Tesofensine: Complete Research Guide
On this page
Quick Reference Card
Attribute
Also Known As
- Detail
- Tesofensine, NS-2330, NS2330, CL-201, GW327830, Tesofensin
Attribute
Administration
- Detail
- Oral (capsule/tablet)
Attribute
Research Status
- Detail
- Research Compound — Not FDA Approved. Phase 2 trials completed for obesity. Phase 3 never completed due to sponsor financial difficulties.
Attribute
Typical Dose Range
- Detail
- 0.25-1.0 mg once daily; 0.5 mg most commonly studied and referenced
Attribute
Half-Life
- Detail
- Approximately 9 days (216 hours); active metabolite half-life approximately 16 days
Attribute
Cycle Length
- Detail
- 12-24 weeks on, 4-6+ weeks off (community protocols); clinical trials used 24-week treatment periods
Attribute
Storage
- Detail
- Room temperature (20-25C / 68-77F), protected from moisture and light. No refrigeration required.
Overview / What Is Tesofensine?
The Basics
Tesofensine is a small-molecule compound, not a peptide, that produces weight loss by acting directly on brain chemistry. It blocks the recycling of three key neurotransmitters: dopamine, norepinephrine, and serotonin. By keeping these chemicals active longer in the brain, tesofensine suppresses appetite, increases energy expenditure, and reduces the mental preoccupation with food that many people experience during dieting.
Originally developed in Denmark for Parkinson's disease and Alzheimer's disease, researchers discovered something unexpected during early neurological trials: patients were losing significant amounts of weight without any dietary intervention. This accidental finding redirected the compound's development toward obesity treatment, where it produced some of the most striking weight loss data seen for an oral medication at the time.
In Phase 2 clinical trials, participants taking the 0.5 mg dose lost an average of 9.2% of their body weight over 24 weeks, roughly double what existing prescription weight loss drugs achieved at the time. The weight loss was predominantly fat mass, with lean body mass relatively preserved.
Despite these results, tesofensine has never reached the market. The Danish company that developed it ran into financial difficulties before completing Phase 3 trials, and concerns about modest increases in heart rate complicated the regulatory picture. It remains an unapproved investigational compound available only through research compound vendors and some compounding pharmacies.
The Science
Tesofensine (NS 2330) is a synthetic phenyltropane-class small molecule with a molecular formula of C17H23Cl2NO and molecular weight of 328.28 Da [1]. It functions as a triple monoamine reuptake inhibitor (TRI), blocking the presynaptic reuptake of dopamine (DAT IC50 = 6.5 nM), norepinephrine (NET IC50 = 1.7 nM), and serotonin (SERT IC50 = 11 nM), with highest potency at the norepinephrine transporter [2][3].
The compound was developed by NeuroSearch A/S (Copenhagen, Denmark) as a candidate treatment for neurodegenerative disorders. Phase I/II trials in Parkinson's disease revealed dose-dependent weight loss as a consistent secondary observation [4][5], prompting redirection to an obesity indication. The landmark Phase 2b trial (TIPO-1) enrolled 203 obese adults (BMI 30-40 kg/m2) and demonstrated 4.5%, 9.2%, and 10.6% mean weight loss at 0.25 mg, 0.5 mg, and 1.0 mg doses respectively over 24 weeks, significantly exceeding the 2.0% achieved with diet and placebo (p<0.0001 for 0.5 mg and 1.0 mg) [1].
It is important to distinguish tesofensine from peptide compounds. Tesofensine is a small synthetic molecule with no amino acid sequence. It is pharmacologically closer to antidepressants such as bupropion than to any peptide-based therapeutic. It appears in the peptide research ecosystem because the same vendors that supply research peptides also carry small-molecule compounds [6].
Molecular Identity
Attribute
Common Names
- Detail
- Tesofensine, NS-2330, NS2330, CL-201, GW327830, Tesofensin, Tesufensin
Attribute
IUPAC Name
- Detail
- (1R,2R,3S,5S)-3-(3,4-dichlorophenyl)-2-(ethoxymethyl)-8-methyl-8-azabicyclo[3.2.1]octane
Attribute
Molecular Formula
- Detail
- C17H23Cl2NO
Attribute
Molecular Weight
- Detail
- 328.28 Da (free base); ~520.40 Da (citrate salt)
Attribute
CAS Number
- Detail
- 195875-84-4 (free base); 861205-83-6 (citrate salt)
Attribute
PubChem CID
- Detail
- 11370864
Attribute
DrugBank ID
- Detail
- DB06156
Attribute
ChEMBL ID
- Detail
- CHEMBL514514
Attribute
FDA UNII
- Detail
- BLH9UKX9V1
Attribute
Structural Class
- Detail
- Phenyltropane; bicyclic 8-azabicyclo[3.2.1]octane core with 3,4-dichlorophenyl substituent
Attribute
Salt Forms
- Detail
- Free base (research); Citrate salt (pharmaceutical formulation)
Attribute
Physical Form
- Detail
- White to off-white sticky solid or powder; hygroscopic
Attribute
Solubility
- Detail
- DMSO: 1 mg/mL; DMF: 2 mg/mL; PBS (pH 7.2): 0.14 mg/mL; Water: sparingly soluble
Mechanism of Action
The Basics
Your brain uses three chemical messengers to regulate appetite, energy, and mood: serotonin (which signals fullness), dopamine (which controls reward and cravings), and norepinephrine (which drives metabolic activity). Normally, after these chemicals do their job, your brain recycles them quickly. Tesofensine slows down that recycling process for all three at once.
The practical effect is straightforward: you feel full sooner, food loses some of its magnetic pull, and your body burns slightly more energy at rest. People who take it often describe a meaningful drop in "food noise," the constant background hum of thinking about meals, snacks, and cravings. This addresses both the physical sensation of hunger and the psychological drive to eat.
What makes tesofensine distinct from most other weight loss compounds is this triple action. Many other compounds only target one or two of these pathways. By hitting all three simultaneously, tesofensine addresses multiple dimensions of overeating: biological hunger, reward-driven cravings, and metabolic rate.
Recent research has also identified a more specific brain target. Tesofensine appears to quiet a group of neurons in the lateral hypothalamus (a brain region that promotes feeding behavior) that use GABA, an inhibitory neurotransmitter, to drive the urge to eat [7].
