg/kg per day (approximately 35 to 105 mg for a 70 kg person) is the most commonly cited range for sustained daily use.
Many protocols use even lower doses for maintenance. The range of 5 to 25 mg per day is frequently discussed in biohacking communities for daily cognitive support, while higher doses of 15 to 50 mg are more commonly used as-needed before cognitively demanding tasks.
Formulation matters enormously. Because oral bioavailability varies from about 6.5% for capsules to 72% for liquid solutions, 10 mg of a liquid preparation may deliver more active compound than 50 mg from a capsule. This difference is not widely appreciated and is a common source of confusion when comparing dosing reports across users.
Cycling is generally recommended rather than continuous daily use. Common patterns include 5 days on and 2 days off, or 4 weeks on followed by 1 to 2 weeks off. The rationale is to prevent the body from adapting to the altered electron transport and to maintain the hormetic benefit zone. Continuous use at doses above 1 mg/kg may gradually shift the redox balance toward oxidative stress.
Timing is straightforward: take Methylene Blue in the morning or early afternoon, at least 6 hours before bedtime. The stimulating effects on mitochondrial energy production can interfere with sleep onset when taken in the evening. Many users take it 30 to 60 minutes before demanding cognitive work.
The Science
FDA-approved (Methemoglobinemia): 1 mg/kg IV over 5-30 minutes; may repeat once after 1 hour if MetHb >30%. Maximum 2 doses. Cumulative toxicity risk above 7 mg/kg.
Vasoplegic Syndrome (off-label): 2 mg/kg IV bolus, or 2-4 mg/kg bolus followed by 0.25 mg/kg/hour infusion for 4-72 hours. A 2025 comparative study found that 4 mg/kg with continuous infusion reduced mortality risk versus 1 mg/kg alone (HR 0.29, 95% CI 0.09-0.90).
Postoperative Delirium Prevention (off-label): 2 mg/kg IV single dose within 1 hour after anesthesia.
Cognitive Enhancement (research): 280 mg single dose (approximately 4 mg/kg) showed fMRI-measured memory improvement [15]. Not a daily dosing paradigm.
Oral Wellness Protocols (community-reported, not clinically validated):
Protocol
Mitochondrial maintenance
- Daily Dose
- 5-20 mg/day oral
- Cycling
- 5 on / 2 off
- Notes
- Conservative long-term approach
Protocol
Cognitive enhancement
- Daily Dose
- 15-50 mg oral
- Cycling
- As needed
- Notes
- Pre-event or pre-work session
Protocol
Mood support
- Daily Dose
- 15-40 mg/day oral
- Cycling
- Continuous or cycling
- Notes
- Pharmacological MAO-A effect
Protocol
Research wellness protocol
- Daily Dose
- 0.5-1 mg/kg/day
- Cycling
- 4 weeks on / 2 off
- Notes
- Start low, titrate over 1 week
What to Expect
Week 1: Orientation Phase
Most users who respond to Methylene Blue notice effects within the first few days. Common early observations include a subtle increase in mental clarity, more sustained daytime energy, and the signature blue or green urine. Some users experience mild nausea, headache, or an unpleasant taste during the first few days, particularly if starting at higher doses. These initial side effects typically resolve quickly. If starting with the commonly discussed low-dose approach (5-10 mg), effects may be subtle or unnoticed initially.
Weeks 2-4: Stabilization
By the second week, users who respond positively typically report more consistent cognitive benefits: improved focus during work sessions, better task completion, and a general sense of "cleaner" mental energy. Mood improvements may become more noticeable as the MAO inhibition effect builds. Energy levels tend to stabilize. Blue urine becomes routine and no longer alarming. Users on cycling protocols (5 on / 2 off) may notice a mild dip on off days initially, though this often levels out.
Weeks 4-8: Assessment Period
By this point, the full effect profile should be apparent. Users who experience benefits typically describe them as steady and reliable rather than dramatic. Those who are going to respond to MB usually know by week 4; if no noticeable effects have emerged, the compound may not be meaningful for that individual's biology. This is a natural decision point: continue, adjust dose, or discontinue. For those on 4-week cycling protocols, the washout period provides a useful comparison point.
Beyond 8 Weeks: Maintenance or Discontinuation
Long-term users typically settle into a consistent maintenance dose and cycling pattern. Some reduce their dose over time as they find the minimum effective amount. Others use MB intermittently, dosing before demanding cognitive periods rather than daily. No published data exists on effects beyond 12 weeks of continuous use in healthy volunteers, so long-term protocols are guided by individual response and practitioner input.
Interaction Compatibility
Synergistic Compounds
- NAD+ — Synergistic mitochondrial support. MB enhances electron transport; NAD+ fuels the redox reactions that drive it. Commonly stacked in longevity protocols.
- MOTS-C — Complementary mechanisms. MOTS-C optimizes healthy mitochondrial function; MB rescues dysfunctional mitochondria. Together they cover both optimization and repair.
- SS-31 — Targets inner mitochondrial membrane; complements MB's ETC bypass mechanism. Both address mitochondrial dysfunction through different pathways.
- Semax — Cognitive enhancement via neurotrophic pathways (BDNF). Complements MB's metabolic approach to cognition. Different mechanisms, potentially additive benefits.
- Selank — Anxiolytic peptide that may counterbalance any anxiety-promoting effects of MB at higher doses. No known interaction concerns.
- CoQ10 / Ubiquinol — Both are mitochondrial electron carriers. Community reports are mixed: some sources suggest CoQ10 may reduce MB effectiveness by competing for electron transport positions, while others recommend the combination. Caution and monitoring advised.
- Red light therapy (photobiomodulation, 600-700 nm) — MB absorbs red light wavelengths, potentially creating synergistic photochemical activation in tissues. This combination is discussed in biohacking communities, though clinical evidence is limited.
Compounds to Avoid
- SSRIs (fluoxetine, sertraline, citalopram, escitalopram, paroxetine, fluvoxamine) — Serotonin syndrome risk. Absolute contraindication.
- SNRIs (venlafaxine, duloxetine, milnacipran) — Serotonin syndrome risk. Absolute contraindication.
- MAO Inhibitors (phenelzine, tranylcypromine, isocarboxazid, selegiline, rasagiline) — Additive MAO inhibition. Absolute contraindication.
- Tramadol, tapentadol — Serotonergic and seizure risk.
- Linezolid — Antibiotic with MAO inhibitor activity.
- Dextromethorphan — Found in many cough medicines. Serotonergic interaction.
- St. John's wort — Herbal MAO inhibitor. Additive serotonin risk.
- Tryptophan, 5-HTP — Serotonin precursors. Additive serotonin risk.
- Buspirone — Serotonergic anxiolytic.
- PDE-5 inhibitors (sildenafil, tadalafil) — MB inhibits NO/cGMP; may reduce effectiveness of PDE-5 inhibitors and cause blood pressure changes.
Administration Guide
Methylene Blue is administered orally in wellness contexts. The most common preparations are liquid solutions (typically 1% concentration, meaning 10 mg per mL) and capsules. Sublingual drops are also available and may offer faster onset.
Materials typically needed:
- Pharmaceutical-grade (USP) Methylene Blue with Certificate of Analysis
- Calibrated dropper or oral syringe for liquid preparations
- Glass of water (to follow the dose and reduce oral staining)
- Optional: straw (to minimize tooth staining with liquid)
Timing considerations:
Morning or early afternoon dosing is recommended, ideally 30-60 minutes before periods of cognitive demand. Most practitioners recommend taking MB at least 6 hours before intended sleep time. MB can be taken on an empty stomach or with food; food may reduce mild nausea but is not required for absorption.
Post-administration observations:
Blue or green urine is expected and harmless, typically appearing within 1-2 hours of dosing and persisting for several hours. Temporary blue discoloration of the tongue and teeth occurs with liquid or sublingual preparations and resolves within hours. Subtle increases in alertness or focus are commonly reported within 30-60 minutes of oral dosing.