The Science
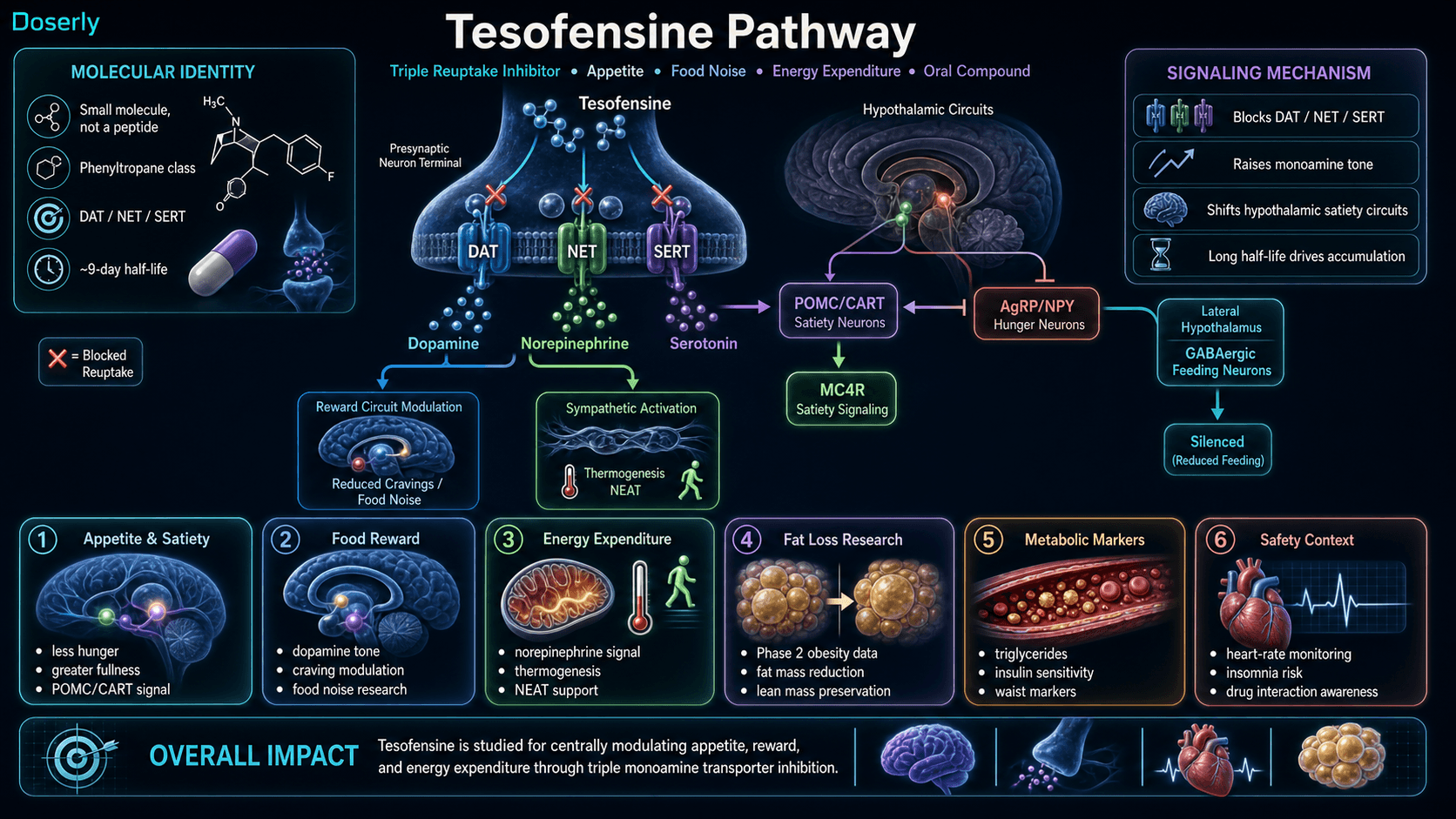
Tesofensine inhibits the presynaptic monoamine transporters DAT, NET, and SERT, increasing extracellular concentrations of dopamine, norepinephrine, and serotonin in the hypothalamic and mesolimbic regions responsible for appetite regulation and energy homeostasis [1][2].
PET imaging studies using carbon-11 labeled ligands have quantified dopamine transporter occupancy at clinically relevant doses: approximately 30-50% DAT occupancy at the 0.5 mg therapeutic dose, a range sufficient for appetite suppression but below the threshold typically associated with euphoric or reinforcing effects [8]. This occupancy profile differentiates tesofensine from classical psychostimulants and partially explains its lower abuse liability, as demonstrated in a formal abuse potential assessment comparing it to d-amphetamine [9].
The serotonergic component activates hypothalamic POMC/CART (anorexigenic) neurons while suppressing AgRP/NPY (orexigenic) neurons, enhancing downstream melanocortin-4 receptor (MC4R) satiety signaling [3]. The noradrenergic component increases sympathetic tone, promoting thermogenesis and non-exercise activity thermogenesis (NEAT).
A 2024 study by Perez et al. using optogenetic and chemogenetic techniques in rodent models demonstrated that tesofensine specifically silences GABAergic neurons in the lateral hypothalamus (LH), a brain region critical for feeding behavior and reward [7]. This mechanistic finding provides a more precise neuroanatomical target beyond generalized monoamine enhancement.
In diet-induced obese rat models, tesofensine demonstrates preferential efficacy in obese versus lean subjects, with a higher metabolic ratio in obese states. The compound reverses low forebrain dopamine levels characteristic of diet-induced obesity, potentially normalizing the dysregulated D2/D3 receptor availability associated with compulsive overeating [10][11].
Pathway Visualization Image
Pharmacokinetics
The Basics
Tesofensine has an unusually long half-life of about 9 days. This means that after you take a dose, the compound stays active in your body for over a week. In practical terms, this has several important consequences.
First, the effects build gradually. It takes approximately 5-6 weeks of daily dosing before the compound reaches its full steady-state concentration in your body. This is why many people do not feel the complete effect in the first week or two. Patience during this ramp-up period is important.
Second, side effects are equally persistent. If a side effect develops, it will not disappear quickly after stopping the compound. Tesofensine and its active metabolite can take over a month to fully clear from your system.
Third, dose adjustments require patience. Changing your dose level takes several weeks to fully manifest in terms of effects, which is why clinical trials allowed minimum 4-6 week windows when evaluating dose responses.
The compound is taken orally and reaches peak blood levels approximately 8 hours after a dose. It is metabolized primarily in the liver and produces an active metabolite that is even longer-lasting, with a half-life of about 16 days.