When to be concerned:
Seek immediate medical attention for: signs of serotonin syndrome (fever, muscle rigidity, rapid heart rate, confusion), dark or bloody urine (may indicate hemolysis), severe shortness of breath, or chest pain. Discontinue use and consult a healthcare provider for persistent headaches, significant anxiety or restlessness, or blood pressure changes.
Supplies & Planning
Methylene Blue preparations:
- Liquid solution (1% = 10 mg/mL): most common for precise dosing. Available in various bottle sizes (15 mL, 30 mL, 50 mL).
- Capsules: available in various strengths (1 mg, 5 mg, 10 mg, 20 mg). Lower bioavailability than liquid.
- Sublingual drops: fast onset, some users prefer for cognitive use.
Dosing tools:
- Calibrated dropper (typically included with liquid products)
- Oral syringe (1 mL or 3 mL) for precise measurement
- Optional: disposable gloves (MB stains skin temporarily)
Storage supplies:
- Dark glass bottle (if transferring from original container)
- Refrigeration for opened liquid preparations
Quality verification:
- Certificate of Analysis (CoA) from the manufacturer
- USP pharmaceutical grade only (not lab grade, not aquarium grade)
- Third-party testing verification for heavy metals
Specific quantities depend on individual dosing protocols determined in consultation with a healthcare provider. Readers requiring help with preparation calculations can use the reconstitution calculator.
Storage & Handling
Powder and tablet forms:
- Store at room temperature (15-25°C / 59-77°F)
- Keep in a tightly sealed container
- Protect from light (amber or dark glass preferred)
- Keep dry; avoid humidity
- Shelf life: typically 2-3 years when stored properly
Liquid solution (opened):
- Refrigerate at 2-8°C (36-46°F) after opening
- Protect from light
- Use within manufacturer's specified timeframe (typically 3-6 months after opening)
- Ensure cap is tightly sealed to prevent evaporation and contamination
Handling precautions:
- Methylene Blue stains skin, clothing, countertops, and other surfaces. Staining is temporary on skin (resolves in 12-24 hours) but may be permanent on fabrics and porous surfaces.
- Use disposable gloves when handling liquid preparations if staining is a concern.
- Clean spills immediately with soap and water or dilute bleach solution.
- Keep away from children (blue color may be attractive; doses safe for adults can be harmful to children).
Lifestyle Factors
Nutrition:
Adequate NAD+ levels support MB's mitochondrial mechanism. Foods rich in niacin (vitamin B3), tryptophan, and nicotinamide may complement MB use. Some practitioners recommend concurrent supplementation with B vitamins, particularly B2 (riboflavin, a cofactor for flavin-dependent enzymes in the ETC) and B3. Adequate hydration is important, particularly given MB's renal excretion.
Exercise:
The relationship between MB and exercise is nuanced. In individuals with suboptimal mitochondrial function, MB may improve exercise tolerance by enhancing ATP production. However, in individuals with healthy mitochondria, MB may paradoxically impair exercise performance by redirecting electron flow away from the normal, optimized ETC pathways. Community reports reflect this duality, with some users reporting improved endurance and others reporting that exercise feels harder. Starting with lower doses and monitoring exercise performance is advisable.
Sleep:
MB should be taken at least 6 hours before bedtime to avoid sleep disruption. The compound's stimulatory effect on mitochondrial energy production and its influence on monoamine neurotransmitters can delay sleep onset when taken later in the day. Some users report improved sleep quality when MB is taken early in the morning, possibly due to improved daytime energy utilization leading to better circadian entrainment.
Red Light Therapy:
Methylene Blue absorbs light in the 600-700 nm range (red light), and some practitioners combine MB with red light therapy (photobiomodulation) for synergistic mitochondrial effects. MB increases the photon absorption capacity of cytochrome c oxidase, the terminal enzyme in the ETC and the primary chromophore for red/near-infrared light therapy. This combination is discussed in biohacking circles, though controlled human studies on the combination are lacking.
Monitoring:
Tracking the following metrics can help assess MB's effects and detect issues early: cognitive performance (focus duration, task completion), energy levels throughout the day, mood and emotional baseline, sleep quality and onset time, blood pressure (MB can increase BP via NO inhibition), urine color (expected), and any new symptoms. For multi-week protocols, periodic blood work including CBC, liver function tests (LFTs), and renal function is recommended by some practitioners.
The lifestyle factors above, nutrition, exercise, sleep, stress management, are not just nice-to-haves alongside a peptide protocol. They're force multipliers. Doserly lets you track these inputs alongside your compounds, building a complete picture of what your body is receiving and how it's responding.
When everything lives in one dashboard, patterns emerge. You can see whether training days correlate with better biomarker trends, whether your sleep scores predict next-day recovery quality, or whether stress spikes derail your progress in measurable ways. This kind of integrated tracking turns the lifestyle recommendations in this section from abstract advice into actionable, personalized insight.
See how each compound fits into the whole protocol.
Doserly organizes compounds, supplements, peptides, medications, and hormone protocols together so overlapping routines are easier to understand.
Stack view
Connected protocol
Stack views improve organization; they do not determine compatibility.
Regulatory Status & Research Classification
United States (FDA):
- Approved for methemoglobinemia (as ProvayBlue, 0.5% injection). NDA approved.
- Off-label use for vasoplegic syndrome and ifosfamide-induced encephalopathy is established in clinical practice.
- No approval for cognitive enhancement, antidepressant, or mitochondrial support indications.
- Available as a prescription medication. Not classified as a dietary supplement.
- ClinicalTrials.gov lists active studies including trials for Alzheimer's disease (LMTM/TRx0237), antimalarial applications, and vasoplegic syndrome.
Canada (Health Canada):
- Available as a prescription drug for methemoglobinemia.
- Not approved for cognitive or wellness applications.
United Kingdom (MHRA):
- Licensed as Proveblue (methylthioninium chloride) for methemoglobinemia.
- Prescription-only medicine. Not available as a supplement.
Australia (TGA):
- Registered for methemoglobinemia treatment.
- Schedule 4 (prescription only).
- Not approved for wellness or cognitive enhancement.
European Union (EMA):
- Centrally authorized as Methylthioninium chloride Proveblue for methemoglobinemia in adults and children.
- Prescription-only across member states.
WADA Status:
- Methylene Blue is not currently listed on the WADA Prohibited List. However, athletes should verify current status before use, as classifications can change.
Active Clinical Trials:
- Alzheimer's disease: LMTM (leucomethylthioninium mesylate) trials ongoing following mixed Phase III results
- Antimalarial combinations: MB-based combination therapies under investigation in Sub-Saharan Africa
- Vasoplegic syndrome: Dosing optimization trials
- Postoperative delirium: Follow-up studies to the 248-patient RCT
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is Methylene Blue and why are people using it?
Methylene Blue is a 149-year-old synthetic compound, originally created as a textile dye, that has found medical applications ranging from treating methemoglobinemia to experimental use in cognitive enhancement. It is gaining attention in the biohacking and longevity communities primarily for its ability to enhance mitochondrial energy production at low doses. It is FDA-approved for one specific medical condition but not for the cognitive or wellness uses most people are interested in.
What dose is commonly discussed for cognitive or wellness use?
Based on available sources, commonly reported oral ranges for wellness purposes fall between 5 and 50 mg per day, with most daily users settling around 10 to 30 mg. The broader therapeutic range cited in clinical literature is 0.5 to 4 mg/kg per day, but wellness protocols generally stay at the lower end. Formulation type (liquid solution vs. capsule) significantly affects how much active compound is absorbed. A healthcare professional should be consulted to determine what is appropriate for any individual.
Can Methylene Blue be taken with antidepressants?