The Science
Tesofensine demonstrates distinctive pharmacokinetic properties driven by its long elimination half-life.
Parameter
Tmax (time to peak)
- Value
- Approximately 8 hours
Parameter
Elimination half-life
- Value
- 9.2 days (216 hours)
Parameter
Active metabolite half-life
- Value
- 16 days (384 hours); NS2360 (N-desmethyl metabolite)
Parameter
Metabolite exposure
- Value
- 31-34% of parent drug AUC at steady state
Parameter
Time to steady state
- Value
- 5-6 weeks with daily dosing
Parameter
Total clearance duration
- Value
- Approximately 46 days
Parameter
Primary metabolism
- Value
- CYP3A4-mediated N-oxidative dealkylation
Parameter
Renal clearance
- Value
- Minimal; 15-20% of total clearance
Parameter
Bioavailability
- Value
- Incomplete; variable absorption with potential food effects
Parameter
Route
- Value
- Oral only
The extended half-life results in significant accumulation with daily dosing. Steady-state plasma concentrations are substantially higher than single-dose levels, which has direct implications for both efficacy and adverse event profiles [2][8]. The primary active metabolite NS2360 (desalkyl metabolite) is formed via CYP3A4-mediated N-dealkylation and contributes to the pharmacological effect, with its own 16-day half-life further extending the compound's biological activity window [2].
Research & Clinical Evidence
Obesity and Weight Loss
The Basics
The strongest evidence for tesofensine comes from a large Phase 2 trial published in The Lancet in 2008, one of the most respected medical journals in the world. The study enrolled 203 obese adults and tested three different doses over 24 weeks. All participants followed a mild calorie-reduction diet.
The results were striking: the 0.5 mg dose produced 9.2% body weight loss, and the 1.0 mg dose produced 10.6%. For context, the placebo group (diet only) lost just 2%. At the time, this roughly doubled the performance of every other prescription weight loss medication on the market.
Importantly, the weight loss was primarily fat. Body composition scans showed that participants preserved their lean muscle mass while losing fat tissue, a pattern that is considered favorable compared to many weight loss approaches where significant muscle is lost alongside fat.
The weight loss also came with improvements in metabolic health markers: better triglyceride levels, improved insulin sensitivity, and reduced waist circumference.
However, transparency requires noting that The Lancet published an "expression of concern" about this study in 2013, related to questions about the completeness of adverse event reporting. The efficacy data itself was not challenged, but the safety reporting may have been incomplete.
The Science
The Phase 2b TIPO-1 trial (NCT00394667), published by Astrup et al. in The Lancet (2008), is the principal efficacy dataset for tesofensine in obesity [1]. The randomized, double-blind, placebo-controlled study enrolled 203 obese adults (BMI 30-40 kg/m2) across multiple centers in Denmark.
Dose
Placebo
- Mean Weight Loss
- -2.0%
- Placebo-Subtracted
- --
- p-value
- --
Dose
0.25 mg
- Mean Weight Loss
- -4.5%
- Placebo-Subtracted
- -2.5%
- p-value
- --
Dose
0.5 mg
- Mean Weight Loss
- -9.2%
- Placebo-Subtracted
- -7.2%
- p-value
- <0.0001
Dose
1.0 mg
- Mean Weight Loss
- -10.6%
- Placebo-Subtracted
- -8.6%
- p-value
- <0.0001
DEXA body composition analysis confirmed fat mass as the predominant component of weight loss with relative lean mass preservation. Quality of life measures (physical functioning, self-esteem, sexual life) improved significantly in the 0.5 mg and 1.0 mg groups [1].
A companion metabolic study by Sjodin et al. (2010) using respiratory chambers in 32 overweight men demonstrated that tesofensine 0.5 mg increased 24-hour energy expenditure by 6.1% and enhanced fat oxidation versus placebo over 14 days [12]. Gilbert et al. (2012) confirmed sustained reductions in subjective hunger ratings, increased fullness, and decreased prospective food consumption from the first two weeks through the 24-week treatment period [13].
An expression of concern was published by The Lancet in 2013 regarding potential under-reporting of adverse events in the original trial [14]. The efficacy findings have not been retracted or challenged.
Neurological Research (Parkinson's Disease)
The Basics
Before its pivot to obesity, tesofensine was tested in Parkinson's disease patients. While the compound did not prove effective enough for motor symptoms to continue development in that direction, these early trials provided valuable safety data and were where the weight loss observation first emerged.
The Science
Hauser et al. (2007) conducted a randomized trial of tesofensine in early Parkinson's disease at doses of 0.25, 0.5, and 1.0 mg [4]. The ADVANS study (Rascol et al., 2008) evaluated tesofensine in advanced Parkinson's disease with motor fluctuations [5]. Neither trial met primary motor function endpoints, but consistent, dose-dependent weight loss across both studies prompted the obesity indication pivot.
Appetite and Neurocircuit Mechanisms
The Basics
Research has gone beyond simply showing that tesofensine works and has started explaining why it works at a fundamental brain level. A 2024 study identified the specific type of brain cells that tesofensine quiets to reduce appetite, providing a clearer picture of its targeted action.
The Science
Perez et al. (2024) employed optogenetic and chemogenetic techniques to demonstrate that tesofensine specifically silences GABAergic neurons in the lateral hypothalamus, a neural population that actively promotes feeding behavior [7]. This finding localizes the anorexigenic mechanism beyond diffuse monoamine enhancement to a defined circuit element. In diet-induced obese rodent models, the compound showed amplified efficacy in obese versus lean subjects, with reduced food intake independent of locomotor changes or taste aversion [10].
Biomarker Evidence Matrix
The following matrix scores tesofensine across relevant biomarker categories. Evidence Strength reflects the quality of published research data. Reported Effectiveness reflects community-reported outcomes from the sentiment analysis.
Category
Fat Loss
- Evidence Strength
- 8/10
- Reported Effectiveness
- 8/10
- Summary
- Phase 2 trial demonstrated 9-10.6% body weight loss predominantly from fat mass. Community reports consistently describe significant fat loss.
Category
Weight Management
- Evidence Strength
- 8/10
- Reported Effectiveness
- 7/10
- Summary
- Strong dose-dependent weight reduction data from Phase 2 trial. Community reports positive but limited long-term maintenance data.
Category
Appetite & Satiety
- Evidence Strength
- 9/10
- Reported Effectiveness
- 9/10
- Summary
- Robust clinical evidence of appetite suppression (Gilbert et al., 2012). Community reports overwhelmingly confirm strong appetite reduction.
Category
Food Noise
- Evidence Strength
- 4/10
- Reported Effectiveness
- 8/10
- Summary
- Minimal formal clinical study of food noise specifically, but pharmacological profile supports it. Community reports strongly positive for food noise reduction.
Category
Energy Levels
- Evidence Strength
- 6/10
- Reported Effectiveness
- 6/10
- Summary
- Metabolic chamber study showed 6.1% increase in energy expenditure. Community reports are mixed: some report calm drive, others feel wired.
Category
Sleep Quality
- Evidence Strength
- 5/10
- Reported Effectiveness
- 3/10
- Summary
- Insomnia reported as common side effect in clinical trials (15-20%). Community reports confirm sleep disruption as a frequent trade-off.
Category
Focus & Mental Clarity
- Evidence Strength
- 3/10
- Reported Effectiveness
- 7/10
- Summary
- No dedicated cognitive trials. Original Parkinson's/Alzheimer's research showed limited cognitive endpoints. Community reports frequently positive for focus.
Category
Mood & Wellbeing
- Evidence Strength
- 4/10
- Reported Effectiveness
- 5/10
- Summary
- Pharmacological profile suggests mood modulation. Community reports are genuinely split: improved mood for some, irritability for others.
Category
Anxiety
- Evidence Strength
- 4/10
- Reported Effectiveness
- 3/10
- Summary
- Known noradrenergic mechanism supports anxiogenic potential. Community reports confirm anxiety increase in susceptible individuals.
Category
Motivation & Drive
- Evidence Strength
- 3/10
- Reported Effectiveness
- 7/10
- Summary
- Dopaminergic mechanism supports motivation enhancement. No dedicated clinical study but community reports frequently positive.
Category
Emotional Regulation
- Evidence Strength
- 3/10
- Reported Effectiveness
- 3/10
- Summary
- Phase 2 trial noted mood disturbances at higher doses. Community reports include irritability and emotional dysregulation.
Category
Heart Rate & Palpitations
- Evidence Strength
- 8/10
- Reported Effectiveness
- 2/10
- Summary
- Well-documented in clinical trials: 7-8 bpm increase at therapeutic doses. Community consistently reports elevated heart rate.
Category
Digestive Comfort
- Evidence Strength
- 5/10
- Reported Effectiveness
- 4/10
- Summary
- Dry mouth (30-35%), constipation (10-15%) in clinical trials. Community reports manageable GI effects.
Category
Cravings & Impulse Control
- Evidence Strength
- 5/10
- Reported Effectiveness
- 7/10
- Summary
- Dopaminergic mechanism supports craving reduction. Community reports positive for food cravings and preliminary interest in alcohol craving reduction.
Category
Side Effect Burden
- Evidence Strength
- 7/10
- Reported Effectiveness
- 4/10
- Summary
- Well-characterized side effect profile from Phase 2 data. Community reports wide individual variation in tolerability.
Category
Treatment Adherence
- Evidence Strength
- 5/10
- Reported Effectiveness
- 6/10
- Summary
- Oral dosing is a significant adherence advantage over injectables. Community reports high compliance for responders.
Benefits & Potential Effects
The Basics
The most well-established benefit of tesofensine is appetite suppression and weight loss. In clinical studies, it produced meaningful reductions in body weight while preserving muscle mass. For many people, the most noticeable effect is a significant quieting of the constant mental noise around food, making it easier to stick with a calorie-controlled diet without the usual willpower battle.
Beyond appetite, the dopaminergic component may contribute to improved motivation and focus during caloric restriction, a period when many people experience mental fog and low drive. Some users report feeling more energized and mentally clear, although this varies between individuals.
The metabolic benefits extend beyond the scale. Research participants saw improvements in triglyceride levels, insulin sensitivity, and waist circumference. The preferential reduction of visceral fat (the deep abdominal fat surrounding organs, which is the most metabolically dangerous type) is particularly noteworthy.
The oral delivery route is a practical advantage. Unlike GLP-1 receptor agonists that require weekly injections, tesofensine is taken as a daily pill, which may improve long-term adherence for people who are averse to injections.
The Science
Clinical data from the Phase 2b TIPO-1 trial supports the following benefit profile [1]:
Body composition: DEXA-confirmed fat mass reduction with relative lean mass preservation. The 0.5 mg dose produced approximately 6.7 kg of fat loss over 24 weeks [1].
Metabolic parameters: Significant improvements in triglyceride levels, VLDL cholesterol, fasting insulin, and insulin sensitivity measures [1]. Waist circumference reduction was dose-dependent and statistically significant at the 0.5 mg and 1.0 mg doses.
Energy expenditure: Sjodin et al. (2010) demonstrated a 6.1% increase in 24-hour energy expenditure and enhanced fat oxidation in a controlled metabolic chamber study at the 0.5 mg dose [12].
Appetite regulation: Gilbert et al. (2012) showed sustained reductions in subjective hunger ratings, increased postprandial fullness, and decreased prospective food consumption, with effects appearing within the first two weeks and maintained through 24 weeks [13].
Quality of life: The TIPO-1 trial reported statistically significant improvements in physical functioning, self-esteem, and sexual life scores at the 0.5 mg and 1.0 mg doses [1].
Abuse liability: A formal abuse potential study (Schoedel et al., 2010) demonstrated significantly lower subjective effects compared to d-amphetamine at comparable doses, consistent with the moderate (30-50%) dopamine transporter occupancy at therapeutic doses [8][9].
The benefits outlined above span multiple body systems, and your experience will be uniquely yours. Rather than guessing which effects are attributable to this compound versus other factors in your life, Doserly helps you log specific outcomes alongside your protocol details, building a clear picture of what's changing and when.
Over weeks and months, this creates something more useful than any anecdotal report: your own evidence-based record of how this compound affects you personally, at your specific dose, within the context of your full health protocol. When it's time to decide whether to continue, adjust, or discontinue, you have real data to inform that conversation with your healthcare provider.
Connect protocol changes to labs and health markers.
Doserly can keep lab results, biomarkers, symptoms, and dose history close together so follow-up conversations have better context.
Insights
Labs and trends

Doserly organizes data; it does not diagnose or interpret labs for you.