This is a critical safety question. Methylene Blue should not be combined with SSRIs, SNRIs, MAO inhibitors, or other serotonergic medications due to the risk of serotonin syndrome, a potentially fatal condition. The FDA has issued specific warnings about this interaction. If you are taking any psychiatric medication, consult your prescribing physician before considering Methylene Blue.
What is the inverted U-shaped dose response?
This describes how Methylene Blue's effects reverse at higher doses. At low doses (nanomolar to low micromolar concentrations), MB acts as an antioxidant and mitochondrial enhancer. At higher doses (above approximately 2-4 mg/kg), it transitions to a pro-oxidant that generates the very reactive oxygen species it suppresses at lower doses. This means that more is not better, and exceeding the hormetic window can produce the opposite of the desired effect.
Why does Methylene Blue turn urine blue?
The blue or green discoloration of urine is a normal, harmless consequence of MB being excreted by the kidneys. Approximately 75% of an oral dose is eliminated through urine, primarily as the colorless reduced form (leucomethylene blue), but enough oxidized (blue) form remains to produce visible coloration. The effect is temporary and resolves as the compound clears the body.
Should I get tested for G6PD deficiency before using Methylene Blue?
Based on available data, G6PD testing is strongly recommended before any use of Methylene Blue. G6PD deficiency is a genetic condition affecting approximately 400 million people worldwide, with higher prevalence in certain populations. In G6PD-deficient individuals, MB can cause severe hemolytic anemia. A simple blood test can determine G6PD status.
How does the formulation affect dosing?
The bioavailability of oral Methylene Blue varies dramatically by formulation. Liquid aqueous solutions have approximately 72% bioavailability, while capsules may deliver as little as 6.5%. This means 10 mg from a liquid could deliver similar amounts to the bloodstream as 100 mg from a capsule. When comparing dosing reports from different users, the formulation context is essential.
Is Methylene Blue a peptide?
No. Methylene Blue is a small synthetic molecule (phenothiazine class, 319.85 g/mol), not a peptide. It is included in the Doserly compound database because it is frequently discussed alongside peptides in mitochondrial support, cognitive enhancement, and longevity protocols, and is often stacked with peptides like MOTS-C, SS-31, and NAD+.
Sources & References
Clinical Trials and Human Studies
- Schirmer RH, Coulibaly B, Stich A, et al. "Methylene blue as an antimalarial agent." Redox Report. 2003;8(5):272-275. PubMed
- Wainwright M, Crossley KB. "Methylene Blue: a therapeutic dye for all seasons?" Journal of Chemotherapy. 2002;14(5):431-443. PubMed
- Wen Y, Li W, Poteet EC, et al. "Alternative mitochondrial electron transfer as a novel strategy for neuroprotection." Journal of Biological Chemistry. 2011;286(18):16504-16515. PubMed
- Poteet E, et al. "Neuroprotective Actions of Methylene Blue and Its Derivatives." PLOS One. 2012;7(10):e48279. PubMed
- Rojas JC, Bruchey AK, Gonzalez-Lima F. "Neurometabolic mechanisms for memory enhancement and neuroprotection of methylene blue." Progress in Neurobiology. 2012;96(1):32-45. PubMed
- Ramsay RR, Dunford C, Gillman PK. "Methylene blue and serotonin toxicity: inhibition of monoamine oxidase A (MAO A) confirms a theoretical prediction." British Journal of Pharmacology. 2007;152(6):946-951. PubMed
- Atamna H, Nguyen A, Schultz C, et al. "Methylene blue delays cellular senescence and enhances key mitochondrial biochemical pathways." FASEB Journal. 2008;22(3):703-712. PubMed