Side Effects & Safety Considerations
The Basics
Tesofensine has a well-defined side effect profile from its Phase 2 clinical trial. The most common effects are dry mouth (roughly one in three people), insomnia (roughly one in five), and constipation (roughly one in seven). These are generally mild and manageable.
The more important safety consideration is cardiovascular. Tesofensine consistently raises resting heart rate by an average of 7-8 beats per minute at the 0.5 mg dose. While this sounds modest, it was the primary safety signal that complicated the compound's path to market, particularly given the history of sibutramine (a similar type of compound that was pulled from the market in 2010 after being linked to cardiovascular events in high-risk patients).
Mood and psychiatric effects deserve attention. Because tesofensine affects the same neurotransmitter systems targeted by antidepressants and stimulants, some individuals experience mood changes, increased anxiety, or irritability. These effects appear more common at the 1.0 mg dose and in individuals with existing mood sensitivities.
Drug interactions are a serious concern. Tesofensine should not be combined with SSRIs, SNRIs, MAO inhibitors, or stimulant medications due to the risk of serotonin syndrome or excessive cardiovascular stimulation. Anyone considering this compound should review their current medication list with a healthcare provider.
The long half-life means that if a side effect develops, it will persist for days to weeks even after the compound is stopped. This is an important consideration before starting.
The Science
Phase 2 adverse event data at the 0.5 mg dose (most commonly referenced) [1]:
Side Effect
Dry mouth
- Incidence
- 30-35%
- Mechanism
- Noradrenergic and serotonergic activity
Side Effect
Insomnia
- Incidence
- 15-20%
- Mechanism
- Dopaminergic and noradrenergic stimulation
Side Effect
Constipation
- Incidence
- 10-15%
- Mechanism
- Reduced GI motility from sympathetic activation
Side Effect
Hard stools
- Incidence
- 10-15%
- Mechanism
- Related to constipation mechanism
Side Effect
Elevated heart rate
- Incidence
- Mean +7.4 bpm
- Mechanism
- Noradrenergic-mediated sympathetic activation
Cardiovascular profile: Mean heart rate increased 7.4 bpm at 0.5 mg and 8.1 bpm at 1.0 mg versus placebo [1]. Mean systolic blood pressure showed small, non-significant increases; diastolic blood pressure was largely unchanged. Individual responses varied considerably, with some participants experiencing clinically significant tachycardia.
The cardiovascular profile bears mechanistic similarity to sibutramine, a dual serotonin-norepinephrine reuptake inhibitor withdrawn from the market in 2010 after the SCOUT trial demonstrated increased cardiovascular events in high-risk populations [15]. This comparison, while not direct evidence against tesofensine, has shaped the regulatory approach to the compound.
Psychiatric effects: Nathan et al. (2011) reviewed neuropsychiatric adverse effects of centrally acting anti-obesity drugs including tesofensine, noting mood elevation, anxiety, and depressive symptoms in the pharmacological class [16]. Mood-related adverse events were more frequent in the 1.0 mg group than the 0.5 mg group in the TIPO-1 trial [1].
Contraindications and drug interactions:
- MAO inhibitors: contraindicated due to risk of serotonin syndrome and hypertensive crisis
- SSRIs/SNRIs: risk of serotonin syndrome with concurrent serotonin reuptake inhibition
- Stimulants (amphetamines, methylphenidate): additive cardiovascular stimulation and monoaminergic effects
- Bupropion: combined dopamine/norepinephrine reuptake inhibition may increase seizure and cardiac risk
Side effect profiles are most useful when you can compare them against your own experience in real time. Doserly lets you log symptoms, severity, and timing alongside your dosing data, creating a side-by-side view of your protocol and your body's response.
This kind of systematic tracking catches things that memory alone misses. A subtle mood shift that began three days after a dose increase. Sleep disruption that correlates with evening administration. These patterns become visible when the data is laid out on a timeline, and they give your healthcare provider actionable information rather than vague concerns. Early detection of emerging side effects means earlier intervention.
Capture changes while they are still fresh.
Log symptoms, energy, sleep, mood, and other observations alongside protocol events so patterns do not live only in memory.
Trend view
Symptom timeline

Symptom tracking is informational and should be interpreted with a qualified clinician.
Dosing Protocols
The Basics
All dosing information for tesofensine comes from clinical trials. There is no FDA-approved dosing protocol because the compound has never received regulatory approval.
Three dose levels have been studied: 0.25 mg, 0.5 mg, and 1.0 mg, all taken once daily by mouth. The 0.5 mg dose is widely regarded as the best balance of effectiveness and tolerability. It produced clinically meaningful weight loss (9.2% over 24 weeks) while maintaining a manageable side effect profile.
The 0.25 mg dose showed modest effects and is sometimes used as a starting dose for the first 2-4 weeks to assess individual tolerance before potentially moving to 0.5 mg. The 1.0 mg dose produced slightly more weight loss but with a notably higher rate of side effects, particularly elevated heart rate and mood disturbances, and the additional benefit over 0.5 mg was relatively small.
Morning dosing is the standard practice, primarily to minimize insomnia risk. Because the half-life is approximately 9 days, missing a single dose has minimal impact on blood levels, but this also means that dose adjustments take several weeks to fully take effect.
Community protocols typically use 12-24 week treatment periods followed by 4-6 weeks off. The extended washout period reflects the compound's long half-life and the need for neurochemical recovery.
The Science
Clinical trial dosing from the Phase 2b TIPO-1 trial [1]:
Dose
0.25 mg daily
- Efficacy (24-week weight loss)
- -4.5% (modest; below clinically meaningful threshold)
- Tolerability
- Favorable side effect profile
Dose
0.5 mg daily
- Efficacy (24-week weight loss)
- -9.2% (optimal risk-benefit)
- Tolerability
- Manageable; most commonly referenced dose
Dose
1.0 mg daily
- Efficacy (24-week weight loss)
- -10.6% (marginal improvement over 0.5 mg)
- Tolerability
- Higher incidence of adverse events
All doses were administered as oral capsules once daily with a mildly hypocaloric diet (300 kcal/day deficit) [1]. The long half-life (~220 hours) means steady-state concentrations are reached after approximately 5-6 weeks of consistent daily dosing [2][8]. Dose adjustments require a minimum of 4-6 weeks to assess the full effect at each dose level.
What to Expect
Weeks 1-2: Initial appetite reduction begins for most individuals, though the compound has not yet reached full steady-state concentration. Dry mouth may be noticeable. Some people report increased alertness or a mild stimulatory sensation. Sleep quality may be affected, particularly if dosing occurs later in the day. Weight loss during this period is modest, typically 1-2 kg, and reflects both reduced calorie intake and early metabolic effects.
Weeks 2-4: Appetite suppression becomes more pronounced as plasma levels continue to build. Food noise and cravings typically diminish significantly. Weight loss accelerates, with most people seeing clear progress on the scale. Cardiovascular effects (heart rate elevation) may become apparent during this period. Morning dosing routines are usually well established.
Weeks 4-8 (approaching steady state): The compound reaches or approaches full steady-state concentration around weeks 5-6. Appetite suppression and metabolic effects are at their peak. Weight loss typically reaches 5-8% of body weight for responders on the 0.5 mg dose. Metabolic markers (fasting glucose, triglycerides) may begin showing improvement. Side effects that are going to develop have typically manifested by this point.
Weeks 8-16: Continued weight loss, though the rate may slow as the body adjusts to a lower weight. Total weight loss typically reaches 8-12% in responders. Some individuals report that appetite suppression becomes slightly less intense over time, though it generally remains meaningful throughout the treatment period. This is a good assessment point to evaluate whether the compound is delivering sufficient benefit relative to any side effects experienced.
Weeks 16-24+: The clinical trial endpoint. Weight loss continues for many individuals. Body composition improvements (reduced waist circumference, improved metabolic markers) are typically well-established. This is the decision point for whether to continue, extend, or cycle off.
Post-cessation: Due to the extremely long half-life, effects (both positive and negative) persist for weeks after the last dose. Full clearance takes approximately 46 days. Appetite will gradually return to baseline during this period. Community protocols suggest a minimum 4-6 week washout before considering another cycle.
Timelines are useful benchmarks, but they mean more when you're tracking your own progress against them. Doserly lets you log daily observations alongside your protocol data, creating a personal timeline that runs parallel to the general expectations above.
When you reach the 4-week or 8-week assessment points, you'll have more than a feeling to work with. You'll have a documented record of how each week progressed, what changed, and when. This makes protocol decisions concrete: whether to extend a cycle, adjust a dose, or try a different approach, the data is there to support the conversation with your healthcare provider rather than relying on recall.
Turn symptom and safety notes into a clearer timeline.
Doserly helps you log doses, symptoms, and safety observations side by side so patterns are easier to discuss with a qualified clinician.
Pattern view
Logs and observations

Pattern visibility is informational and should be reviewed with a clinician.
Interaction Compatibility
Potentially Complementary
- Retatrutide: GLP-1/GIP/glucagon triple agonist. Different mechanism (incretin pathway vs. central monoamine modulation). Theoretical complementarity, but no combination data exists. Cardiovascular monitoring would be essential.
- AOD-9604: HGH fragment targeting lipolysis. Non-overlapping mechanism. Community sources suggest pairing for enhanced fat mobilization.
- MOTS-C: Mitochondrial-derived metabolic peptide. Community sources suggest pairing for enhanced metabolic activity.
- 5-Amino-1MQ: NNMT inhibitor targeting fat cell metabolism. Non-overlapping mechanism.
- SLU-PP-332: Exercise mimetic. Community sources suggest pairing for metabolic enhancement.
- NAD+: Cellular energy cofactor. Non-overlapping mechanism.
- SS-31: Mitochondrial-targeted peptide. Community sources suggest pairing for cellular energy support.
Use Caution
- Semaglutide: GLP-1 agonist. Completely different mechanism. Theoretical synergy for additive appetite suppression, but no safety data for the combination exists. The cardiovascular effects of tesofensine may counteract the cardiovascular benefits of GLP-1 agonists.
- Tirzepatide: GLP-1/GIP dual agonist. Same caution as semaglutide.
- Cagrilintide: Amylin analog. Additive appetite suppression effects without combination safety data.
- MK-677: Growth hormone secretagogue. May increase appetite, potentially counteracting tesofensine's primary mechanism.
Not Recommended
- SSRIs/SNRIs (prescription medications): Risk of serotonin syndrome due to combined serotonin reuptake inhibition
- MAO inhibitors (prescription medications): Life-threatening serotonin syndrome and hypertensive crisis risk
- Stimulant medications (amphetamines, methylphenidate): Additive cardiovascular and monoaminergic effects
- Bupropion: Combined dopamine/norepinephrine reuptake inhibition increases seizure and cardiac risk
- High caffeine intake: Additive cardiovascular stimulation and insomnia risk
Administration Guide
Tesofensine is administered orally as a capsule or tablet. No reconstitution, mixing, or injection is required, which makes administration straightforward compared to most peptide compounds.
Materials required:
- Tesofensine capsules/tablets in the desired dose (typically 0.25 mg or 0.5 mg)
- Water for swallowing
Timing considerations: Morning administration is the standard practice, as this minimizes the risk of insomnia. Some sources suggest taking it with food, though the clinical trials did not specify strict food requirements. Consistency in timing is more important than the specific time chosen, given the long half-life.
Monitoring: Resting heart rate and blood pressure should be logged daily, ideally at the same time each day, for at least the first week after starting and the first week after any dose adjustment. An ECG is advisable for individuals with cardiac history or if notable heart rate or blood pressure changes develop.
Post-administration care: No immediate post-dose monitoring is typically needed. Watch for the development of insomnia (may take several days to manifest due to accumulation), dry mouth (maintain hydration), and cardiovascular changes (log vitals consistently). If palpitations, sustained blood pressure elevation (>10 mmHg above baseline), severe insomnia unresponsive to timing adjustment, or signs of serotonin syndrome (agitation, fever, muscle rigidity) develop, contact a healthcare provider immediately.
Supplies & Planning
Tesofensine's oral administration makes supply planning considerably simpler than injectable compounds.
Typical supplies:
- Tesofensine capsules/tablets in the appropriate dose
- Blood pressure monitor (home use; automatic cuff recommended)
- Heart rate monitor or fitness tracker with resting HR tracking
- A log or tracking app for daily vitals
Quality considerations: Tesofensine is not FDA-approved and is available only through compounding pharmacies or research compound vendors. Product quality and accurate dosing can vary significantly between sources. A Certificate of Analysis (CoA) with third-party testing verification is advisable to confirm accurate dosing (particularly important given the narrow dose range of 0.25-1.0 mg) and compound purity.