- Bužga M, Machytka E, Dvořáčková E, et al. "Methylene blue: a controversial diagnostic acid and medication?" Toxicology Research. 2022;11(5):711-717. PMC
- Pfaffendorf M, Bruning TA, Batnik HD, van Zwieten PA. "The interaction between methylene blue and the cholinergic system." British Journal of Pharmacology. 1997;122(1):95-98. PubMed
- Crowe A, James MJ, Lee VM, et al. "Aminothienopyridazines and methylene blue affect Tau fibrillization via cysteine oxidation." Journal of Biological Chemistry. 2013;288(16):11024-11037. PubMed
- Walter-Sack I, Rengelshausen J, Oberwittler H, et al. "High absolute bioavailability of methylene blue given as an aqueous oral formulation." European Journal of Clinical Pharmacology. 2009;65(2):179-189. PubMed
- Peter C, Hongwan D, Küpfer A, Lauterburg BH. "Pharmacokinetics and organ distribution of intravenous and oral methylene blue." European Journal of Clinical Pharmacology. 2000;56(3):247-250. PubMed
- DiSanto AR, Wagner JG. "Pharmacokinetics of highly ionized drugs II: methylene blue. Absorption, metabolism, and excretion studies." Journal of Pharmaceutical Sciences. 1972;61(7):1086-1090. PubMed
- Postoperative delirium prevention RCT (248 elderly patients, 2 mg/kg IV). Referenced in multiple clinical reviews. ClinicalTrials.gov registration available.
- Rodriguez P, Zhou W, Barrett DW, et al. "Multimodal Randomized Functional MR Imaging of the Effects of Methylene Blue in the Human Brain." Radiology. 2016;281(2):516-526. PubMed
- Telch MJ, Bruchey AK, Rosenfield D, et al. "Effects of Post-Session Administration of Methylene Blue on Fear Extinction and Contextual Memory in Adults With Claustrophobia." American Journal of Psychiatry. 2014;171(10):1091-1098. PubMed
- Naylor GJ, Smith AH, Connelly P. "A controlled trial of methylene blue in severe depressive illness." Biological Psychiatry. 1987;22(5):657-659. PubMed
- Naylor GJ, Martin B, Hopwood SE, Watson Y. "A two-year double-blind crossover trial of the prophylactic effect of methylene blue in manic-depressive psychosis." Biological Psychiatry. 1986;21(10):915-920. PubMed
- Alda M, McKinnon M, Blagdon R, et al. "Methylene blue treatment for residual symptoms of bipolar disorder: randomised crossover study." British Journal of Psychiatry. 2017;210(1):54-60. PubMed
- TauRx Therapeutics. LMTM (leucomethylthioninium mesylate) Phase III trials for Alzheimer's disease. ClinicalTrials.gov: NCT01689246, NCT01689233.
- Cappellini MD, Fiorelli G. "Glucose-6-phosphate dehydrogenase deficiency." The Lancet. 2008;371(9606):64-74. PubMed
Reviews and Meta-analyses
- Oz M, Lorke DE, Petroianu GA. "Methylene blue and Alzheimer's disease." Biochemical Pharmacology. 2009;78(8):927-932. PubMed
Related Peptide Guides
- NAD+ — Mitochondrial coenzyme; synergistic with MB for cellular energy support
- MOTS-C — Mitochondrial-derived peptide; complementary mechanism (optimizes healthy mitochondria vs. MB's rescue of dysfunctional mitochondria)
- SS-31 — Mitochondrial-targeted peptide; targets inner mitochondrial membrane
- Semax — Nootropic peptide; complementary cognitive enhancement via neurotrophic pathways
- Selank — Anxiolytic peptide; may complement MB for cognitive protocols
- 5-Amino-1MQ — Metabolic optimization compound; discussed alongside MB in energy stacks
- SLU-PP-332 — Exercise mimetic; paired with MB in some mitochondrial protocols
- BAM15 — Mitochondrial uncoupler; different mechanism of mitochondrial modulation
- Dihexa — Cognitive peptide; sometimes combined with MB in nootropic stacks
- Tesofensine — Included in blends with MB (see Dihexa / Methylene Blue / Tesofensine)
- Epithalon — Longevity peptide; discussed alongside MB in anti-aging protocols