Planning: For a typical 12-week cycle at 0.5 mg daily, approximately 84 doses would be needed. Account for the 4-6 week washout period before considering another cycle.
Storage & Handling
Tesofensine is generally stable at room temperature, which simplifies storage compared to most peptide compounds that require refrigeration.
Lyophilized/powder form:
- Store at -20C (-4F) for long-term storage (3+ years of stability)
- Room temperature (20-25C / 68-77F) is acceptable for shorter-term storage
- Protect from moisture (the compound is hygroscopic)
- Protect from direct light
- Keep in original sealed packaging with desiccant if available
Capsule/tablet form:
- Room temperature storage (20-25C / 68-77F)
- Protect from moisture and light
- No refrigeration required
- Keep container tightly closed
Handling notes: The hygroscopic nature of the compound means it absorbs moisture from the air. Minimize exposure to humid conditions and seal containers promptly after use.
Lifestyle Factors
Diet: A high-protein diet (1.6-2.2 g/kg body weight) is advisable to safeguard lean muscle mass during the caloric restriction that tesofensine facilitates. The compound's appetite-suppressing effects can significantly reduce food intake, making intentional attention to protein and nutrient density important to avoid inadvertent malnutrition during aggressive calorie restriction.
Exercise: Regular physical activity supports cardiovascular health and helps manage the potential heart rate and blood pressure effects of tesofensine. Both resistance training (to preserve lean mass during weight loss) and moderate cardiovascular exercise are beneficial. Monitoring heart rate during exercise is advisable, particularly during the first few weeks.
Sleep: Ensure 7-9 hours of quality sleep. Morning dosing helps minimize insomnia risk. Limiting caffeine intake (particularly afternoon and evening) is important, as the combination of tesofensine's noradrenergic effects and caffeine can compound sleep disruption. If insomnia persists despite morning dosing, this should be discussed with a healthcare provider.
Hydration: Increased water intake helps manage dry mouth, the most common side effect. Electrolyte attention is important, as reduced food intake can decrease electrolyte consumption.
Caffeine: Many sources recommend moderating caffeine intake while using tesofensine. The noradrenergic stimulation from both compounds can be additive for cardiovascular effects and sleep disruption.
Monitoring: Regular vitals logging (heart rate, blood pressure) provides early detection of cardiovascular changes. Lab work (fasting glucose, HbA1c, lipid panel, liver enzymes) at baseline and periodically during use provides objective metabolic data.
Regulatory Status & Research Classification
United States (FDA): Tesofensine is not approved for any indication. It has not completed Phase 3 clinical trials for obesity. The compound is available only through compounding pharmacies (in a legal gray area) and as a research chemical. There is no IND application currently active for general obesity.
Saniona/Tesomet development: Saniona A/S (Denmark) holds the rights to tesofensine and has developed Tesomet, a fixed-dose combination of tesofensine (0.5 mg) with metoprolol (a beta-1 selective blocker at approximately 100:1 ratio) designed to counteract the heart rate increase. Tesomet received FDA Orphan Drug Designation for Prader-Willi Syndrome (PWS) in March 2021. Phase 2a trials in adult PWS patients showed meaningful reductions in body weight and hyperphagia with acceptable tolerability. As of early 2026, Saniona announced approval to initiate the second part of its Phase 2a study in adolescent PWS patients.
Canada (Health Canada): Not approved. No DIN or NPN status.
United Kingdom (MHRA): Not approved or classified.
Australia (TGA): Not scheduled or approved.
European Union (EMA): No marketing authorization. Saniona (Danish company) holds development rights but has not submitted for EMA approval.
WADA status: Not listed specifically, but compounds that modify neurotransmitter reuptake may fall under prohibited stimulant categories depending on classification. Athletes should verify current status with their sport's governing body.
Key clinical trials:
- NCT00394667 (TIPO-1): Phase 2b, obesity, completed 2008 [1]
- NCT03149445: Phase 2a, Tesomet in Prader-Willi Syndrome (adults), completed
- NCT05198362: Phase 2b, Tesomet in PWS, voluntarily suspended March 2022 (financial), potential restart
Why development stalled:
- NeuroSearch A/S (original developer) entered financial difficulties before completing Phase 3
- Post-sibutramine regulatory climate demands extensive cardiovascular outcome data for obesity drugs
- Competition from approved GLP-1 drugs reduced commercial interest
- The Lancet expression of concern undermined confidence in the primary dataset
- Heart rate increase (~7-8 bpm) made regulators cautious
Regulatory status changes frequently. Always verify the current legal status of any compound in your specific country or jurisdiction before making any decisions.
FAQ
What is tesofensine?
Tesofensine is a synthetic small-molecule compound (not a peptide) that functions as a triple monoamine reuptake inhibitor, blocking the recycling of dopamine, norepinephrine, and serotonin in the brain. It was originally developed for Parkinson's disease but was redirected to obesity research after weight loss was observed in early trials.
Is tesofensine FDA-approved?
No. Tesofensine has never been approved by the FDA, EMA, or any major regulatory agency for any indication. It has not completed Phase 3 clinical trials. It is available only as a research compound or through compounding pharmacies.
What dose was used in clinical trials?
Phase 2 trials tested 0.25 mg, 0.5 mg, and 1.0 mg once daily. Based on available data, the 0.5 mg dose is most frequently referenced as providing the best balance of weight loss efficacy and tolerability, producing approximately 9.2% body weight loss over 24 weeks.
How does tesofensine compare to semaglutide or tirzepatide?
They work through entirely different mechanisms. Tesofensine targets central neurotransmitters while GLP-1 drugs work through gut hormone pathways. GLP-1 drugs have larger Phase 3 trials, FDA approval, and demonstrated cardiovascular benefits. Tesofensine has Phase 2 data only, no approval, and a cardiovascular concern (heart rate increase). However, tesofensine is oral (versus injectable), has minimal GI side effects, and may address reward-driven overeating through dopamine modulation in ways that GLP-1 drugs do not.
How long does it take to work?
Initial appetite reduction may begin within the first 1-2 weeks. However, due to the long half-life (approximately 9 days), full steady-state blood levels are not reached until approximately 5-6 weeks of daily dosing. Maximum effects develop gradually over this period.
What are the main side effects?
Based on Phase 2 trial data, the most commonly reported side effects at the 0.5 mg dose include dry mouth (30-35%), insomnia (15-20%), constipation (10-15%), and elevated heart rate (mean increase of approximately 7.4 bpm). Cardiovascular monitoring is considered essential by most sources.
Can tesofensine be combined with GLP-1 drugs?
No clinical studies have evaluated this combination. While the different mechanisms suggest theoretical complementarity, the safety profile of the combination is unknown. The cardiovascular effects of tesofensine (increased heart rate) could potentially counteract the cardiovascular benefits demonstrated by GLP-1 agonists.
Is tesofensine a stimulant? Is it addictive?
Tesofensine occupies approximately 30-50% of dopamine transporters at therapeutic doses, which is below the threshold typically associated with euphoric or reinforcing effects. A formal abuse liability study found its subjective effects were significantly lower than d-amphetamine. While it is not classified as a controlled substance in most jurisdictions, it does affect the same neurotransmitter systems as stimulants and should be treated with appropriate caution.
Can tesofensine help with food addiction or emotional eating?
The dopaminergic component of tesofensine's mechanism is theoretically relevant to reward-driven eating behaviors. Animal studies show that it reverses low forebrain dopamine levels associated with diet-induced obesity. Community reports frequently mention reduced food cravings and "food noise." However, tesofensine has not been specifically studied for food addiction or binge eating disorder in any clinical trial.
Sources & References
Clinical Trials
[1] Astrup A, Madsbad S, Breum L, Jensen TJ, Kroustrup JP, Larsen TM. Effect of tesofensine on bodyweight loss, body composition, and quality of life in obese patients: a randomised, double-blind, placebo-controlled trial. Lancet. 2008;372(9653):1906-1913. https://pubmed.ncbi.nlm.nih.gov/18950853/
[4] Hauser RA, Salin L, Juhel N, Konyago VL. Randomized trial of the triple monoamine reuptake inhibitor NS 2330 (tesofensine) in early Parkinson's disease. Mov Disord. 2007;22(3):359-365. https://pubmed.ncbi.nlm.nih.gov/17149725/
[5] Rascol O, Poewe W, Lees A, et al. Tesofensine (NS 2330), a monoamine reuptake inhibitor, in patients with advanced Parkinson disease and motor fluctuations: the ADVANS Study. Arch Neurol. 2008;65(5):577-583. https://pubmed.ncbi.nlm.nih.gov/18474731/
Metabolic and Appetite Studies
[12] Sjodin A, Gasteyger C, Nielsen AL, et al. The effect of the triple monoamine reuptake inhibitor tesofensine on energy metabolism and appetite in overweight and moderately obese men. Int J Obes. 2010;34(11):1634-1643. https://pubmed.ncbi.nlm.nih.gov/20479765/
[13] Gilbert JA, Gasteyger C, Raben A, Meier DH, Astrup A, Sjodin A. The effect of tesofensine on appetite sensations. Obesity. 2012;20(3):553-561. https://pubmed.ncbi.nlm.nih.gov/21720440/
Pharmacology and Imaging
[2] Astrup A, Meier DH, Mikkelsen BO, Villumsen JS, Larsen TM. Weight loss produced by tesofensine in patients with Parkinson's or Alzheimer's disease. Obesity. 2008;16(6):1363-1369. https://pubmed.ncbi.nlm.nih.gov/18356831/
[3] Doggrell SA. Tesofensine: a novel potent weight loss medicine. Expert Opin Investig Drugs. 2009;18(7):1043-1046. https://pubmed.ncbi.nlm.nih.gov/19548858/
[8] Appel L, Bergstrom M, Buus Lassen J, Langstrom B. Tesofensine, a novel triple monoamine re-uptake inhibitor with anti-obesity effects: dopamine transporter occupancy as measured by PET. Eur Neuropsychopharmacol. 2014;24(2):251-261. https://pubmed.ncbi.nlm.nih.gov/24239329/
[9] Schoedel KA, et al. Abuse potential assessment of tesofensine compared to d-amphetamine in recreational stimulant users. 2010.
Preclinical and Mechanistic
[7] Perez CI, Luis-Islas J, Lopez A, et al. Tesofensine, a novel antiobesity drug, silences GABAergic neurons in the lateral hypothalamus. PLoS One. 2024;19(4):e0300544. https://pubmed.ncbi.nlm.nih.gov/38656972/
[10] Hansen HH, et al. Tesofensine induces appetite suppression and weight loss with superior effects in diet-induced obese rats. 2013. https://pubmed.ncbi.nlm.nih.gov/23932919/
[11] Van de Giessen EM, et al. Tesofensine reduces food intake and body weight in obese rats while decreasing striatal D2/D3 receptor availability. 2012.
Safety Reviews
[6] The Peptide Catalog. Tesofensine for Weight Loss: How It Works. 2026. (Non-primary source; used for regulatory history context only)
[14] The Lancet. Expression of Concern regarding Astrup et al. 2008. Published 2013.
[15] James WP, et al. Effect of sibutramine on cardiovascular outcomes in overweight and obese subjects. N Engl J Med. 2010;363(10):905-917. (SCOUT trial)
[16] Nathan PJ, et al. The neuropsychiatric adverse effects of centrally acting antiobesity drugs. CNS Neurosci Ther. 2011;17(5):490-505.
Related Peptide Guides
- Semaglutide — GLP-1 receptor agonist; FDA-approved for weight management; different mechanism (incretin pathway)
- Tirzepatide — Dual GLP-1/GIP agonist; FDA-approved for weight management; stronger weight loss data
- Retatrutide — Triple GLP-1/GIP/glucagon agonist; strongest weight loss data in trials
- Cagrilintide — Amylin analog; appetite suppression through different pathway
- AOD-9604 — HGH fragment targeting lipolysis; community-paired with tesofensine
- 5-Amino-1MQ — NNMT inhibitor; metabolic fat loss compound
- MOTS-C — Mitochondrial-derived metabolic peptide; exercise mimetic
- SLU-PP-332 — Exercise mimetic; metabolic enhancement
- Tesamorelin — FDA-approved GHRH analog for visceral fat reduction; sometimes stacked in metabolic protocols
- Mazdutide — GLP-1/glucagon dual agonist; emerging weight loss compound
- Survodutide — GLP-1/glucagon dual agonist; emerging weight loss compound
- Orforglipron — Oral GLP-1 agonist; another oral alternative for weight management
- MK-677 — Growth hormone secretagogue; note potential appetite increase may counteract tesofensine
- Dihexa / Methylene Blue / Tesofensine blend — Available as combination on the platform